Download Your Migraine Diary
Download Your Migraine Diary
Download Your Migraine Diary

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
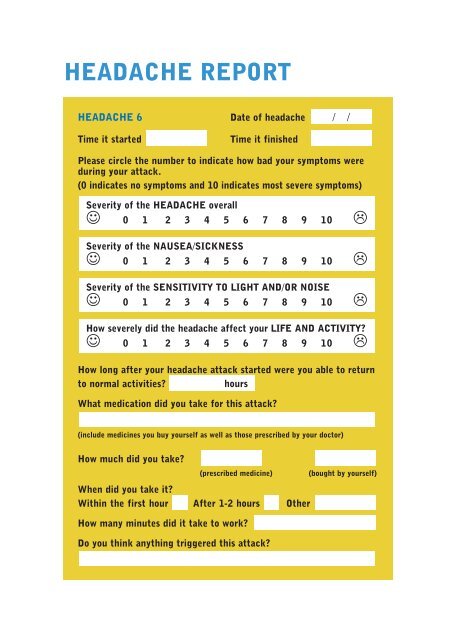
HEADACHE REPORT<br />
HEADACHE 6<br />
Time it started<br />
Date of headache<br />
Time it finished<br />
/ /<br />
Please circle the number to indicate how bad your symptoms were<br />
during your attack.<br />
(0 indicates no symptoms and 10 indicates most severe symptoms)<br />
Severity of the HEADACHE overall<br />
☺ 0 1 2 3 4 5 6 7 8 9 10 ☹<br />
Severity of the NAUSEA/SICKNESS<br />
☺ 0 1 2 3 4 5 6 7 8 9 10 ☹<br />
Severity of the SENSITIVITY TO LIGHT AND/OR NOISE<br />
☺ 0 1 2 3 4 5 6 7 8 9 10 ☹<br />
How severely did the headache affect your LIFE AND ACTIVITY?<br />
☺ 0 1 2 3 4 5 6 7 8 9 10 ☹<br />
How long after your headache attack started were you able to return<br />
to normal activities?<br />
hours<br />
What medication did you take for this attack?<br />
(include medicines you buy yourself as well as those prescribed by your doctor)<br />
How much did you take?<br />
(prescribed medicine)<br />
(bought by yourself)<br />
When did you take it?<br />
Within the first hour After 1-2 hours Other<br />
How many minutes did it take to work?<br />
Do you think anything triggered this attack?