Preventing Avoidable Readmissions Driver Diagram
Preventing Avoidable Readmissions Driver Diagram
Preventing Avoidable Readmissions Driver Diagram

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
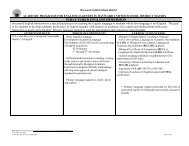
Primary <strong>Driver</strong>s Secondary <strong>Driver</strong>s Change Ideas<br />
Self-management skills • Enhance patients’/caregivers’ knowledge<br />
about the medications prescribed.<br />
• Enhance patients’/caregivers’ knowledge<br />
about their symptoms, red flags, and selfcare<br />
strategies.<br />
• Identify and address patients’ health literacy and<br />
activation levels.<br />
• Use Teach-back to validate patient understanding.<br />
•<br />
• Obtain an accurate home medication history from the patient and/or<br />
primary caregiver at admission.<br />
Educate patients/caregivers before discharge regarding all<br />
medications prescribed, the purpose of these medications,<br />
the means of obtaining them, and the instructions for taking<br />
them.<br />
• Provide clearly written medication instructions using health<br />
literacy concepts and culturally appropriate training<br />
materials.<br />
• Develop patient-centered educational tools that employ health literacy<br />
concepts to teach patients about their diagnosis and symptoms.<br />
• Train clinical staff on Teach-back using role play, and observe their<br />
technique in the field. Do they…<br />
o Use “I” statements when speaking with patients and<br />
caregivers? “To make sure I did a good job explaining<br />
your medications, can you tell me …?”<br />
o Validate patient and caregiver understanding of<br />
discharge instructions?<br />
Coordination of information along the care<br />
continuum<br />
• Create a patient-centered record.<br />
• Timely communication with members of the care<br />
team who are not hospital-based.<br />
•<br />
• Accurate medication reconciliation at<br />
admission, at any change in the level of care,<br />
and at discharge.<br />
• Evaluate best practices and resources and established<br />
tools such as the Project RED After Hospital Care Plan (AHCP) and<br />
Coleman Personal Health Record.<br />
• Determine which models will work in your organization.<br />
• Engage IT support for completing plans of care.<br />
• Determine where key information is to be stored and how it<br />
will be compiled to complete plans of care.<br />
• Obtain accurate information about patients’ primary care physicians<br />
at the time of admission.<br />
• Send completed discharge summaries to patients’ primary care<br />
physicians within 48 hours of discharge.<br />
• Use of a concise, standardized discharge transfer form.<br />
• Assign clear accountability for medication reconciliation and<br />
perform reconciliation at each transition of care; consider a home<br />
visit to educate patients/caregivers about their medications and to<br />
reconcile the medications in the patients’ homes.