Evaluation & Management of Adult Hypoglycemic Disorders
Evaluation & Management of Adult Hypoglycemic Disorders
Evaluation & Management of Adult Hypoglycemic Disorders

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
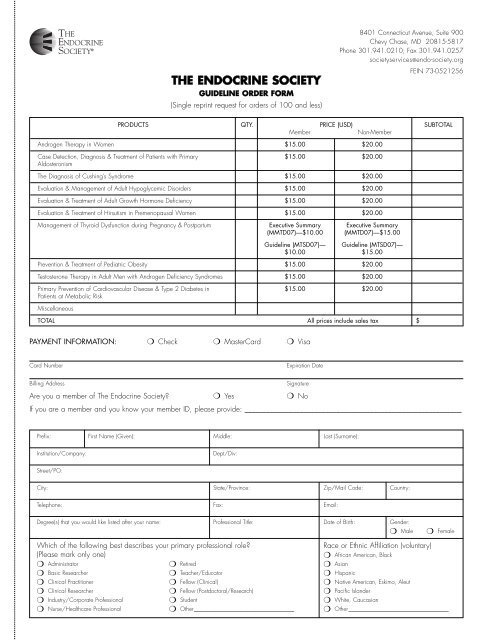
THE ENDOCRINE SOCIETY<br />
GUIDELINE ORDER FORM<br />
(Single reprint request for orders <strong>of</strong> 100 and less)<br />
8401 Connecticut Avenue, Suite 900<br />
Chevy Chase, MD 20815-5817<br />
Phone 301.941.0210; Fax 301.941.0257<br />
societyservices@endo-society.org<br />
FEIN 73-0521256<br />
PRODUCTS QTY. PRICE (USD) SUBTOTAL<br />
Member<br />
Non-Member<br />
Androgen Therapy in Women $15.00 $20.00<br />
Case Detection, Diagnosis & Treatment <strong>of</strong> Patients with Primary $15.00 $20.00<br />
Aldosteronism<br />
The Diagnosis <strong>of</strong> Cushing’s Syndrome $15.00 $20.00<br />
<strong>Evaluation</strong> & <strong>Management</strong> <strong>of</strong> <strong>Adult</strong> <strong>Hypoglycemic</strong> <strong>Disorders</strong> $15.00 $20.00<br />
<strong>Evaluation</strong> & Treatment <strong>of</strong> <strong>Adult</strong> Growth Hormone Deficiency $15.00 $20.00<br />
<strong>Evaluation</strong> & Treatment <strong>of</strong> Hirsutism in Premenopausal Women $15.00 $20.00<br />
<strong>Management</strong> <strong>of</strong> Thyroid Dysfunction during Pregnancy & Postpartum Executive Summary Executive Summary<br />
(MMTD07)—$10.00 (MMTD07)—$15.00<br />
Guideline (MTSD07)— Guideline (MTSD07)—<br />
$10.00 $15.00<br />
Prevention & Treatment <strong>of</strong> Pediatric Obesity $15.00 $20.00<br />
Testosterone Therapy in <strong>Adult</strong> Men with Androgen Deficiency Syndromes $15.00 $20.00<br />
Primary Prevention <strong>of</strong> Cardiovascular Disease & Type 2 Diabetes in $15.00 $20.00<br />
Patients at Metabolic Risk<br />
Miscellaneous<br />
TOTAL All prices include sales tax $<br />
PAYMENT INFORMATION: ❍ Check ❍ MasterCard ❍ Visa<br />
Card Number<br />
Expiration Date<br />
Billing Address<br />
Signature<br />
Are you a member <strong>of</strong> The Endocrine Society? ❍ Yes ❍ No<br />
If you are a member and you know your member ID, please provide: ___________________________________________________________<br />
Prefix: First Name (Given): Middle: Last (Surname):<br />
Institution/Company:<br />
Dept/Div:<br />
Street/PO:<br />
City: State/Province: Zip/Mail Code: Country:<br />
Telephone: Fax: Email:<br />
Degree(s) that you would like listed after your name: Pr<strong>of</strong>essional Title: Date <strong>of</strong> Birth: Gender:<br />
❍ Male<br />
❍ Female<br />
Which <strong>of</strong> the following best describes your primary pr<strong>of</strong>essional role?<br />
Race or Ethnic Affiliation (voluntary)<br />
(Please mark only one)<br />
❍ African American, Black<br />
❍ Administrator ❍ Retired ❍ Asian<br />
❍ Basic Researcher ❍ Teacher/Educator ❍ Hispanic<br />
❍ Clinical Practitioner ❍ Fellow (Clinical) ❍ Native American, Eskimo, Aleut<br />
❍ Clinical Researcher ❍ Fellow (Postdoctoral/Research) ❍ Pacific Islander<br />
❍ Industry/Corporate Pr<strong>of</strong>essional ❍ Student ❍ White, Caucasian<br />
❍ Nurse/Healthcare Pr<strong>of</strong>essional ❍ Other___________________________________ ❍ Other___________________________________