Product Monograph - epgonline.org
Product Monograph - epgonline.org
Product Monograph - epgonline.org

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Acceptability<br />
Acceptability<br />
Terminology<br />
The current WHO criteria (Belsey et al. 1986) for describing<br />
vaginal bleeding patterns are:<br />
– bleeding (B): any vaginal blood loss requiring the use of 2 or<br />
more sanitary pads or tampons per day<br />
– spotting (S): any vaginal blood loss requiring no or at most 1<br />
sanitary pad or tampon per day<br />
– bleeding/spotting (B/S) episode: 1 or more consecutive day(s)<br />
during which vaginal blood loss (bleeding or spotting) occurs,<br />
each episode being bounded by B/S-free days<br />
– amenorrhea: no bleeding throughout a 90-day reference period<br />
– infrequent bleeding: 1 or 2 B/S episodes in a 90-day<br />
reference period<br />
– frequent bleeding: 6 or more B/S episodes in a 90-day<br />
reference period<br />
– prolonged bleeding: any B/S episode lasting more than 14 day<br />
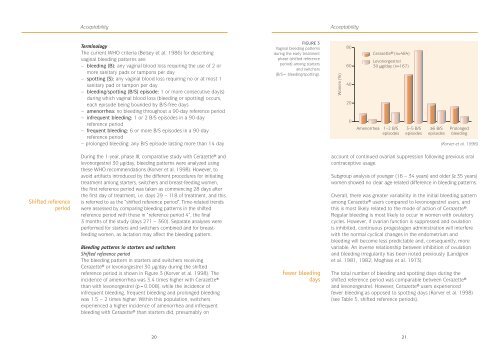
FIGURE 3<br />
Vaginal bleeding patterns<br />
during the early treatment<br />
phase (shifted reference<br />
period) among starters<br />
and switchers<br />
(B/S= bleeding/spotting).<br />
Women (%)<br />
80<br />
60<br />
40<br />
20<br />
0<br />
Amenorrhea<br />
Cerazette ® (n=484)<br />
Levon<strong>org</strong>estrel<br />
30 µg/day (n=167)<br />
1–2 B/S<br />
episodes<br />
3–5 B/S<br />
episodes<br />
≥6 B/S<br />
episodes<br />
Prolonged<br />
bleeding<br />
(Korver et al. 1998)<br />
Shifted reference<br />
period<br />
During the 1-year, phase III, comparative study with Cerazette® and<br />
levon<strong>org</strong>estrel 30 µg/day, bleeding patterns were analyzed using<br />
these WHO recommendations (Korver et al. 1998). However, to<br />
avoid artifacts introduced by the different procedures for initiating<br />
treatment among starters, switchers and breast-feeding women,<br />
the first reference period was taken as commencing 28 days after<br />
the first day of treatment, i.e. days 29 – 118 of treatment, and this<br />
is referred to as the “shifted reference period”. Time-related trends<br />
were assessed by comparing bleeding patterns in the shifted<br />
reference period with those in “reference period 4”, the final<br />
3 months of the study (days 271 – 360). Separate analyses were<br />
performed for starters and switchers combined and for breastfeeding<br />
women, as lactation may affect the bleeding pattern.<br />
Bleeding patterns in starters and switchers<br />
Shifted reference period<br />
The bleeding pattern in starters and switchers receiving<br />
Cerazette® or levon<strong>org</strong>estrel 30 µg/day during the shifted<br />
reference period is shown in Figure 3 (Korver et al. 1998). The<br />
incidence of amenorrhea was 3.4 times higher with Cerazette®<br />
than with levon<strong>org</strong>estrel (p=0.008), while the incidence of<br />
infrequent bleeding, frequent bleeding and prolonged bleeding<br />
was 1.5 – 2 times higher. Within this population, switchers<br />
experienced a higher incidence of amenorrhea and infrequent<br />
bleeding with Cerazette® than starters did, presumably on<br />
Fewer bleeding<br />
days<br />
account of continued ovarian suppression following previous oral<br />
contraceptive usage.<br />
Subgroup analysis of younger (16 – 34 years) and older (≥ 35 years)<br />
women showed no clear age-related difference in bleeding patterns.<br />
Overall, there was greater variability in the initial bleeding pattern<br />
among Cerazette® users compared to levon<strong>org</strong>estrel users, and<br />
this is most likely related to the mode of action of Cerazette®.<br />
Regular bleeding is most likely to occur in women with ovulatory<br />
cycles. However, if ovarian function is suppressed and ovulation<br />
is inhibited, continuous progestogen administration will interfere<br />
with the normal cyclical changes in the endometrium and<br />
bleeding will become less predictable and, consequently, more<br />
variable. An inverse relationship between inhibition of ovulation<br />
and bleeding irregularity has been noted previously (Landgren<br />
et al. 1981, 1982; Moghissi et al. 1973).<br />
The total number of bleeding and spotting days during the<br />
shifted reference period was comparable between Cerazette®<br />
and levon<strong>org</strong>estrel. However, Cerazette® users experienced<br />
fewer bleeding as opposed to spotting days (Korver et al. 1998)<br />
(see Table 5, shifted reference periods).<br />
20<br />
21