Drug: ACCUTANE - Magellan Health Services || TennCare Portal
Drug: ACCUTANE - Magellan Health Services || TennCare Portal
Drug: ACCUTANE - Magellan Health Services || TennCare Portal

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Prior Authorization Criteria for Amitiza ®<br />
CRITERIA FOR REVIEW<br />
Approval for Amitiza® will be granted upon documentation of:<br />
Diagnosis of idiopathic chronic constipation AND<br />
o Trial and failure of at least ONE agent from TWO of the following classes (as<br />
confirmed by paid claims by <strong>TennCare</strong>):<br />
• Osmotic laxatives<br />
• Bulk-forming laxatives<br />
• Stimulant laxatives, OR<br />
Diagnosis of constipation predominate irritable bowel syndrome (IBS) in female, AND<br />
o Trial and failure of at least ONE agent from TWO of the following classes (as<br />
confirmed by paid claims by <strong>TennCare</strong>):<br />
• Osmotic laxatives<br />
• Bulk-forming laxatives<br />
• Stimulant laxatives, OR<br />
Diagnosis of opioid induced consiptation in chronic non-cancer pain, AND<br />
o Documentation of paid claims by <strong>TennCare</strong> for opioids for at least 150 out of 180<br />
days, AND<br />
o Trial and failure of both PEG and Lactulose (as confirmed by paid claims by<br />
<strong>TennCare</strong>)<br />
COMMITTEE VOTE:<br />
APPROVED DISAPPROVED APPROVED with MODIFICATION<br />
Prior Authorization Criteria for Simbrinza ®<br />
Simbrinza ® will be approved if the following criteria is met:<br />
Patient is on simultaneous therapy with brimonidine and Azopt ® for at least 60 days<br />
Clinically valid reason why patient cannot take 2 agent seperately.<br />
COMMITTEE VOTE:<br />
APPROVED DISAPPROVED APPROVED with MODIFICATION<br />
Prior Authorization Criteria for Vecamyl ®<br />
Vecamyl will be approved for patients meeting ALL of the following criteria:<br />
Diagnosis of Essential Hypertension or Malignant Hypertension, AND<br />
Trial and failure, contraindication or intolerance to ALL of the following:<br />
o ACE inhibitor or ARB plus a diuretic; AND<br />
o Beta blocker plus a diuretic, AND<br />
o Clonidine, AND<br />
o Hydralazine<br />
COMMITTEE VOTE:<br />
APPROVED DISAPPROVED APPROVED with MODIFICATION<br />
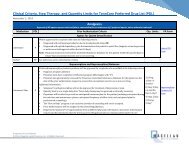
Quantity Limits<br />
Vecamyl ®<br />
10/day<br />
COMMITTEE VOTE:<br />
APPROVED DISAPPROVED APPROVED with MODIFICATION<br />
Page 12 of 14<br />
August 13, 2013 Tennessee PAC