

view Unit 19: Postpartum and Postabortion Family Planning
view Unit 19: Postpartum and Postabortion Family Planning
view Unit 19: Postpartum and Postabortion Family Planning

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>19</strong>.7 <strong>Postpartum</strong> Contraception Options for Women Living<br />
with HIV/AIDS<br />
• In general, women living with HIV/AIDS can use any hormonal method—COCs, POPs,<br />
progestin-only injectables, contraceptive implants—with some restrictions for women on<br />
ARV therapy. (See table below.)<br />
• LAM: If replacement feeding is acceptable, feasible, affordable, sustainable, <strong>and</strong> safe<br />
(AFASS), women living with HIV should avoid breastfeeding <strong>and</strong> not rely on LAM. But if<br />
replacement feeding does not meet these conditions, a woman living with HIV should<br />
breastfeed exclusively for the first 6 months, thereby using LAM (until her menses<br />
resumes).<br />
• FAM: Women who are infected with HIV, have AIDS, or are on ARV therapy can safely use<br />
fertility awareness methods after 3 menstrual cycles or normal secretions have returned.<br />
• Condoms: All clients, including clients living with HIV, should be counselled on condom use<br />
for dual protection <strong>and</strong> to prevent transmission of HIV to partners.<br />
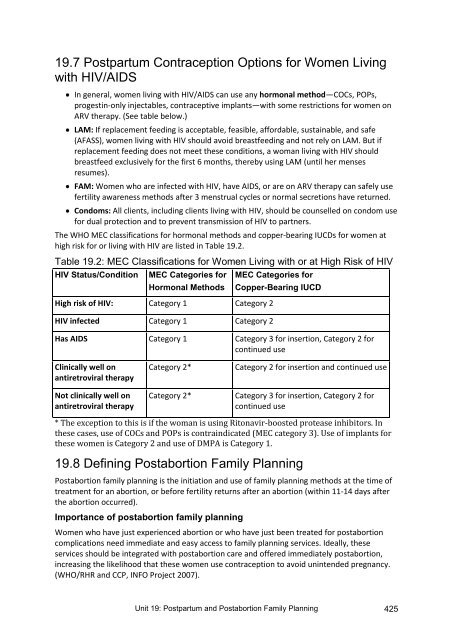
The WHO MEC classifications for hormonal methods <strong>and</strong> copper-bearing IUCDs for women at<br />
high risk for or living with HIV are listed in Table <strong>19</strong>.2.<br />
Table <strong>19</strong>.2: MEC Classifications for Women Living with or at High Risk of HIV<br />
HIV Status/Condition MEC Categories for<br />
Hormonal Methods<br />
MEC Categories for<br />
Copper-Bearing IUCD<br />
High risk of HIV: Category 1 Category 2<br />
HIV infected Category 1 Category 2<br />
Has AIDS Category 1 Category 3 for insertion, Category 2 for<br />
continued use<br />
Clinically well on<br />
antiretroviral therapy<br />
Not clinically well on<br />
antiretroviral therapy<br />
Category 2*<br />
Category 2*<br />
Category 2 for insertion <strong>and</strong> continued use<br />
Category 3 for insertion, Category 2 for<br />
continued use<br />
* The exception to this is if the woman is using Ritonavir-boosted protease inhibitors. In<br />
these cases, use of COCs <strong>and</strong> POPs is contraindicated (MEC category 3). Use of implants for<br />
these women is Category 2 <strong>and</strong> use of DMPA is Category 1.<br />
<strong>19</strong>.8 Defining <strong>Postabortion</strong> <strong>Family</strong> <strong>Planning</strong><br />
<strong>Postabortion</strong> family planning is the initiation <strong>and</strong> use of family planning methods at the time of<br />
treatment for an abortion, or before fertility returns after an abortion (within 11-14 days after<br />
the abortion occurred).<br />
Importance of postabortion family planning<br />
Women who have just experienced abortion or who have just been treated for postabortion<br />
complications need immediate <strong>and</strong> easy access to family planning services. Ideally, these<br />
services should be integrated with postabortion care <strong>and</strong> offered immediately postabortion,<br />
increasing the likelihood that these women use contraception to avoid unintended pregnancy.<br />
(WHO/RHR <strong>and</strong> CCP, INFO Project 2007).<br />
<strong>Unit</strong> <strong>19</strong>: <strong>Postpartum</strong> <strong>and</strong> <strong>Postabortion</strong> <strong>Family</strong> <strong>Planning</strong> 425



![view Unit 14: Emergency Contraceptive Pills [PDF 319KB]](https://img.yumpu.com/50082157/1/184x260/view-unit-14-emergency-contraceptive-pills-pdf-319kb.jpg?quality=85)
![view Unit 8: Intrauterine Contraceptive Devices [PDF 992KB]](https://img.yumpu.com/47853006/1/184x260/view-unit-8-intrauterine-contraceptive-devices-pdf-992kb.jpg?quality=85)



![view Unit 15: Lactational Amenorrhea Method [PDF 259KB]](https://img.yumpu.com/30000479/1/184x260/view-unit-15-lactational-amenorrhea-method-pdf-259kb.jpg?quality=85)