An assessment of interactions between global ... - ResearchGate
An assessment of interactions between global ... - ResearchGate
An assessment of interactions between global ... - ResearchGate

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Health Policy<br />
100<br />
Multisector: environment,<br />
sex, rural development<br />
Agriculture, fishing, forestry<br />
Energy, transportation,<br />
communication<br />
Other social infrastructure<br />
Government and civil<br />
society<br />
Water and sanitation<br />
Reproductive health and<br />
population services<br />
Health<br />
Education<br />
90<br />
80<br />
70<br />
Official development assistance (%)<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
1980<br />
1981<br />
1982<br />
1983<br />
1984<br />
1985<br />
1986<br />
1987<br />
1988<br />
1989<br />
1990<br />
1991<br />
1992<br />
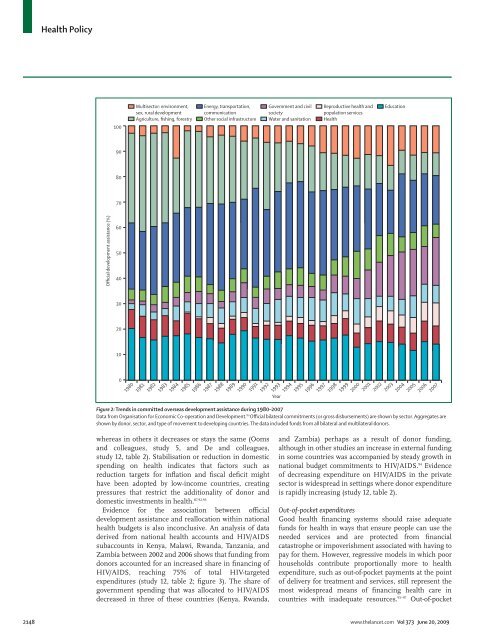
Figure 2: Trends in committed overseas development assistance during 1980–2007<br />
Data from Organisation for Economic Co-operation and Development. 80 Official bilateral commitments (or gross disbursements) are shown by sector. Aggregates are<br />
shown by donor, sector, and type <strong>of</strong> movement to developing countries. The data included funds from all bilateral and multilateral donors.<br />
whereas in others it decreases or stays the same (Ooms<br />
and colleagues, study 5, and De and colleagues,<br />
study 12, table 2). Stabilisation or reduction in domestic<br />
spending on health indicates that factors such as<br />
reduction targets for inflation and fiscal deficit might<br />
have been adopted by low-income countries, creating<br />
pressures that restrict the additionality <strong>of</strong> donor and<br />
domestic investments in health. 87,92,93<br />
Evidence for the association <strong>between</strong> <strong>of</strong>ficial<br />
development assistance and reallocation within national<br />
health budgets is also inconclusive. <strong>An</strong> analysis <strong>of</strong> data<br />
derived from national health accounts and HIV/AIDS<br />
subaccounts in Kenya, Malawi, Rwanda, Tanzania, and<br />
Zambia <strong>between</strong> 2002 and 2006 shows that funding from<br />
donors accounted for an increased share in financing <strong>of</strong><br />
HIV/AIDS, reaching 75% <strong>of</strong> total HIV-targeted<br />
expenditures (study 12, table 2; figure 3). The share <strong>of</strong><br />
government spending that was allocated to HIV/AIDS<br />
decreased in three <strong>of</strong> these countries (Kenya, Rwanda,<br />
1993<br />
Year<br />
1994<br />
1995<br />
1996<br />
1997<br />
1998<br />
1999<br />
2000<br />
2001<br />
2002<br />
2003<br />
2004<br />
2005<br />
2006<br />
2007<br />
and Zambia) perhaps as a result <strong>of</strong> donor funding,<br />
although in other studies an increase in external funding<br />
in some countries was accompanied by steady growth in<br />
national budget commitments to HIV/AIDS. 94 Evidence<br />
<strong>of</strong> decreasing expenditure on HIV/AIDS in the private<br />
sector is widespread in settings where donor expenditure<br />
is rapidly increasing (study 12, table 2).<br />
Out-<strong>of</strong>-pocket expenditures<br />
Good health financing systems should raise adequate<br />
funds for health in ways that ensure people can use the<br />
needed services and are protected from financial<br />
catastrophe or impoverishment associated with having to<br />
pay for them. However, regressive models in which poor<br />
households contribute proportionally more to health<br />
expenditure, such as out-<strong>of</strong>-pocket payments at the point<br />
<strong>of</strong> delivery for treatment and services, still represent the<br />
most widespread means <strong>of</strong> financing health care in<br />
countries with inadequate resources. 95–97 Out-<strong>of</strong>-pocket<br />
2148 www.thelancet.com Vol 373 June 20, 2009