- Page 1 and 2: ESSENTIALS OF CLINICAL NEPHROLOGY E
- Page 3 and 4: Essentials of Clinical Nephrology T
- Page 5 and 6: Dedication To the soul of my dear f
- Page 7 and 8: FOREWARD Although this country is p
- Page 9 and 10: CONTENTS Forward ..................
- Page 11 and 12: PART IX: TUBULAR AND INTERSTITIAL D
- Page 13 and 14: RENAL FUNCTIONS AND STRUCTURE KIDNE
- Page 15 and 16: Juxtaglomerular apparatus Liver Ren
- Page 17 and 18: 3. Prostanoids (Prostaglandins) (Fi
- Page 19 and 20: B- Peptide hormones degraded by the
- Page 21 and 22: main action is on the late distal t
- Page 23 and 24: - Renal venous system follows the s
- Page 25 and 26: (Fig. 1.6) Diagrammatic illustratio
- Page 27 and 28: Figure 8 shows a cross section of t
- Page 29 and 30: (Fig. 1.8d) Electron micrograph (X
- Page 31 and 32: ANATOMIC PHYSIOLOGY (FUNCTION OF DI
- Page 33 and 34: Concentration And Dilution Of Urine
- Page 35 and 36: (Fig. 1.9) Countercurrent mechanism
- Page 37 and 38: INVESTIGATIONS FOR KIDNEY DISEASES
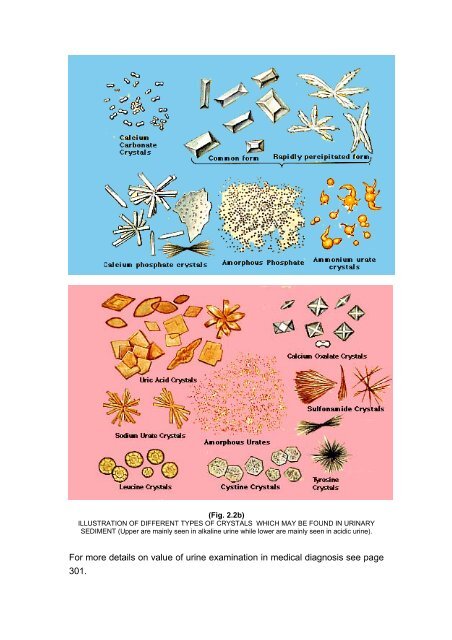
- Page 39: (Fig. 2.2a) An Illustration of Urin
- Page 43 and 44: progressive decrease in urine volum
- Page 45 and 46: C. IMMUNOLOGICAL TESTS FOR DIAGNOSI
- Page 47 and 48: B-mode U.S. imaging is the usual ex
- Page 49 and 50: (Fig. 2.4c) It shows a longitudinal
- Page 51 and 52: Duplex ultrasonography shows the st
- Page 53 and 54: (Fig. 2.8) Intravenous urography (I
- Page 55 and 56: (Fig. 2.9): The grading system adop
- Page 57 and 58: (Fig. 2.10b) IA-DSA of left kidney
- Page 59 and 60: excreted, either by glomerular filt
- Page 61 and 62: (Fig. 2.14) Diuretic Renogram (obst
- Page 63: Suggested Readings: - Wilcox CS: Is
- Page 66 and 67: B. Extrinsic antigens include bacte
- Page 68 and 69: 5. Neutrophils: have an important r
- Page 70 and 71: 2. Collagen disease (e.g. SLE, poly
- Page 72 and 73: (Fig. 3.3b) The same case in Fig. 3
- Page 74 and 75: (III) Clinical manifestations of gl
- Page 76 and 77: 1. Hypoalbuminaemia results in a de
- Page 78 and 79: 4. Manifestations of the etiologic
- Page 80 and 81: 7. Corticosteroids are given when t
- Page 82 and 83: 5. Serum creatinine is usually high
- Page 84 and 85: MCN is more common in male (male to
- Page 86 and 87: MGN could be primary or secondary t
- Page 88 and 89: . Autoimmune disease as SLE and cry
- Page 90 and 91:
monocytes), later become fibrous. G
- Page 92 and 93:
SECONDARY GLOMERULAR DISEASES In ma
- Page 94 and 95:
(Fig. 3.9d) Immunofluorescence stai
- Page 96 and 97:
10- Immunologic disorders (positive
- Page 98 and 99:
(Fig. 3.10c) Immunofluorescent stai
- Page 100 and 101:
Clinical features: Clinical manifes
- Page 102 and 103:
e responsible for the alterations i
- Page 104 and 105:
When renal failure manifests, suppo
- Page 106 and 107:
(Fig 3.14) Photograph showing the c
- Page 108 and 109:
In patients with bacterial endocard
- Page 110 and 111:
Schistosomal Nephropathy Introducti
- Page 112 and 113:
in the pathogenesis of local tissue
- Page 114 and 115:
well-documented in an extensive exp
- Page 116 and 117:
Glomerulopathy Secondary To Virus I
- Page 118 and 119:
8- Autoimmune thyroiditis. 9- Polya
- Page 120 and 121:
TREATMENT OF GLOMERULONEPHRITIS The
- Page 122 and 123:
term, but an effect may be obtained
- Page 124 and 125:
Suggested Readings: - Woo KT: Recen
- Page 126 and 127:
Polyarteritis Nodosa Incidence: Pol
- Page 128 and 129:
Clinical features of PAN: 1- Consti
- Page 130 and 131:
Immunofluorescence microscopy is al
- Page 132 and 133:
Renal pathology: • Glomeruli show
- Page 134 and 135:
larynx. Vasculitis in this disease
- Page 136 and 137:
(Fig. 4.4b) Immunofluorescen staine
- Page 138 and 139:
Suggested Readings: - Griffith ME,
- Page 140 and 141:
(Fig. 5.1a) H & E stained section(X
- Page 142 and 143:
There are 5 outstanding features fo
- Page 145 and 146:
ACUTE RENAL FAILURE (ARF) Definitio
- Page 147 and 148:
Acute Tubular Necrosis Acute tubula
- Page 149 and 150:
Tumour Specific Syndromes: Tumour l
- Page 151 and 152:
2. Renal Ultrasonography and echo-d
- Page 153 and 154:
If the case proved to be pre-renal,
- Page 155 and 156:
In case of contrast media, the foll
- Page 157:
Suggested Readings: - McCarthy JT:
- Page 160 and 161:
year, while in Egypt and some devel
- Page 162 and 163:
PATHOPHYSIOLOGY OF CHRONIC RENAL FA
- Page 164 and 165:
(Fig. 7.1) Disturbances of Acid-bas
- Page 166 and 167:
(Fig. 7.2a) Disturbances of calcium
- Page 168 and 169:
Calcified papillae shown in plain f
- Page 170 and 171:
Eye CNS • Malaise, lethergy • c
- Page 172 and 173:
• Iatrogenic causes as frequent b
- Page 174 and 175:
• Uraemic amaurosis (rare): which
- Page 176 and 177:
INVESTIGATIONS OF A CASE WITH CHRON
- Page 178 and 179:
c. Postrenal factors: Causing obstr
- Page 180 and 181:
Step 4. RENAL REPLACEMENT THERAPY (
- Page 182 and 183:
solutes that can pass easily throug
- Page 184 and 185:
(C) Nausea and Vomiting: The aetiol
- Page 186 and 187:
(C) Arrhythmia: Arrhythmias during
- Page 188 and 189:
3- Recent thoracic or abdominal sur
- Page 190 and 191:
KIDNEY TRANSPLANTATION Definition:
- Page 192 and 193:
2- Cadaveric donors: These are pers
- Page 194 and 195:
. Complications due to individual d
- Page 196 and 197:
- Ter Wee PM, et al: Dietary protei
- Page 198 and 199:
B) Amino acids tubular transport de
- Page 200 and 201:
distal RTA, more HCO 3 and chloride
- Page 202 and 203:
2. Hypokalemia due to defective han
- Page 204 and 205:
4. Autoimmune disease • Sjogren's
- Page 206 and 207:
5. Miscellaneous • Amyloidosis
- Page 208 and 209:
WILSON'S DISEASE Characterized by a
- Page 210 and 211:
Treatment: 1. Vitamin D (either the
- Page 213 and 214:
TUBULAR AND INTERSTITIAL DISEASES T
- Page 215 and 216:
(Fig. 9.1a) Cross section of a kidn
- Page 217 and 218:
The etiologic cause is unknown, pos
- Page 219 and 220:
3. Vascular sclerosis: Affecting sm
- Page 221 and 222:
5. Pregnancy and gonadal manifestat
- Page 223 and 224:
VUR is genetically determined. It h
- Page 225 and 226:
3. Obstruction of the urinary tract
- Page 227 and 228:
Symptoms: Fever, malaise, aches, dy
- Page 229 and 230:
2. Hypertension. 3. Insidious onset
- Page 231 and 232:
d) Direct infection : From epididym
- Page 233 and 234:
Symptoms: 1- Asymptomatic 2- Consti
- Page 235 and 236:
Cystoscopy - May show ulcers or con
- Page 237 and 238:
Rationale of short antituberculous
- Page 239 and 240:
Drug Route of Dose in GFR GFR GFR n
- Page 241 and 242:
Disadvantages: - Needs experience a
- Page 243 and 244:
CYSTIC RENAL DISEASES Renal cyst is
- Page 245 and 246:
tricuspid valve incompetence and le
- Page 247 and 248:
Pathology: 1. Both kidneys are enla
- Page 249 and 250:
IVU- medullary sponge kidney demons
- Page 251 and 252:
Management 1. Patients under dialys
- Page 253 and 254:
RENAL STONE DISEASES Renal stone di
- Page 255 and 256:
6. Xanthinuria It is a very rare me
- Page 257:
Suggested Readings: - Jaeger O: Gen
- Page 260 and 261:
solutes which could affect plasma o
- Page 262 and 263:
2. Volume receptors are mainly in t
- Page 264 and 265:
• Essential hyponatraemia: Occurs
- Page 266 and 267:
saline and in severe cases, small a
- Page 268 and 269:
III. DISTURBANCES IN PLASMA POTASSI
- Page 270 and 271:
B- Increase renal excretion of K +
- Page 272 and 273:
(Fig. 12.1) Extensive vacuolization
- Page 274 and 275:
3- Gastrointestinal manifestations
- Page 277 and 278:
DISORDERS OF ACID-BASE BALANCE Phys
- Page 279 and 280:
HCo 3 -. Since these substances are
- Page 281 and 282:
B- Gastrointestinal causes of metab
- Page 283 and 284:
• Cushing's syndrome • Bartter'
- Page 285 and 286:
HYPERTENSION AND THE KIDNEY The val
- Page 287 and 288:
2- Secretion of hormone which cause
- Page 289 and 290:
(Fig. 14.2b) Hx&E stained kidney se
- Page 291 and 292:
pressure is released gradually (2cm
- Page 293 and 294:
2- Vasodilators: This group include
- Page 295 and 296:
the angiotensin II. There are three
- Page 297 and 298:
Secondary Hypertension A- Renal Hyp
- Page 299 and 300:
A-Two-kidney-one-clip (2K/1C) model
- Page 301 and 302:
(Fig. 14.5 ) An angiogram showing a
- Page 303 and 304:
PTCA will be tried as example in yo
- Page 305 and 306:
Suggested Readings: - Stanley JC: D
- Page 307 and 308:
MISCELLANEOUS PROTEINURIA Proteinur
- Page 309 and 310:
a. Strenuous exercise b. Fever c. O
- Page 311 and 312:
4. Casts such as proteinuria. 5. Bl
- Page 313 and 314:
VALUE OF URINE EXAMINATION IN MEDIC
- Page 315 and 316:
3. Colour: - Normal: umber yellow -
- Page 317 and 318:
• Direct microscopic examination
- Page 319 and 320:
7. Chemicals: Determination of 24 h
- Page 321 and 322:
RENAL MANIFESTATIONS OF SYSTEMIC DI
- Page 323 and 324:
2- Nephrogenic diabetes insipidus.
- Page 325 and 326:
Gout and Kidney Patient with gout m
- Page 327 and 328:
RENAL DISEASES IN HEPATIC PATIENTS
- Page 329 and 330:
• Elevated plasma endothelin (E)
- Page 331 and 332:
• Orthotopic liver transplantatio
- Page 333 and 334:
MALIGNANCY AND THE KIDNEY The spect
- Page 335 and 336:
Multiple myeloma. Case of light cha
- Page 337 and 338:
POEMS Syndrome (P= polyneuropathy,
- Page 339 and 340:
2- Minimal change glomerulonephriti
- Page 341 and 342:
Prevention of tumour lysis syndrome
- Page 343 and 344:
• Non Hodgkin's lymphoma, and Kap
- Page 345 and 346:
DRUGS AND THE KIDNEY In this chapte
- Page 347 and 348:
• Uremia may reduce drug metaboli
- Page 349 and 350:
• It's usual dose is 1gm / 8hrs.
- Page 351 and 352:
• Digoxin is not dialyzable • Q
- Page 353 and 354:
• Renal prostaglandins (PGE 2 , P
- Page 355 and 356:
(D) Diuretic treatment of nephrotic
- Page 357 and 358:
KIDNEY AND THE HEART This issue cou
- Page 359 and 360:
Suggested Readings: - Leschke M, et
- Page 361 and 362:
• The renal vessels may show inti
- Page 363 and 364:
Suggested Readings: - Lindeman RD,
- Page 365 and 366:
Renal pathology: Glomeruli show swe
- Page 367 and 368:
- Treatment of sudden acute renal f
- Page 369 and 370:
Pregnancy In Dialysis Patients: •
- Page 371 and 372:
ENVIRONMENTALLY-INDUCED KIDNEY DISE
- Page 373 and 374:
Lead containing inclusion bodies wi
- Page 375 and 376:
Radiation injury It may be defined
- Page 377:
Suggested Reading: - Sobh M: Enviro