CHN4101 Orthopedic Surgery Post Operative.pdf - Carondelet
CHN4101 Orthopedic Surgery Post Operative.pdf - Carondelet
CHN4101 Orthopedic Surgery Post Operative.pdf - Carondelet

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
P<br />
H<br />
Y<br />
S<br />
I<br />
C<br />
I<br />
A<br />
N<br />
‘<br />
S<br />
O<br />
R<br />
D<br />
E<br />
R<br />
USE BALL POINT PEN – PRESS FIRMLY<br />
CARONDELET HEALTH NETWORK<br />
HOSPITAL PROVIDED PRE-PRINTED PHYSICIAN’S ORDERS<br />
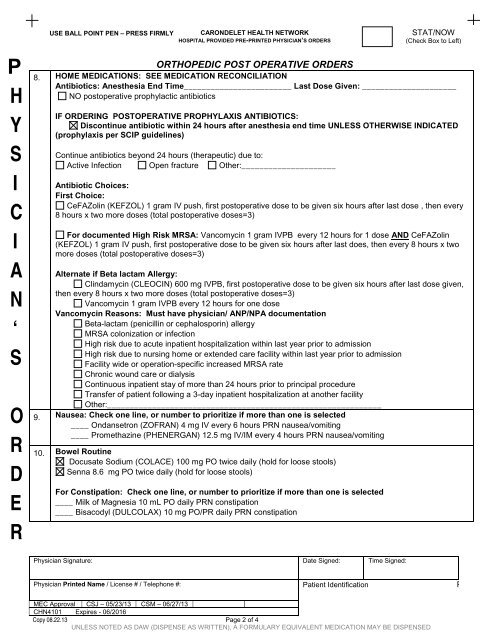
ORTHOPEDIC POST OPERATIVE ORDERS<br />
STAT/NOW<br />
(Check Box to Left)<br />
8. HOME MEDICATIONS: SEE MEDICATION RECONCILIATION<br />
Antibiotics: Anesthesia End Time________________________ Last Dose Given: _____________________<br />
NO postoperative prophylactic antibiotics<br />
IF ORDERING POSTOPERATIVE PROPHYLAXIS ANTIBIOTICS:<br />
Discontinue antibiotic within 24 hours after anesthesia end time UNLESS OTHERWISE INDICATED<br />
(prophylaxis per SCIP guidelines)<br />
Continue antibiotics beyond 24 hours (therapeutic) due to:<br />
Active Infection Open fracture Other:_____________________<br />
Antibiotic Choices:<br />
First Choice:<br />
CeFAZolin (KEFZOL) 1 gram IV push, first postoperative dose to be given six hours after last dose , then every<br />
8 hours x two more doses (total postoperative doses=3)<br />
For documented High Risk MRSA: Vancomycin 1 gram IVPB every 12 hours for 1 dose AND CeFAZolin<br />
(KEFZOL) 1 gram IV push, first postoperative dose to be given six hours after last does, then every 8 hours x two<br />
more doses (total postoperative doses=3)<br />
Alternate if Beta lactam Allergy:<br />
Clindamycin (CLEOCIN) 600 mg IVPB, first postoperative dose to be given six hours after last dose given,<br />
then every 8 hours x two more doses (total postoperative doses=3)<br />
Vancomycin 1 gram IVPB every 12 hours for one dose<br />
Vancomycin Reasons: Must have physician/ ANP/NPA documentation<br />
Beta-lactam (penicillin or cephalosporin) allergy<br />
MRSA colonization or infection<br />
High risk due to acute inpatient hospitalization within last year prior to admission<br />
High risk due to nursing home or extended care facility within last year prior to admission<br />
Facility wide or operation-specific increased MRSA rate<br />
Chronic wound care or dialysis<br />
Continuous inpatient stay of more than 24 hours prior to principal procedure<br />
Transfer of patient following a 3-day inpatient hospitalization at another facility<br />
Other:_____________________________________________________________<br />
9. Nausea: Check one line, or number to prioritize if more than one is selected<br />
____ Ondansetron (ZOFRAN) 4 mg IV every 6 hours PRN nausea/vomiting<br />
____ Promethazine (PHENERGAN) 12.5 mg IV/IM every 4 hours PRN nausea/vomiting<br />
10. Bowel Routine<br />
Docusate Sodium (COLACE) 100 mg PO twice daily (hold for loose stools)<br />
Senna 8.6 mg PO twice daily (hold for loose stools)<br />
For Constipation: Check one line, or number to prioritize if more than one is selected<br />
____ Milk of Magnesia 10 mL PO daily PRN constipation<br />
____ Bisacodyl (DULCOLAX) 10 mg PO/PR daily PRN constipation<br />
Physician Signature: Date Signed: Time Signed:<br />
Physician Printed Name / License # / Telephone #: Patient Identification P<br />
MEC Approval CSJ – 05/23/13 CSM – 06/27/13<br />
<strong>CHN4101</strong> Expires - 06/2016<br />
Copy 08.22.13 Page 2 of 4<br />
UNLESS NOTED AS DAW (DISPENSE AS WRITTEN), A FORMULARY EQUIVALENT MEDICATION MAY BE DISPENSED