EAR CARE PROCEDURE FOR COMMUNITY NURSING SERVICES
EAR CARE PROCEDURE FOR COMMUNITY NURSING SERVICES
EAR CARE PROCEDURE FOR COMMUNITY NURSING SERVICES

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
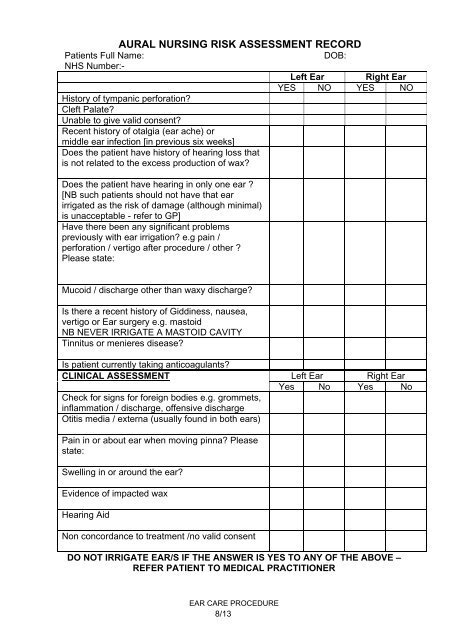
AURAL <strong>NURSING</strong> RISK ASSESSMENT RECORD<br />
Patients Full Name:<br />
DOB:<br />
NHS Number:-<br />
Left Ear Right Ear<br />
YES NO YES NO<br />
History of tympanic perforation<br />
Cleft Palate<br />
Unable to give valid consent<br />
Recent history of otalgia (ear ache) or<br />
middle ear infection [in previous six weeks]<br />
Does the patient have history of hearing loss that<br />
is not related to the excess production of wax<br />
Does the patient have hearing in only one ear <br />
[NB such patients should not have that ear<br />
irrigated as the risk of damage (although minimal)<br />
is unacceptable - refer to GP]<br />
Have there been any significant problems<br />
previously with ear irrigation e.g pain /<br />
perforation / vertigo after procedure / other <br />
Please state:<br />
Mucoid / discharge other than waxy discharge<br />
Is there a recent history of Giddiness, nausea,<br />
vertigo or Ear surgery e.g. mastoid<br />
NB NEVER IRRIGATE A MASTOID CAVITY<br />
Tinnitus or menieres disease<br />
Is patient currently taking anticoagulants<br />
CLINICAL ASSESSMENT<br />
Check for signs for foreign bodies e.g. grommets,<br />
inflammation / discharge, offensive discharge<br />
Otitis media / externa (usually found in both ears)<br />
Left Ear Right Ear<br />
Yes No Yes No<br />
Pain in or about ear when moving pinna Please<br />
state:<br />
Swelling in or around the ear<br />
Evidence of impacted wax<br />
Hearing Aid<br />
Non concordance to treatment /no valid consent<br />
DO NOT IRRIGATE <strong>EAR</strong>/S IF THE ANSWER IS YES TO ANY OF THE ABOVE –<br />
REFER PATIENT TO MEDICAL PRACTITIONER<br />
<strong>EAR</strong> <strong>CARE</strong> <strong>PROCEDURE</strong><br />
8/13