Patient Forms
Patient Forms
Patient Forms

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
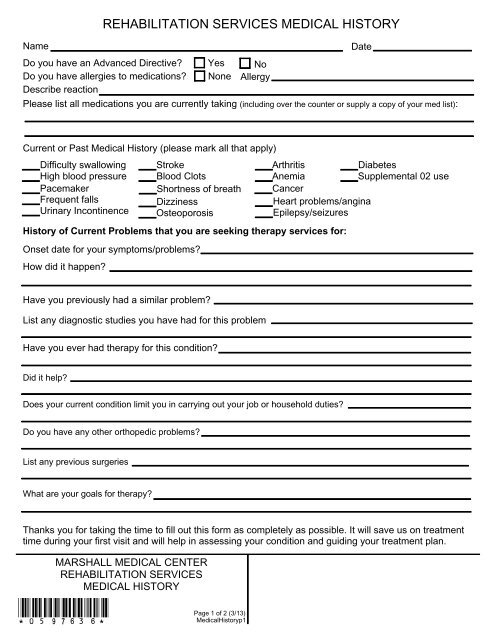
REHABILITATION SERVICES MEDICAL HISTORY<br />
Name<br />
Date<br />
Do you have an Advanced Directive<br />
Do you have allergies to medications<br />
Describe reaction<br />
Yes<br />
None<br />
No<br />
Allergy<br />
Please list all medications you are currently taking (including over the counter or supply a copy of your med list):<br />
Current or Past Medical History (please mark all that apply)<br />
Difficulty swallowing Stroke<br />
Arthritis<br />
Diabetes<br />
High blood pressure Blood Clots<br />
Anemia<br />
Supplemental 02 use<br />
Pacemaker Shortness of breath Cancer<br />
Frequent falls<br />
Dizziness<br />
Heart problems/angina<br />
Urinary Incontinence Osteoporosis<br />
Epilepsy/seizures<br />
History of Current Problems that you are seeking therapy services for:<br />
Onset date for your symptoms/problems<br />
How did it happen<br />
Have you previously had a similar problem<br />
List any diagnostic studies you have had for this problem<br />
Have you ever had therapy for this condition<br />
Did it help<br />
Does your current condition limit you in carrying out your job or household duties<br />
Do you have any other orthopedic problems<br />
List any previous surgeries<br />
What are your goals for therapy<br />
Thanks you for taking the time to fill out this form as completely as possible. It will save us on treatment<br />
time during your first visit and will help in assessing your condition and guiding your treatment plan.<br />
MARSHALL MEDICAL CENTER<br />
REHABILITATION SERVICES<br />
MEDICAL HISTORY<br />
*0597636* Page 1 of 2 (3/13)<br />
MedicalHistoryp1
REHABILITATION SERVICES MEDICAL HISTORY-page 2<br />
Draw in areas of pain on body diagrams using appropriate symbols.<br />
Severe Pain<br />
Moderate Pain<br />
Dull Ache<br />
Radiating Pain<br />
Numbness/Tingling<br />
*******<br />
0000000<br />
∩∩∩∩∩<br />
↑↓↑↓↑↓↑↓<br />
XXXXXXX<br />
Reviewed by _____________________________________________ Date _______________ Time ________________<br />
Signature / Title<br />
MARSHALL MEDICAL CENTER<br />
REHABILITATION SERVICES<br />
MEDICAL HISTORY<br />
*0597636* Page 2 of 2 (3/13)<br />
MedicalHistoryp2