- Page 1 and 2: FLORIDA HEALTH CARE PLANS EAST VOLU
- Page 3 and 4: FLUOROSCOPIC PROCEDURES............
- Page 5 and 6: ULTRASOUND ........................
- Page 7 and 8: 2 EAST 06/01/08 FLORIDA HEALTH CARE
- Page 9 and 10: ALLERGY Robert DiNicolo, M.D. # 001
- Page 11 and 12: DIABETIC SHOE PROVIDERS Atlantic Po
- Page 13 and 14: CARDIOLOGY Preferred Medical Center
- Page 15 and 16: CHIROPRACTIC Lawrence Petker, D.C.
- Page 17 and 18: DENTAL SERVICES Preferred Medical C
- Page 19 and 20: DIABETES EDUCATION Florida Health C
- Page 21 and 22: DIALYSIS SERVICES DVA Healthcare Re
- Page 23 and 24: Acute Low Back & Neck Pain • This
- Page 25 and 26: EAR LAVAGE Florida Health Care Plan
- Page 27 and 28: EMG TESTING Preferred Medical Cente
- Page 29 and 30: FLUOROSCOPIC PROCEDURES Twin Lakes
- Page 31 and 32: GENETIC TESTING All Genetic Testing
- Page 33 and 34: GYNECOLOGY AND WELL WOMAN’S ASSES
- Page 35 and 36: HOME HEALTH CARE Doctors’ Choice
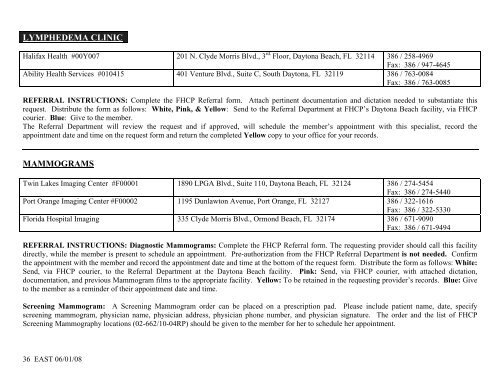
- Page 37 and 38: HOSPITAL SURGERY Halifax Health #00
- Page 39: INFUSION / INJECTION CLINIC Florida
- Page 43 and 44: NEPHROLOGY Nephrology Consultants,
- Page 45 and 46: NEUROLOGY (cont’d) Coastal Neurol
- Page 47 and 48: OBSTETRICS Halifax OB/GYN Associate
- Page 49 and 50: ONCOLOGY - MEDICAL/HEMATOLOGY (cont
- Page 51 and 52: OPHTHALMOLOGY Preferred Medical Cen
- Page 53 and 54: ORTHOPAEDICS Preferred Medical Cent
- Page 55 and 56: OSTOMY SERVICES Florida Health Care
- Page 57 and 58: BALANCE & VESTIBULAR THERAPY Univer
- Page 59 and 60: PAIN MANAGEMENT (cont’d) Ambulato
- Page 61 and 62: PHARMACY FHCP Pharmacy 350 N. Clyde
- Page 63 and 64: PODIATRY Atlantic Podiatry Associat
- Page 65 and 66: PRIMARY CARE (cont’d) Pablo Garci
- Page 67 and 68: SUBSTANCE ABUSE, DETOXIFICATION AND
- Page 69 and 70: PULMONOLOGY Suresh D. Desai, M.D. #
- Page 71 and 72: RHEUMATOLOGY - PEDIATRICS Children
- Page 73 and 74: SMOKING CESSATION PROGRAM QuitSmart
- Page 75 and 76: SURGERY-CARDIOVASCULAR Coastal Card
- Page 77 and 78: MINOR SURGICAL CLINIC Harry H. Blac
- Page 79 and 80: SURGERY - PLASTIC Vijay Moradia, M.
- Page 81 and 82: SURGERY - VASCULAR Surgical Associa
- Page 83 and 84: URGENT CARE SERVICES MediQuick Urge
- Page 85 and 86: VARICOSE VEIN TREATMENT Thomas Corb
- Page 87 and 88: WOUND CARE CLINIC Florida Health Ca
- Page 89 and 90: FLORIDA HEALTH CARE PLANS SOUTHEAST
- Page 91 and 92:
FLUOROSCOPIC PROCEDURES............
- Page 93 and 94:
ULTRASOUND ........................
- Page 95 and 96:
FLORIDA HEALTH CARE PLANS OUTPATIEN
- Page 97 and 98:
ALLERGY Robert DiNicolo, M.D. # 001
- Page 99 and 100:
DIABETIC SHOE PROVIDERS Atlantic Po
- Page 101 and 102:
CARDIOLOGY Yogesh Shah, M.D. #01045
- Page 103 and 104:
CHIROPRACTIC Michelle Gingras, D.C.
- Page 105 and 106:
DENTAL SERVICES Preferred Medical C
- Page 107 and 108:
DIABETES EDUCATION Florida Health C
- Page 109 and 110:
DIALYSIS SERVICES DVA Healthcare Re
- Page 111 and 112:
Acute Low Back & Neck Pain • This
- Page 113 and 114:
EAR LAVAGE Florida Health Care Plan
- Page 115 and 116:
EMG TESTING Preferred Medical Cente
- Page 117 and 118:
FLUOROSCOPIC PROCEDURES Bert Fish M
- Page 119 and 120:
GASTROENTEROLOGY (cont’d) Nagrani
- Page 121 and 122:
GYNECOLOGY AND WELL WOMAN’S ASSES
- Page 123 and 124:
HOME HEALTH CARE Doctors’ Choice
- Page 125 and 126:
INFECTIOUS DISEASES Daniel Warner,
- Page 127 and 128:
LABORATORY SERVICES - ROUTINE LabCo
- Page 129 and 130:
MRI’S Bert Fish Medical Center #0
- Page 131 and 132:
NEUROLOGY Preferred Medical Centers
- Page 133 and 134:
OBSTETRICS Halifax OB/GYN Associate
- Page 135 and 136:
OPHTHALMOLOGY Robert C. Dean, M.D.
- Page 137 and 138:
ORTHOPAEDICS Atlantic Orthopaedic A
- Page 139 and 140:
OSTOMY SERVICES Florida Health Care
- Page 141 and 142:
BALANCE & VESTIBULAR THERAPY Univer
- Page 143 and 144:
PAIN MANAGEMENT (cont’d) Ambulato
- Page 145 and 146:
PHYSICAL MEDICINE AND REHABILITATIO
- Page 147 and 148:
PSYCHIATRY / BEHAVIORAL HEALTH Marg
- Page 149 and 150:
SUBSTANCE ABUSE, DETOXIFICATION AND
- Page 151 and 152:
PULMONOLOGY Suresh D. Desai, M.D. #
- Page 153 and 154:
RHEUMATOLOGY - PEDIATRICS Children
- Page 155 and 156:
SMOKING CESSATION PROGRAM QuitSmart
- Page 157 and 158:
SURGERY-CARDIOVASCULAR Coastal Card
- Page 159 and 160:
SURGERY-GENERAL Avrohm Faber, M.D.
- Page 161 and 162:
SURGERY - ORAL Peter J. Linek, D.D.
- Page 163 and 164:
SURGERY - THORACIC Coastal Cardiova
- Page 165 and 166:
SUTURE AND STAPLE REMOVAL Florida H
- Page 167 and 168:
URGENT CARE SERVICES MediQuick Urge
- Page 169 and 170:
VARICOSE VEIN TREATMENT Thomas Corb
- Page 171 and 172:
WEIGHT MANAGEMENT PROGRAM Halifax F
- Page 173 and 174:
FLORIDA HEALTH CARE PLANS WEST VOLU
- Page 175 and 176:
EVENT MONITOR......................
- Page 177 and 178:
SURGERY-THORACIC ..................
- Page 179 and 180:
***********************************
- Page 181 and 182:
ALLERGY Asthma & Allergy Specialist
- Page 183 and 184:
BRACES / ORTHOTICS / PROSTHETICS Am
- Page 185 and 186:
CARDIAC CATHETERIZATION Florida Hos
- Page 187 and 188:
CARDIOLOGY (cont’d) Central Flori
- Page 189 and 190:
CHIROPRACTIC James Jeremy Hether, D
- Page 191 and 192:
CT’S Florida Hospital - DeLand #0
- Page 193 and 194:
DERMATOLOGY Acclaimed Dermatology R
- Page 195 and 196:
DIAGNOSTIC TESTING Florida Hospital
- Page 197 and 198:
DISEASE MANAGEMENT PROGRAMS The lis
- Page 199 and 200:
DURABLE MEDICAL EQUIPMENT Apria Hea
- Page 201 and 202:
EAR, NOSE AND THROAT (ENT) Coastal
- Page 203 and 204:
EMG TESTING Central Florida Neurolo
- Page 205 and 206:
EVENT MONITOR Florida Health Care P
- Page 207 and 208:
GASTROENTEROLOGY Central Florida Ga
- Page 209 and 210:
GENETIC TESTING All Genetic Testing
- Page 211 and 212:
GYNECOLOGY AND WELL WOMAN’S ASSES
- Page 213 and 214:
HOLTER MONITOR Florida Health Care
- Page 215 and 216:
HOSPITAL SURGERY Florida Hospital -
- Page 217 and 218:
INFUSION CLINIC Florida Health Care
- Page 219 and 220:
LABORATORY SERVICES - ROUTINE Flori
- Page 221 and 222:
MRI’S Florida Hospital - DeLand #
- Page 223 and 224:
NEPHROLOGY Nephrology Consultants,
- Page 225 and 226:
NEUROLOGY (con’t) Preferred Medic
- Page 227 and 228:
OBSTETRICS Halifax OB/GYN Associate
- Page 229 and 230:
ONCOLOGY-RADIATION Florida Oncology
- Page 231 and 232:
OPTOMETRY Total Vision Eye & Contac
- Page 233 and 234:
ORTHOPAEDICS - SPORTS MEDICINE (Non
- Page 235 and 236:
***********************************
- Page 237 and 238:
PAIN MANAGEMENT Pain Management & R
- Page 239 and 240:
PEDIATRICS Preferred Medical Center
- Page 241 and 242:
PHYSICAL MEDICINE AND REHABILITATIO
- Page 243 and 244:
PRIMARY CARE Preferred Medical Cent
- Page 245 and 246:
PSYCHIATRY / BEHAVIORAL HEALTH Fami
- Page 247 and 248:
PULMONARY FUNCTION TESTS (PFT’s)
- Page 249 and 250:
RABIES VACCINE SERIES Volusia Count
- Page 251 and 252:
RHEUMATOLOGY - PEDIATRICS Children
- Page 253 and 254:
SMOKING CESSATION PROGRAM QuitSmart
- Page 255 and 256:
SURGERY-CARDIOVASCULAR Coastal Card
- Page 257 and 258:
SURGERY-GENERAL Rene Capulong, M.D.
- Page 259 and 260:
SURGERY - ORAL Peter J. Linek, D.D.
- Page 261 and 262:
SURGERY-THORACIC Corbyons & Donohoe
- Page 263 and 264:
SURGERY - VASCULAR Surgical Associa
- Page 265 and 266:
ULTRASOUND Florida Health Care Plan
- Page 267 and 268:
UROLOGY Atlantic Urology Associates
- Page 269 and 270:
VNG TESTING Timko Hearing and Balan
- Page 271 and 272:
X-RAYS (PLAIN FILMS) Florida Health
- Page 273 and 274:
TABLE OF CONTENTS ACUTE LOW BACK &
- Page 275 and 276:
OUTPATIENT REHABILITATION .........
- Page 277 and 278:
ACUTE LOW BACK & NECK PROGRAM This
- Page 279 and 280:
AFTER HOURS PRIMARY CARE FHCP Pedia
- Page 281 and 282:
BONE DENSITY STUDIES Florida Health
- Page 283 and 284:
CARDIAC CATHETERIZATION Florida Hos
- Page 285 and 286:
CARDIOLOGY - PEDIATRIC Pediatric Ca
- Page 287 and 288:
CT’S Florida Hospital - Flagler #
- Page 289 and 290:
DERMATOLOGY Acclaimed Dermatology R
- Page 291 and 292:
DIAGNOSTIC TESTING Florida Hospital
- Page 293 and 294:
DISEASE MANAGEMENT PROGRAMS The lis
- Page 295 and 296:
DURABLE MEDICAL EQUIPMENT Apria Hea
- Page 297 and 298:
EEG TESTING Florida Hospital - Flag
- Page 299 and 300:
EVENT MONITOR Florida Health Care P
- Page 301 and 302:
GENETIC TESTING All Genetic Testing
- Page 303 and 304:
GYNECOLOGY AND WELL WOMAN’S ASSES
- Page 305 and 306:
HOME HEALTH CARE Doctors’ Choice
- Page 307 and 308:
INFECTIOUS DISEASES Daniel A. Warne
- Page 309 and 310:
LABORATORY SERVICES - ROUTINE Flori
- Page 311 and 312:
MRI’S Florida Hospital - Flagler
- Page 313 and 314:
NEUROLOGY Preferred Medical Centers
- Page 315 and 316:
OBSTETRICS Halifax OB/GYN Associate
- Page 317 and 318:
ONCOLOGY - MEDICAL/HEMATOLOGY (cont
- Page 319 and 320:
OPHTHALMOLOGY Preferred Medical Cen
- Page 321 and 322:
ORTHOPAEDICS - SPORTS MEDICINE (Non
- Page 323 and 324:
FLORIDA HEALTH CARE PLANS OUTPATIEN
- Page 325 and 326:
PAIN MANAGEMENT Pain Management & R
- Page 327 and 328:
PEDIATRICS Preferred Medical Center
- Page 329 and 330:
PODIATRY Atlantic Podiatry Associat
- Page 331 and 332:
SUBSTANCE ABUSE, DETOXIFICATION AND
- Page 333 and 334:
PULMONOLOGY Lawrence Burns, M.D. #0
- Page 335 and 336:
RHEUMATOLOGY - PEDIATRICS Children
- Page 337 and 338:
SMOKING CESSATION PROGRAM QuitSmart
- Page 339 and 340:
SURGERY - CARDIOVASCULAR Coastal Ca
- Page 341 and 342:
SURGERY-GENERAL Alfred Alson, M.D.
- Page 343 and 344:
SURGERY - ORAL Peter J. Linek, D.D.
- Page 345 and 346:
SURGERY - VASCULAR Surgical Associa
- Page 347 and 348:
ULTRASOUND Florida Health Care Plan
- Page 349 and 350:
UROLOGY Atlantic Urological Associa
- Page 351 and 352:
VNG TESTING Timko Hearing and Balan
- Page 353:
X-RAYS (PLAIN FILMS) Florida Health