Advocate Health Care Network Plan-Humana PPO - Advocate Benefits
Advocate Health Care Network Plan-Humana PPO - Advocate Benefits
Advocate Health Care Network Plan-Humana PPO - Advocate Benefits

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
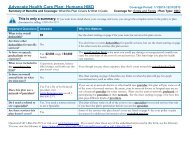
<strong>Advocate</strong> <strong>Health</strong> <strong>Care</strong> <strong>Network</strong> <strong>Plan</strong>-<strong>Humana</strong> <strong>PPO</strong> Coverage Period: 01/01/2013 – 12/31/2013<br />
Summary of <strong>Benefits</strong> and Coverage: What this <strong>Plan</strong> Covers & What it Costs Coverage for: Individual + Family | <strong>Plan</strong> Type: <strong>PPO</strong><br />
Common<br />
Medical Event<br />
If you have mental<br />
health, behavioral<br />
health, or substance<br />
abuse needs<br />
If you are pregnant<br />
If you need help<br />
recovering or have<br />
other special health<br />
needs<br />
If your child needs<br />
dental or eye care<br />
Your Cost If Your Cost If You<br />
Services You May Need<br />
You Use an Use an<br />
In-network Out-of-network<br />
Limitations & Exceptions<br />
Provider Provider<br />
Mental/Behavioral health outpatient services 20% coinsurance 40% coinsurance ---none---<br />
Preauthorization applies. Your cost<br />
Mental/Behavioral health inpatient services 20% coinsurance 40% coinsurance if prior authorization is not received<br />
is 50%.<br />
Substance use disorder outpatient services 20% coinsurance 40% coinsurance ---none---<br />
Preauthorization applies. Your cost<br />
Substance use disorder inpatient services 20% coinsurance 40% coinsurance if prior authorization is not received<br />
is 50%.<br />
Prenatal and postnatal care 20% coinsurance 40% coinsurance ----none----<br />
Delivery and all inpatient services 20% coinsurance 40% coinsurance ----none----<br />
Preauthorization applies. Your<br />
Home health care 20% coinsurance 40% coinsurance cost if prior authorization is not<br />
received is 50%.<br />
Rehabilitation services 20% coinsurance 40% coinsurance 60 visits per benefit period.<br />
Habilitation services 20% coinsurance 40% coinsurance 60 visits per benefit period.<br />
Preauthorization applies. Your<br />
Skilled nursing care 20% coinsurance 40% coinsurance cost if prior authorization is not<br />
received is 50%.<br />
<strong>Benefits</strong> are limited to items used to<br />
serve a medical purpose. DME<br />
Durable medical equipment 20% coinsurance 40% coinsurance benefits are provided for both<br />
purchase and rental equipment (up<br />
to the purchase price).<br />
Preauthorization applies. Your cost<br />
Hospice service 20% coinsurance 40% coinsurance if prior authorization is not received<br />
is 50%.<br />
Eye exam Not Covered Not Covered ---none---<br />
Glasses Not Covered Not Covered ---none---<br />
Dental check-up Not Covered Not Covered ---none---