Anthem CA Lumenos HSA 1500 Complete ... - Medicoverage
Anthem CA Lumenos HSA 1500 Complete ... - Medicoverage
Anthem CA Lumenos HSA 1500 Complete ... - Medicoverage

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
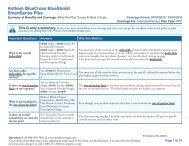
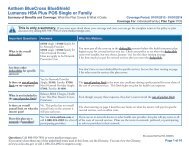
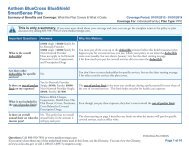
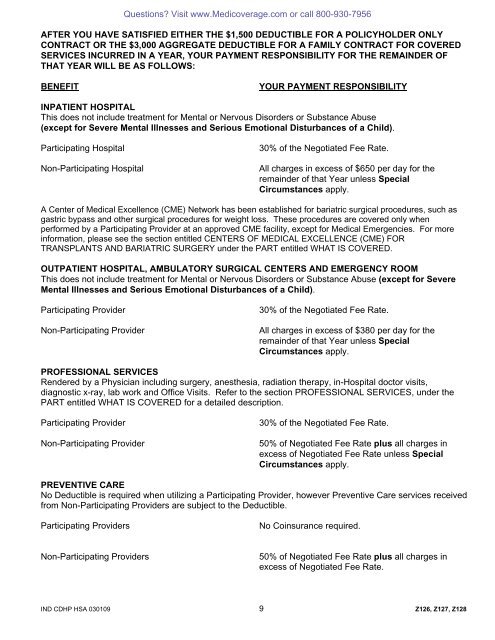
Questions? Visit www.<strong>Medicoverage</strong>.com or call 800-930-7956AFTER YOU HAVE SATISFIED EITHER THE $1,500 DEDUCTIBLE FOR A POLICYHOLDER ONLYCONTRACT OR THE $3,000 AGGREGATE DEDUCTIBLE FOR A FAMILY CONTRACT FOR COVEREDSERVICES INCURRED IN A YEAR, YOUR PAYMENT RESPONSIBILITY FOR THE REMAINDER OFTHAT YEAR WILL BE AS FOLLOWS:BENEFITYOUR PAYMENT RESPONSIBILITYINPATIENT HOSPITALThis does not include treatment for Mental or Nervous Disorders or Substance Abuse(except for Severe Mental Illnesses and Serious Emotional Disturbances of a Child).Participating HospitalNon-Participating Hospital30% of the Negotiated Fee Rate.All charges in excess of $650 per day for theremainder of that Year unless SpecialCircumstances apply.A Center of Medical Excellence (CME) Network has been established for bariatric surgical procedures, such asgastric bypass and other surgical procedures for weight loss. These procedures are covered only whenperformed by a Participating Provider at an approved CME facility, except for Medical Emergencies. For moreinformation, please see the section entitled CENTERS OF MEDI<strong>CA</strong>L EXCELLENCE (CME) FORTRANSPLANTS AND BARIATRIC SURGERY under the PART entitled WHAT IS COVERED.OUTPATIENT HOSPITAL, AMBULATORY SURGI<strong>CA</strong>L CENTERS AND EMERGENCY ROOMThis does not include treatment for Mental or Nervous Disorders or Substance Abuse (except for SevereMental Illnesses and Serious Emotional Disturbances of a Child).Participating ProviderNon-Participating Provider30% of the Negotiated Fee Rate.All charges in excess of $380 per day for theremainder of that Year unless SpecialCircumstances apply.PROFESSIONAL SERVICESRendered by a Physician including surgery, anesthesia, radiation therapy, in-Hospital doctor visits,diagnostic x-ray, lab work and Office Visits. Refer to the section PROFESSIONAL SERVICES, under thePART entitled WHAT IS COVERED for a detailed description.Participating ProviderNon-Participating Provider30% of the Negotiated Fee Rate.50% of Negotiated Fee Rate plus all charges inexcess of Negotiated Fee Rate unless SpecialCircumstances apply.PREVENTIVE <strong>CA</strong>RENo Deductible is required when utilizing a Participating Provider, however Preventive Care services receivedfrom Non-Participating Providers are subject to the Deductible.Participating ProvidersNo Coinsurance required.Non-Participating Providers50% of Negotiated Fee Rate plus all charges inexcess of Negotiated Fee Rate.IND CDHP <strong>HSA</strong> 030109 9 Z126, Z127, Z128