URTI CPG Booklet_consensus (English - pdf - 762 Kb) - MSO-HNS
URTI CPG Booklet_consensus (English - pdf - 762 Kb) - MSO-HNS
URTI CPG Booklet_consensus (English - pdf - 762 Kb) - MSO-HNS
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
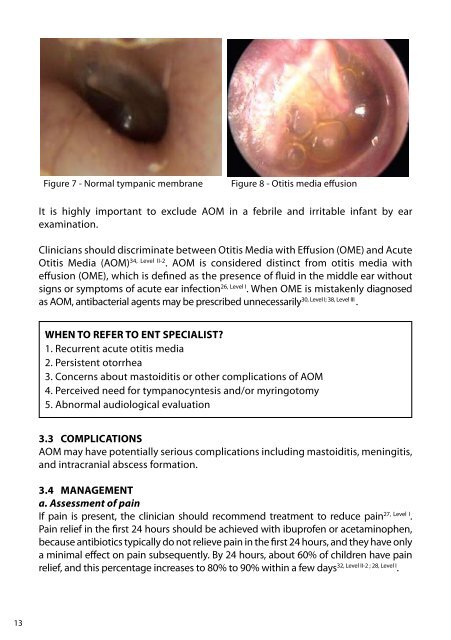
Figure 7 - Normal tympanic membraneFigure 8 - Otitis media effusionIt is highly important to exclude AOM in a febrile and irritable infant by earexamination.Clinicians should discriminate between Otitis Media with Effusion (OME) and AcuteOtitis Media (AOM) 34, Level II-2 . AOM is considered distinct from otitis media witheffusion (OME), which is defined as the presence of fluid in the middle ear withoutsigns or symptoms of acute ear infection 26, Level I . When OME is mistakenly diagnosedas AOM, antibacterial agents may be prescribed unnecessarily 30, Level I; 38, Level III .WHEN TO REFER TO ENT SPECIALIST?1. Recurrent acute otitis media2. Persistent otorrhea3. Concerns about mastoiditis or other complications of AOM4. Perceived need for tympanocyntesis and/or myringotomy5. Abnormal audiological evaluation3.3 COMPLICATIONSAOM may have potentially serious complications including mastoiditis, meningitis,and intracranial abscess formation.3.4 MANAGEMENTa. Assessment of painIf pain is present, the clinician should recommend treatment to reduce pain 27, Level I .Pain relief in the first 24 hours should be achieved with ibuprofen or acetaminophen,because antibiotics typically do not relieve pain in the first 24 hours, and they have onlya minimal effect on pain subsequently. By 24 hours, about 60% of children have painrelief, and this percentage increases to 80% to 90% within a few days 32, Level II-2 ; 28, Level I .13