PARTICIPANT info/MEDICAL inforMATIONLast Name:__________________________________________________________________ First Name:________________________________ MI:________INSURANCE AND MEDICAL inforMAtion:Carrier/Plan Name: ___________________________________________________________ Group #: ____________________________________________Name <strong>of</strong> Insured: _____________________________________________________________ Relationship to Participant: ________________________PREFERRED proVIDer:Physician: _____________________________________________________________________________Phone:_______________________________________Preferred Hospital: _________________________________________________________________________________________________________________Is participant cover by insurance: Yes NoI HAVE inCLUDED A COPY <strong>of</strong> MY ChilD IMMuniZAtion reCORDS.Is the Member/Participant currently taking prescription/over the counter medications? Yes NoList Medication/Dosage/Purpose: _____________________________________________________________________________________________________Any condition requiring special care? Yes No(e.g. Diabetes, Gastrointestinal, Motor Disorder, Seizures, ADHD, Autism, Cognitive Disorder, Asthma, etc.)If yes, please specify: ____________________________________________________________________________________________________________________Has the Member/Participant had surgeries, illness, or any severe injuries? Yes NoIf yes, please specify: ____________________________________________________________________________________________________________________Please provide information we may not have asked that you feel is important for us to know as we incorporateyour child into our program ___________________________________________________________________________________________________________Does the member/participant have allergies? Yes No (e.g. food, medication, seasonal, etc.)Describe all known allergies in detail: ________________________________________________________________________________________________Does member/participant have dietary restrictions? Yes NoExplain Dietary Restrictions: ___________________________________________________________________________________________________________WAIVerS and AuthoriZAtion for treATMentThe health history is complete and accurate and participant has permission to engage in all activities unless otherwise specified in writing. Iunderstand that the <strong>YMCA</strong> <strong>of</strong> <strong>Greater</strong> <strong>Charlotte</strong> assumes no responsibility for injuries or illness which my child may sustain as a result <strong>of</strong> his/herparticipation in Summer Camp, athletics, sports programs, the use <strong>of</strong> any equipment, exercise or other activities. I expressly acknowledge that mychild has been medically cleared to participate in vigorous physical activities. I also understand that there is a risk <strong>of</strong> injury while participating inphysical activities. I agree to hold harmless the <strong>YMCA</strong>, its staff and volunteers for accidents <strong>of</strong> injuries arising out <strong>of</strong> my child’s participation inactivity.While the <strong>YMCA</strong> <strong>of</strong> <strong>Greater</strong> <strong>Charlotte</strong> will make every effort to provide reasonable accommodations for mentally and physically challenged children,we will not enroll children who are (1) <strong>of</strong> danger to themselves, (2) <strong>of</strong> danger to others, (3) a disruption to the normal activities making itunreasonably difficult for other children to enjoy the day camp programs. Any <strong>of</strong> the above reasons will be grounds for dismissal from the program.The <strong>YMCA</strong> follows the guidelines <strong>of</strong> the ADA. If my child requires special accommodations, I understand that I must contact the camp director prior tomy child’s participation in the program.I agree to have my child examined medically within a reasonable time period by family physician stating he/she is free from communicable disease andhas not been exposed to such. I hereby give my permission to the medical personnel selected by the <strong>YMCA</strong> director to order x-rays, routine tests,treatment; to release any records necessary for insurance purposes, and to provide or arrange necessary related transportation for myself/or mychild. In the event that I cannot be reached in an emergency, I herby give permission to the physician selected by the <strong>YMCA</strong> director to secure andadminister treatment including hospitalization for my child. I understand that no accident or medical insurance is provided with this activity.I give my consent for my child to leave the <strong>YMCA</strong> site, participate in authorized <strong>YMCA</strong> trips, swim at approved facilities and to ride in authorizedvehicles for the purpose <strong>of</strong> transportation in connection with the <strong>YMCA</strong> program.PRINT NAME: ___________________________________________________________________________________ DATE: ____________________________SIGNATURE: ________________________________________________________________________________________________________________________
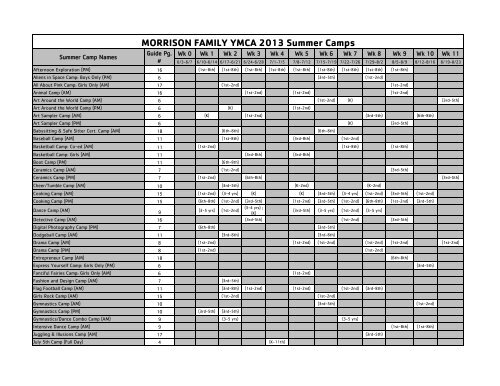
Summer Camp NamesWk 0 Wk 1 Wk 2 Wk 3 Wk 4 Wk 5 Wk 6 Wk 7 Wk 8 Wk 9 Wk 10 Wk 116/3-6/7 6/10-6/14 6/17-6/21 6/24-6/28 7/1-7/5 7/8-7/12 7/15-7/19 7/22-7/26 7/29-8/2 8/5-8/9 8/12-8/16 8/19-8/23Afternoon Exploration (PM) 16 (1st-8th) (1st-8th) (1st-8th) (1st-8th) (1st-8th) (1st-8th) (1st-8th) (1st-8th) (1st-8th)Aliens in Space Camp: Boys Only (PM) 6 (3rd-5th) (1st-2nd)All About Pink Camp: Girls Only (AM) 17 (1st-2nd) (1st-2nd)Animal Camp (AM) 16 (1st-2nd) (1st-2nd) (1st-2nd)Art Around the World Camp (AM) 6 (1st-2nd) (K) (3rd-5th)Art Around the World Camp (PM) 6 (K) (1st-2nd)Art Sampler Camp (AM) 6 (K) (1st-2nd) (3rd-5th) (6th-8th)Art Sampler Camp (PM) 6 (K) (3rd-5th)Babysitting & Safe Sitter Cert. Camp (AM) 18 (6th-8th) (6th-8th)Baseball Camp (AM) 11 (1st-8th) (3rd-8th) (1st-2nd)Basketball Camp: Co-ed (AM) 11 (1st-2nd) (1st-8th) (1st-8th)Basketball Camp: Girls (AM) 11 (3rd-8th) (3rd-8th)Boot Camp (PM) 11 (6th-8th)Ceramics Camp (AM) 7 (1st-2nd) (3rd-5th)Ceramics Camp (PM) 7 (1st-2nd) (6th-8th) (3rd-5th)Cheer/Tumble Camp (AM) 10 (3rd-5th) (K-2nd) (K-2nd)Cooking Camp (AM) 15 (1st-2nd) (3-4 yrs) (K) (K) (3rd-5th) (3-4 yrs) (1st-2nd) (3rd-5th) (1st-2nd)Cooking Camp (PM) 15 (6th-8th) (1st-2nd) (3rd-5th) (1st-2nd) (3rd-5th) (1st-2nd) (6th-8th) (1st-2nd) (3rd-5th)Dance Camp (AM)9(3-5 yrs) (1st-2nd)(3-4 yrs) ;(K)(3rd-5th) (3-5 yrs) (1st-2nd) (3-5 yrs)Detective Camp (AM) 16 (3rd-5th) (1st-2nd) (3rd-5th)Digital Photography Camp (PM) 7 (6th-8th) (3rd-5th)Dodgeball Camp (AM) 11 (3rd-8th) (3rd-8th)Drama Camp (AM) 8 (1st-2nd) (1st-2nd) (1st-2nd) (1st-2nd) (1st-2nd) (1st-2nd)Drama Camp (PM) 8 (1st-2nd) (1st-2nd)Entrepreneur Camp (AM) 18 (6th-8th)Express Yourself Camp: Girls Only (PM) 6 (3rd-5th)Fanciful Fairies Camp: Girls Only (AM) 6 (1st-2nd)Fashion and Design Camp (AM) 7 (3rd-5th)Flag Football Camp (AM) 11 (3rd-8th) (1st-2nd) (1st-2nd) (1st-2nd) (3rd-8th)Girls Rock Camp (AM) 15 (1st-2nd) (1st-2nd)Gymnastics Camp (AM) 10 (3rd-5th) (1st-2nd)Gymnastics Camp (PM) 10 (3rd-5th) (3rd-5th)<strong>MORRISON</strong> <strong>FAMILY</strong> <strong>YMCA</strong> 2013 Summer CampsGuide Pg.#Gymnastics/Dance Combo Camp (AM) 9 (3-5 yrs) (3-5 yrs)Intensive Dance Camp (AM) 9 (1st-8th) (1st-8th)Juggling & Illusions Camp (AM) 17 (3rd-5th)July 5th Camp (Full Day) 4 (K-11th)