Wellesley College Health History Form
Wellesley College Health History Form
Wellesley College Health History Form

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
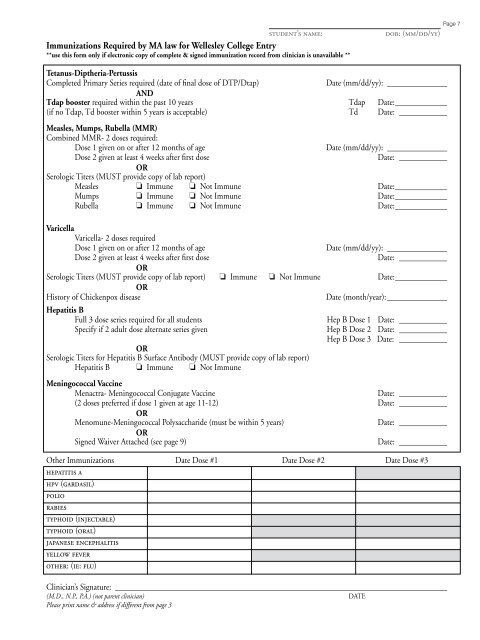
student’s name:Immunizations Required by MA law for <strong>Wellesley</strong> <strong>College</strong> Entry**use this form only if electronic copy of complete & signed immunization record from clinician is unavailable **dob: (mm/dd/yy)Page 7Tetanus-Diptheria-PertussisCompleted Primary Series required (date of final dose of DTP/Dtap)Date (mm/dd/yy): ________________ANDTdap booster required within the past 10 years Tdap Date:______________(if no Tdap, Td booster within 5 years is acceptable) Td Date: _____________Measles, Mumps, Rubella (MMR)Combined MMR- 2 doses required:Dose 1 given on or after 12 months of ageDate (mm/dd/yy): ________________Dose 2 given at least 4 weeks after first doseDate: _____________ORSerologic Titers (MUST provide copy of lab report)Measles ❏ Immune ❏ Not Immune Date:______________Mumps ❏ Immune ❏ Not Immune Date:______________Rubella ❏ Immune ❏ Not Immune Date:______________VaricellaVaricella- 2 doses requiredDose 1 given on or after 12 months of ageDate (mm/dd/yy): ________________Dose 2 given at least 4 weeks after first doseDate: _____________ORSerologic Titers (MUST provide copy of lab report) ❏ Immune ❏ Not Immune Date:______________OR<strong>History</strong> of Chickenpox diseaseHepatitis BFull 3 dose series required for all studentsSpecify if 2 adult dose alternate series givenORSerologic Titers for Hepatitis B Surface Antibody (MUST provide copy of lab report)Hepatitis B ❏ Immune ❏ Not ImmuneDate (month/year):________________Hep B Dose 1 Date: _____________Hep B Dose 2 Date: _____________Hep B Dose 3 Date: _____________Meningococcal VaccineMenactra- Meningococcal Conjugate VaccineDate: _____________(2 doses preferred if dose 1 given at age 11-12) Date: _____________ORMenomune-Meningococcal Polysaccharide (must be within 5 years)Date: _____________ORSigned Waiver Attached (see page 9)Date: _____________Other Immunizations Date Dose #1 Date Dose #2 Date Dose #3hepatitis ahpv (gardasil)poliorabiestyphoid (injectable)typhoid (oral)japanese encephalitisyellow feverother: (ie: flu)Clinician’s Signature:____________________________________________________________________________________(M.D., N.P., P.A.) (not parent clinician)DATEPlease print name & address if different from page 3