Scientific Article |Utility of Upper Endoscopy and Colonoscopy inEvaluating Gastrointestinal Luminal Wall ThickeningFound on Computed TomographyMuhammad Sohaib Karim, MDMax C. Miranda, MDJohn M. Shamma’a, MDStephan U. Goebel, MDUma Sundaram, MDSection of Digestive Diseases,Department of Medicine<strong>West</strong> <strong>Virginia</strong> University School ofMedicine, MorgantownAbstractBackground: Abdominal computedtomography (CT) scans are frequentlyperformed for a variety of abdominalcomplaints. Not infrequently, bowel wallthickening noted on these radiographicstudies of the gastrointestinal (GI) tractprompt further endoscopic evaluation. It isunclear whether the costs and risks ofendoscopy are justified given thesubsequent yield on endoscopicexamination of this radiological finding.Materials and Methods: A retrospectivestudy was done on patients referred to theDigestive Diseases section of a tertiary levelhospital for abnormal findings seen on CTduring the study period. These patientswere seen over one year and their chartsreviewed. The items reviewed in the chartswere: age, gender, chief complaint, physicalfindings, ordering location, CT scanindication, CT scan abnormality, endoscopicfindings, and the time interval between CTscan and endoscopic procedure.Results: A total of 169 patients withbowel wall thickening that proceeded to anendoscopy were identified. The average agefor the patients was 18 to 89 with a mean of55 years. Females comprised 59% of thepatients. The mean period from the time ofthe CT scan to endoscopy was 32 days. Inthe upper GI tract, 39 patients had bowelwall thickening. Of these, 25 had abnormalpathology on subsequent endoscopycorrelating with the radiological findings. Inthe lower GI tract, 109 patients had bowelwall thickening. Of these, 36 had abnormalfindings on the subsequent endoscopy. Inthis group, 10% was found to be ofneoplastic origin upon further work-up. Thepositive predictive value (PPV) for bowelwall thickening in the UGI tract was 64%. Inthe lower GI tract, the PPV was 33%Conclusion: Thickening of thegastrointestinal tract is not uncommonlynoted on abdominal CT scans. The resultantendoscopic evaluations of these findingsappear to yield more when these changesare seen in the upper GI tract as comparedto the lower GI tract. Luminal wall thickeningin the upper GI tract seen on CT is a veryuseful predictor of pathology (PPV=64%).For colonic wall thickening seen on CT, thePPV was only 33%. Nevertheless, werecommend direct visualization as 10% ofthese findings were found to be malignancieson follow-up.IntroductionComputed Tomography (CT) isan increasingly used modality inthe initial work-up of patients whopresent with abdominal pain. CTscans are known to be an effectivediagnostic tool in the evaluationof abdominal pathology such astumors, obstruction, strictures, etc.In the initial CT scan of theabdomen and the pelvis, intraluminalpathology, if found, is alwaysmentioned. Substantial information,both abnormal findings andnormal variants can be gleaned bya radiologist from studying bowelappearance. One of the most commonfindings reported on abdominalCT studies is thickening of thebowel wall. Bowel wall thickeningmay be a normal finding, or maybe indicative of pathology such asinflammatory bowel disease or anacute inflammatory process. 1-3 Inaddition, intraluminal thickeningas a radiological finding may alsoshow esophageal pathologies upondirect visualization if found in theupper GI tract. 4-5 Furthermore,bowel wall inflammation causedby infectious etiologies is wellknown to manifest as bowelwall thickening on CT scans. 6Bowel wall thickening is defined asincreased bowel wall diameter abovethe upper limit of normal which is 1-2mm for the small bowel, and 2-3 mmfor the colon. However, some studiesseem to suggest that a large portion(20% to 60%) of patients with colonicbowel wall thickening seen on a CTscan, are found to have a normalendoscopic exam upon follow up. 3,4,9,11To clarify the indication forendoscopy, we therefore decidedto do a retrospective reviewof endoscopic reports of thosepatients that had been referred tothe Section of Digestive Diseasesfor bowel wall thickening seenon abdominal CT scans.Materials and Methods<strong>Medical</strong> records of 169 patientsreferred to a tertiary level hospital forabnormal findings seen on CT thatthereafter received an endoscopicevaluation were identified. Thesepatients were seen over a period ofone year and their charts reviewed.The items reviewed in the chartswere age, gender, chief complaint,physical findings, ordering location,CT scan indication, CT scanabnormality, endoscopic findingsand the time interval between CTscan and endoscopic procedure.ResultsWe studied a total of 169 patients.The average age of the patients inthis study ranged from 18 to 89with a mean of 55 years. Of these,41% were male (Table 1). Thetime period between CT scan andendoscopy ranged from the sameday to a maximum of 176 days witha mean of 32 days. In this sample,the most common chief complaintwas abdominal pain (66%), followedby gastrointestinal bleeding (10%),history of non-abdominal cancer(4%), diarrhea (3%), dysphagia (2%),16 <strong>West</strong> <strong>Virginia</strong> <strong>Medical</strong> Journal
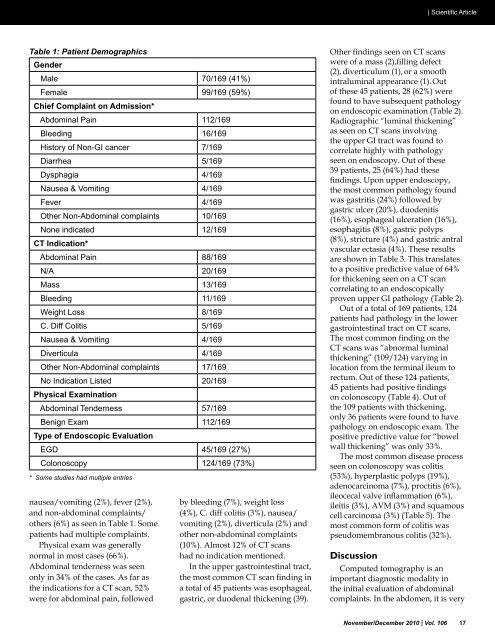
| Scientific ArticleTable 1: Patient DemographicsGenderMale 70/169 (41%)Female 99/169 (59%)Chief Complaint on Admission*Abdominal Pain 112/169Bleeding 16/169History of Non-GI cancer 7/169Diarrhea 5/169Dysphagia 4/169Nausea & Vomiting 4/169Fever 4/169Other Non-Abdominal complaints 10/169None indicated 12/169CT Indication*Abdominal Pain 88/169N/A 20/169Mass 13/169Bleeding 11/169Weight Loss 8/169C. Diff Colitis 5/169Nausea & Vomiting 4/169Diverticula 4/169Other Non-Abdominal complaints 17/169No Indication Listed 20/169Physical ExaminationAbdominal Tenderness 57/169Benign Exam 112/169Type of Endoscopic EvaluationEGD 45/169 (27%)Colonoscopy 124/169 (73%)* Some studies had multiple entriesnausea/vomiting (2%), fever (2%),and non-abdominal complaints/others (6%) as seen in Table 1. Somepatients had multiple complaints.Physical exam was generallynormal in most cases (66%).Abdominal tenderness was seenonly in 34% of the cases. As far asthe indications for a CT scan, 52%were for abdominal pain, followedby bleeding (7%), weight loss(4%), C. diff colitis (3%), nausea/vomiting (2%), diverticula (2%) andother non-abdominal complaints(10%). Almost 12% of CT scanshad no indication mentioned.In the upper gastrointestinal tract,the most common CT scan finding ina total of 45 patients was esophageal,gastric, or duodenal thickening (39).Other findings seen on CT scanswere of a mass (2),filling defect(2), diverticulum (1), or a smoothintraluminal appearance (1). Outof these 45 patients, 28 (62%) werefound to have subsequent pathologyon endoscopic examination (Table 2).Radiographic “luminal thickening”as seen on CT scans involvingthe upper GI tract was found tocorrelate highly with pathologyseen on endoscopy. Out of these39 patients, 25 (64%) had thesefindings. Upon upper endoscopy,the most common pathology foundwas gastritis (24%) followed bygastric ulcer (20%), duodenitis(16%), esophageal ulceration (16%),esophagitis (8%), gastric polyps(8%), stricture (4%) and gastric antralvascular ectasia (4%). These resultsare shown in Table 3. This translatesto a positive predictive value of 64%for thickening seen on a CT scancorrelating to an endoscopicallyproven upper GI pathology (Table 2).Out of a total of 169 patients, 124patients had pathology in the lowergastrointestinal tract on CT scans.The most common finding on theCT scans was “abnormal luminalthickening” (109/124) varying inlocation from the terminal ileum torectum. Out of these 124 patients,45 patients had positive findingson colonoscopy (Table 4). Out ofthe 109 patients with thickening,only 36 patients were found to havepathology on endoscopic exam. Thepositive predictive value for “bowelwall thickening” was only 33%.The most common disease processseen on colonoscopy was colitis(53%), hyperplastic polyps (19%),adenocarcinoma (7%), proctitis (6%),ileocecal valve inflammation (6%),ileitis (3%), AVM (3%) and squamouscell carcinoma (3%) (Table 5). Themost common form of colitis waspseudomembranous colitis (32%).DiscussionComputed tomography is animportant diagnostic modality inthe initial evaluation of abdominalcomplaints. In the abdomen, it is veryNovember/December 2010 | Vol. 106 17