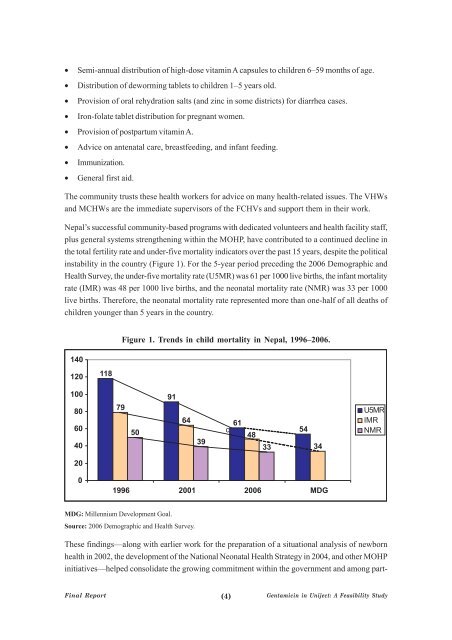
• Semi-annual distribution <strong>of</strong> high-dose vitam<strong>in</strong> A capsules to children 6–59 months <strong>of</strong> age.• Distribution <strong>of</strong> deworm<strong>in</strong>g tablets to children 1–5 years old.• Provision <strong>of</strong> oral rehydration salts (and z<strong>in</strong>c <strong>in</strong> some districts) for diarrhea cases.• Iron-folate tablet distribution for pregnant women.• Provision <strong>of</strong> postpartum vitam<strong>in</strong> A.• Advice on antenatal care, breastfeed<strong>in</strong>g, and <strong>in</strong>fant feed<strong>in</strong>g.• Immunization.• General first aid.The community trusts <strong>the</strong>se health workers for advice on many health-related issues. The VHWsand MCHWs are <strong>the</strong> immediate supervisors <strong>of</strong> <strong>the</strong> FCHVs and support <strong>the</strong>m <strong>in</strong> <strong>the</strong>ir work.Nepal’s successful community-based programs with dedicated volunteers and health facility staff,plus general systems streng<strong>the</strong>n<strong>in</strong>g with<strong>in</strong> <strong>the</strong> MOHP, have contributed to a cont<strong>in</strong>ued decl<strong>in</strong>e <strong>in</strong><strong>the</strong> total fertility rate and under-five mortality <strong>in</strong>dicators over <strong>the</strong> past 15 years, despite <strong>the</strong> political<strong>in</strong>stability <strong>in</strong> <strong>the</strong> country (Figure 1). For <strong>the</strong> 5-year period preced<strong>in</strong>g <strong>the</strong> 2006 Demographic andHealth Survey, <strong>the</strong> under-five mortality rate (U5MR) was 61 per 1000 live births, <strong>the</strong> <strong>in</strong>fant mortalityrate (IMR) was 48 per 1000 live births, and <strong>the</strong> neonatal mortality rate (NMR) was 33 per 1000live births. Therefore, <strong>the</strong> neonatal mortality rate represented more than one-half <strong>of</strong> all deaths <strong>of</strong>children younger than 5 years <strong>in</strong> <strong>the</strong> country.Figure 1. Trends <strong>in</strong> child mortality <strong>in</strong> Nepal, 1996–2006.MDG: Millennium Development Goal.Source: 2006 Demographic and Health Survey.These f<strong>in</strong>d<strong>in</strong>gs—along with earlier work for <strong>the</strong> preparation <strong>of</strong> a situational analysis <strong>of</strong> newbornhealth <strong>in</strong> 2002, <strong>the</strong> development <strong>of</strong> <strong>the</strong> National Neonatal Health Strategy <strong>in</strong> 2004, and o<strong>the</strong>r MOHP<strong>in</strong>itiatives—helped consolidate <strong>the</strong> grow<strong>in</strong>g commitment with<strong>in</strong> <strong>the</strong> government and among part-F<strong>in</strong>al Report(4) <strong>Gentamic<strong>in</strong></strong> <strong>in</strong> <strong>Uniject</strong>: A Feasibility Study
ners for improv<strong>in</strong>g newborn health and survival. In order to achieve Millennium Development Goal4 (Reduce Child Mortality), it was apparent that <strong>the</strong> ma<strong>in</strong> killers <strong>of</strong> neonates (<strong>in</strong>fection, birth asphyxia,and <strong>the</strong> complications <strong>of</strong> low birth weight and prematurity) must be addressed urgently.In 2004, <strong>the</strong> MOHP <strong>in</strong>troduced a community-based pilot program <strong>in</strong> Morang district, a large district<strong>in</strong> <strong>the</strong> eastern terai (flatland) <strong>of</strong> Nepal, to address <strong>the</strong> high mortality attributed to neonatal <strong>in</strong>fectionsand sepsis. This <strong>in</strong>itiative was implemented with technical support and oversight from <strong>the</strong> JohnSnow, Inc. (known as JSI) Research and Tra<strong>in</strong><strong>in</strong>g Institute and fund<strong>in</strong>g from <strong>the</strong> Sav<strong>in</strong>g NewbornLives program <strong>of</strong> Save <strong>the</strong> Children with support from <strong>the</strong> Bill & Mel<strong>in</strong>da Gates Foundation. TheUnited States Agency for International Development (USAID) provided additional f<strong>in</strong>ancial andtechnical support and facilitated later expansion <strong>of</strong> <strong>the</strong> program to <strong>the</strong> whole district through <strong>the</strong>Nepal Family Health Program (NFHP). It was implemented entirely through <strong>the</strong> exist<strong>in</strong>g publichealth system <strong>of</strong> <strong>the</strong> MOHP, under <strong>the</strong> direction <strong>of</strong> <strong>the</strong> District Public Health Office (DPHO).This pilot program was called <strong>the</strong> Morang Innovative Neonatal Intervention (MINI). The publichealth services <strong>of</strong> Morang district are coord<strong>in</strong>ated through <strong>the</strong> DPHO located <strong>in</strong> <strong>the</strong> district headquarters,Biratnagar. Accord<strong>in</strong>g to <strong>the</strong> national health policy <strong>of</strong> Nepal, each <strong>of</strong> <strong>the</strong> 65 VDCs <strong>of</strong>Morang have at least one health <strong>in</strong>stitution, and <strong>the</strong>ir distribution is as follows: 7 primary health carecenters, 10 health posts, and 49 SHPs.The FCHVs <strong>in</strong> Morang had also been previously tra<strong>in</strong>ed on <strong>the</strong> assessment and management <strong>of</strong>children with pneumonia. S<strong>in</strong>ce 1995, FCHVs have treated children 2 months to 5 years <strong>of</strong> agewith oral pediatric cotrimoxazole (cotrimoxazole-p) tablets for pneumonia. They are familiar with<strong>the</strong> use <strong>of</strong> a timer to count respiratory rate and assessment <strong>of</strong> young <strong>in</strong>fants for danger signs. Theyhave been tra<strong>in</strong>ed to refer sick young <strong>in</strong>fants younger than 2 months and those with “severe pneumonia”to <strong>the</strong> nearest health facility for fur<strong>the</strong>r assessment and treatment.The MINI program tra<strong>in</strong>ed and supported <strong>the</strong> FCHVs to visit homes <strong>in</strong> <strong>the</strong>ir villages with<strong>in</strong> 24hours <strong>of</strong> birth to weigh <strong>the</strong> newborn, prepare a simple record <strong>of</strong> <strong>the</strong> birth, assess <strong>the</strong> neonate forany danger signs <strong>of</strong> <strong>in</strong>fection, and alert <strong>the</strong> mo<strong>the</strong>r and caretakers to call <strong>the</strong> FCHV immediatelyfor reassessment if any danger signs occur. FCHVs also teach families about essential newborncare (ENC) and additional care needed for low weight babies. Through <strong>the</strong> MINI program, FCHVs<strong>in</strong> Morang have also been tra<strong>in</strong>ed to identify and <strong>in</strong>itiate management <strong>of</strong> both local bacterial <strong>in</strong>fectionsand possible severe bacterial <strong>in</strong>fections (PSBIs) <strong>in</strong> young <strong>in</strong>fants (0–59 days <strong>of</strong> age).While FCHVs are not asked to attend deliveries as part <strong>of</strong> <strong>the</strong> MINI <strong>in</strong>tervention, <strong>the</strong>y are aware<strong>of</strong> <strong>the</strong> pregnant women <strong>in</strong> <strong>the</strong>ir communities, as <strong>the</strong>y ma<strong>in</strong>ta<strong>in</strong> a pregnancy surveillance registerand provide iron-folate tablets to pregnant women. Dur<strong>in</strong>g <strong>the</strong>se antenatal contacts, FCHVs providecounsel<strong>in</strong>g on birth preparedness and recommend that women seek antenatal care from <strong>the</strong>health facility staff (<strong>in</strong>clud<strong>in</strong>g tetanus toxoid <strong>in</strong>jections). In addition, through MINI, FCHVs talkabout ENC practices and describe <strong>the</strong> danger signs <strong>of</strong> neonatal <strong>in</strong>fections, and leave colorful <strong>in</strong>formationflyers with families that describe <strong>the</strong>se danger signs. FCHVs also ask families to <strong>in</strong>form<strong>the</strong>m immediately after <strong>the</strong> birth, so <strong>the</strong>y can return to <strong>the</strong> home and conduct an <strong>in</strong>itial assessment<strong>of</strong> <strong>the</strong> newborn.<strong>Gentamic<strong>in</strong></strong> <strong>in</strong> <strong>Uniject</strong>: A Feasibility Study(5)F<strong>in</strong>al Report