TABLE 4 Developmental Milestones in the First 2 Years of LifeMilestoneAverage Age of Developmental ImplicationsAttainment, moGross motorHead steady in sitting 2.0 Allows more visual interactionPull to sit, no head lag 3.0 Muscle toneH<strong>and</strong>s together in midline 3.0 Self-discoveryAsymmetric tonic neck reflex gone 4.0 Child can inspect h<strong>and</strong>s in midlineSits without support 6.0 Increasing explorationRolls back to stomach 6.5 Truncal flexion, risk of fallsWalks alone 12.0 Exploration, control of proximity toparentsRuns 16.0 Supervision more difficultFine motorGrasps rattle 3.5 Object useReaches for objects 4.0 Visuomotor coordinationPalmar grasp gone 4.0 Voluntary releaseTransfers object h<strong>and</strong> to h<strong>and</strong> 5.5 Comparison of objectsThumb-finger grasp 8.0 Able to explore small objectsTurns pages of book 12.0 Increasing autonomy during book timeScribbles 13.0 Visuomotor coordinationBuilds tower of 2 cubes 15.0 Uses objects in combinationBuilds tower of 6 cubes 22.0 Requires visual, gross, <strong>and</strong> fine motorcoordinationCommunication <strong>and</strong> languageSmiles in response to face, voice 1.5 Child more active social participantMonosyllabic babble 6.0 Experimentation with sound, tactile senseInhibits to “no” 7.0 Response to tone (nonverbal)Follows 1-step comm<strong>and</strong> with gesture 7.0 Nonverbal communicationFollows 1-step comm<strong>and</strong> without10.0 Verbal receptive languagegesture (eg, “Give it to me”)Speaks first real word 12.0 Beginning of labelingSpeaks 4–6 words 15.0 Acquisition of object <strong>and</strong> personal namesSpeaks 10–15 words 18.0 Acquisition of object <strong>and</strong> personal namesSpeaks 2-word sentences (eg, “Mommyshoe”)19.0 Beginning grammaticization, correspondswith vocabulary of 50 wordsCognitiveStares momentarily at spot whereobject disappeared (eg, yarn ball2.0 Lack of object permanence (out of sight,out of mind)dropped)Stares at own h<strong>and</strong> 4.0 Self-discovery, cause <strong>and</strong> effectBangs 2 cubes 8.0 Active comparison of objectsUncovers toy (after seeing it hidden) 8.0 Object permanenceEgocentric pretend play (eg, pretends 12.0 Beginning symbolic thoughtto drink from cup)Uses stick to reach toy 17.0 Able to link actions to solve problemsPretend play with doll (gives doll bottle) 17.0 Symbolic thoughtModified from: Behrman RE, Jenson HB, Kliegman R, eds. Nelson Textbook of Pediatrics. 16th ed. Philadelphia, PA: Saunders;2003.children. These tympanograms aregenerally not classified as A, B, or C butrather as peak or no peak.Evoked Otoacoustic EmissionsEvoked otoacoustic emissions (OAEs)are acoustic signals generated fromwithin the cochlea that travel in a reversedirection through the middle-earspace <strong>and</strong> tympanic membrane out tothe ear canal. These signals are generatedin response to an auditory stimulus,either clicks or tone bursts. Thesignals may be detected with a verysensitive microphone/probe systemplaced in the external ear canal. TheOAE test allows for individual ear assessment,can be performed quickly atany age, <strong>and</strong> does not depend onwhether the child is asleep or awake.Mild degrees of motion artifact do notinterfere with test results; however,screening results are frequently influencedby the presence of middle-earpathologic abnormalities. The OAE testis an effective screening measure formiddle-ear abnormalities <strong>and</strong> for moderateor more severe degrees of hearingloss, because normal OAE responsesare not obtained if hearingthresholds are approximately 30- to40-dB hearing levels or higher. The automatedOAE screener provides a passfailreport; no test interpretation by anaudiologist is required. The OAE testdoes not further quantify hearing lossor hearing threshold level. The OAE testalso does not assess the integrity of theneural transmission of sound from theeighth nerve to the brainstem <strong>and</strong>,therefore, will miss auditory neuropathy<strong>and</strong> other neuronal abnormalities.Infants with such abnormalities willhave normal OAE test results but abnormalauditory brainstem response(ABR) test results. A “failed” OAE testonly implies that a hearing loss ofmore than 30 to 40 dB may exist or thatthe middle-ear status is abnormal.Automated ABROne objective physiologic means ofscreening hearing is the automatedABR. This instrument measures cochlearresponse in the 1- to 4-kHzrange with a broadb<strong>and</strong> click stimulusin each ear. Many ABR screening instrumentsincorporate built-in artifactrejection for myogenic, electrical, <strong>and</strong>environmental noise interference,which ensures that data collection ishalted if testing conditions are unfavorable.The automated screener providesa pass-fail report; no test interpretationby an audiologist is required.A “fail” report on an automated ABR impliesa hearing level of worse than 40 dB.Automated ABR can test each ear individually<strong>and</strong> can be performed on childrenof any age. Motion artifacts interferewith test results. For this reason, the test1256 FROM THE AMERICAN ACADEMY OF PEDIATRICSDownloaded from pediatrics.aappublications.org by Susan Panny on June 10, 2012
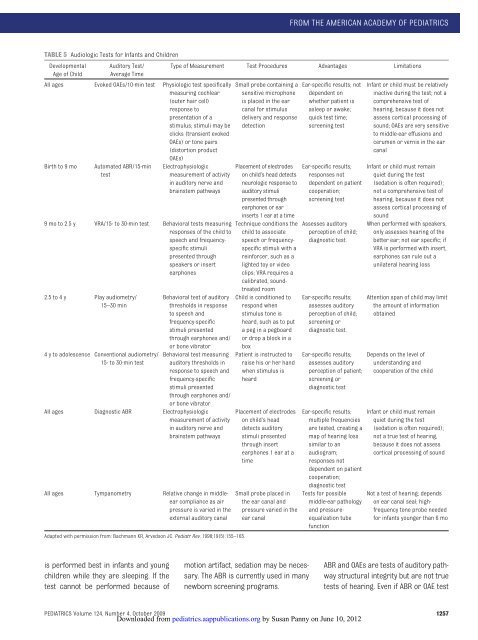
FROM THE AMERICAN ACADEMY OF PEDIATRICSTABLE 5 Audiologic Tests for Infants <strong>and</strong> ChildrenDevelopmentalAge of ChildAuditory Test/Average TimeType of Measurement Test Procedures Advantages LimitationsAll ages Evoked OAEs/10-min test Physiologic test specificallymeasuring cochlear(outer hair cell)response topresentation of astimulus; stimuli may beclicks (transient evokedOAEs) or tone pairs(distortion productOAEs)Birth to 9 moAutomated ABR/15-mintestElectrophysiologicmeasurement of activityin auditory nerve <strong>and</strong>brainstem pathways9 mo to 2.5 y VRA/15- to 30-min test Behavioral tests measuringresponses of the child tospeech <strong>and</strong> frequencyspecificstimulipresented throughspeakers or insertearphones2.5 to 4 y Play audiometry/15–30 min4 y to adolescence Conventional audiometry/15- to 30-min testBehavioral test of auditorythresholds in responseto speech <strong>and</strong>frequency-specificstimuli presentedthrough earphones <strong>and</strong>/or bone vibratorBehavioral test measuringauditory thresholds inresponse to speech <strong>and</strong>frequency-specificstimuli presentedthrough earphones <strong>and</strong>/or bone vibratorAll ages Diagnostic ABR Electrophysiologicmeasurement of activityin auditory nerve <strong>and</strong>brainstem pathwaysAll ages Tympanometry Relative change in middleearcompliance as airpressure is varied in theexternal auditory canalAdapted with permission from: Bachmann KR, Arvedson JC. Pediatr Rev. 1998;19(5):155–165.Small probe containing asensitive microphoneis placed in the earcanal for stimulusdelivery <strong>and</strong> responsedetectionPlacement of electrodeson child’s head detectsneurologic response toauditory stimulipresented throughearphones or earinserts 1 ear at a timeTechnique conditions thechild to associatespeech or frequencyspecificstimuli with areinforcer, such as alighted toy or videoclips; VRA requires acalibrated, soundtreatedroomChild is conditioned torespond whenstimulus tone isheard, such as to puta peg in a pegboardor drop a block in aboxPatient is instructed toraise his or her h<strong>and</strong>when stimulus isheardPlacement of electrodeson child’s headdetects auditorystimuli presentedthrough insertearphones 1 ear at atimeSmall probe placed inthe ear canal <strong>and</strong>pressure varied in theear canalEar-specific results; notdependent onwhether patient isasleep or awake;quick test time;screening testEar-specific results;responses notdependent on patientcooperation;screening testAssesses auditoryperception of child;diagnostic test.Ear-specific results;assesses auditoryperception of child;screening ordiagnostic test.Ear-specific results;assesses auditoryperception of patient;screening ordiagnostic testEar-specific results;multiple frequenciesare tested, creating amap of hearing losssimilar to anaudiogram;responses notdependent on patientcooperation;diagnostic testTests for possiblemiddle-ear pathology<strong>and</strong> pressureequalizationtubefunctionInfant or child must be relativelyinactive during the test; not acomprehensive test ofhearing, because it does notassess cortical processing ofsound; OAEs are very sensitiveto middle-ear effusions <strong>and</strong>cerumen or vernix in the earcanalInfant or child must remainquiet during the test(sedation is often required);not a comprehensive test ofhearing, because it does notassess cortical processing ofsoundWhen performed with speakers,only assesses hearing of thebetter ear; not ear specific; ifVRA is performed with insert,earphones can rule out aunilateral hearing lossAttention span of child may limitthe amount of informationobtainedDepends on the level ofunderst<strong>and</strong>ing <strong>and</strong>cooperation of the childInfant or child must remainquiet during the test(sedation is often required);not a true test of hearing,because it does not assesscortical processing of soundNot a test of hearing; dependson ear canal seal; highfrequencytone probe neededfor infants younger than 6 mois performed best in infants <strong>and</strong> youngchildren while they are sleeping. If thetest cannot be performed because ofmotion artifact, sedation may be necessary.The ABR is currently used in manynewborn screening programs.ABR <strong>and</strong> OAEs are tests of auditory pathwaystructural integrity but are not truetests of hearing. Even if ABR or OAE testPEDIATRICS Volume 124, Number 4, October 2009 1257Downloaded from pediatrics.aappublications.org by Susan Panny on June 10, 2012