

ACOG Practice Bulletin No. 90: Asthma in Pregnancy
ACOG Practice Bulletin No. 90: Asthma in Pregnancy
ACOG Practice Bulletin No. 90: Asthma in Pregnancy
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
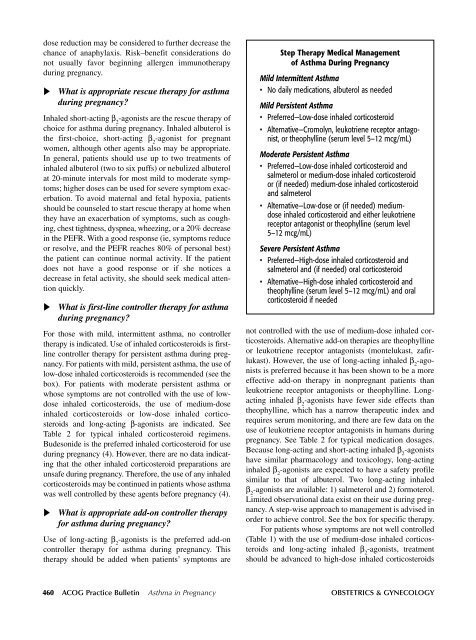
dose reduction may be considered to further decrease thechance of anaphylaxis. Risk–benefit considerations donot usually favor beg<strong>in</strong>n<strong>in</strong>g allergen immunotherapydur<strong>in</strong>g pregnancy.What is appropriate rescue therapy for asthmadur<strong>in</strong>g pregnancy?Inhaled short-act<strong>in</strong>g β 2-agonists are the rescue therapy ofchoice for asthma dur<strong>in</strong>g pregnancy. Inhaled albuterol isthe first-choice, short-act<strong>in</strong>g β 2-agonist for pregnantwomen, although other agents also may be appropriate.In general, patients should use up to two treatments of<strong>in</strong>haled albuterol (two to six puffs) or nebulized albuterolat 20-m<strong>in</strong>ute <strong>in</strong>tervals for most mild to moderate symptoms;higher doses can be used for severe symptom exacerbation.To avoid maternal and fetal hypoxia, patientsshould be counseled to start rescue therapy at home whenthey have an exacerbation of symptoms, such as cough<strong>in</strong>g,chest tightness, dyspnea, wheez<strong>in</strong>g, or a 20% decrease<strong>in</strong> the PEFR. With a good response (ie, symptoms reduceor resolve, and the PEFR reaches 80% of personal best)the patient can cont<strong>in</strong>ue normal activity. If the patientdoes not have a good response or if she notices adecrease <strong>in</strong> fetal activity, she should seek medical attentionquickly.What is first-l<strong>in</strong>e controller therapy for asthmadur<strong>in</strong>g pregnancy?For those with mild, <strong>in</strong>termittent asthma, no controllertherapy is <strong>in</strong>dicated. Use of <strong>in</strong>haled corticosteroids is firstl<strong>in</strong>econtroller therapy for persistent asthma dur<strong>in</strong>g pregnancy.For patients with mild, persistent asthma, the use oflow-dose <strong>in</strong>haled corticosteroids is recommended (see thebox). For patients with moderate persistent asthma orwhose symptoms are not controlled with the use of lowdose<strong>in</strong>haled corticosteroids, the use of medium-dose<strong>in</strong>haled corticosteroids or low-dose <strong>in</strong>haled corticosteroidsand long-act<strong>in</strong>g β-agonists are <strong>in</strong>dicated. SeeTable 2 for typical <strong>in</strong>haled corticosteroid regimens.Budesonide is the preferred <strong>in</strong>haled corticosteroid for usedur<strong>in</strong>g pregnancy (4). However, there are no data <strong>in</strong>dicat<strong>in</strong>gthat the other <strong>in</strong>haled corticosteroid preparations areunsafe dur<strong>in</strong>g pregnancy. Therefore, the use of any <strong>in</strong>haledcorticosteroids may be cont<strong>in</strong>ued <strong>in</strong> patients whose asthmawas well controlled by these agents before pregnancy (4).What is appropriate add-on controller therapyfor asthma dur<strong>in</strong>g pregnancy?Use of long-act<strong>in</strong>g β 2-agonists is the preferred add-oncontroller therapy for asthma dur<strong>in</strong>g pregnancy. Thistherapy should be added when patients’ symptoms areStep Therapy Medical Managementof <strong>Asthma</strong> Dur<strong>in</strong>g <strong>Pregnancy</strong>Mild Intermittent <strong>Asthma</strong>• <strong>No</strong> daily medications, albuterol as neededMild Persistent <strong>Asthma</strong>• Preferred—Low-dose <strong>in</strong>haled corticosteroid• Alternative—Cromolyn, leukotriene receptor antagonist,or theophyll<strong>in</strong>e (serum level 5–12 mcg/mL)Moderate Persistent <strong>Asthma</strong>• Preferred—Low-dose <strong>in</strong>haled corticosteroid andsalmeterol or medium-dose <strong>in</strong>haled corticosteroidor (if needed) medium-dose <strong>in</strong>haled corticosteroidand salmeterol• Alternative—Low-dose or (if needed) mediumdose<strong>in</strong>haled corticosteroid and either leukotrienereceptor antagonist or theophyll<strong>in</strong>e (serum level5–12 mcg/mL)Severe Persistent <strong>Asthma</strong>• Preferred—High-dose <strong>in</strong>haled corticosteroid andsalmeterol and (if needed) oral corticosteroid• Alternative—High-dose <strong>in</strong>haled corticosteroid andtheophyll<strong>in</strong>e (serum level 5–12 mcg/mL) and oralcorticosteroid if needednot controlled with the use of medium-dose <strong>in</strong>haled corticosteroids.Alternative add-on therapies are theophyll<strong>in</strong>eor leukotriene receptor antagonists (montelukast, zafirlukast).However, the use of long-act<strong>in</strong>g <strong>in</strong>haled β 2-agonistsis preferred because it has been shown to be a moreeffective add-on therapy <strong>in</strong> nonpregnant patients thanleukotriene receptor antagonists or theophyll<strong>in</strong>e. Longact<strong>in</strong>g<strong>in</strong>haled β 2-agonists have fewer side effects thantheophyll<strong>in</strong>e, which has a narrow therapeutic <strong>in</strong>dex andrequires serum monitor<strong>in</strong>g, and there are few data on theuse of leukotriene receptor antagonists <strong>in</strong> humans dur<strong>in</strong>gpregnancy. See Table 2 for typical medication dosages.Because long-act<strong>in</strong>g and short-act<strong>in</strong>g <strong>in</strong>haled β 2-agonistshave similar pharmacology and toxicology, long-act<strong>in</strong>g<strong>in</strong>haled β 2-agonists are expected to have a safety profilesimilar to that of albuterol. Two long-act<strong>in</strong>g <strong>in</strong>haledβ 2-agonists are available: 1) salmeterol and 2) formoterol.Limited observational data exist on their use dur<strong>in</strong>g pregnancy.A step-wise approach to management is advised <strong>in</strong>order to achieve control. See the box for specific therapy.For patients whose symptoms are not well controlled(Table 1) with the use of medium-dose <strong>in</strong>haled corticosteroidsand long-act<strong>in</strong>g <strong>in</strong>haled β 2-agonists, treatmentshould be advanced to high-dose <strong>in</strong>haled corticosteroids460 <strong>ACOG</strong> <strong>Practice</strong> <strong>Bullet<strong>in</strong></strong> <strong>Asthma</strong> <strong>in</strong> <strong>Pregnancy</strong> OBSTETRICS & GYNECOLOGY








