SCHOOL DISTRICT OF WAUKESHA SUMMER SCHOOL 2012
SCHOOL DISTRICT OF WAUKESHA SUMMER SCHOOL 2012
SCHOOL DISTRICT OF WAUKESHA SUMMER SCHOOL 2012
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
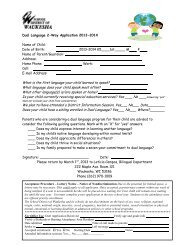
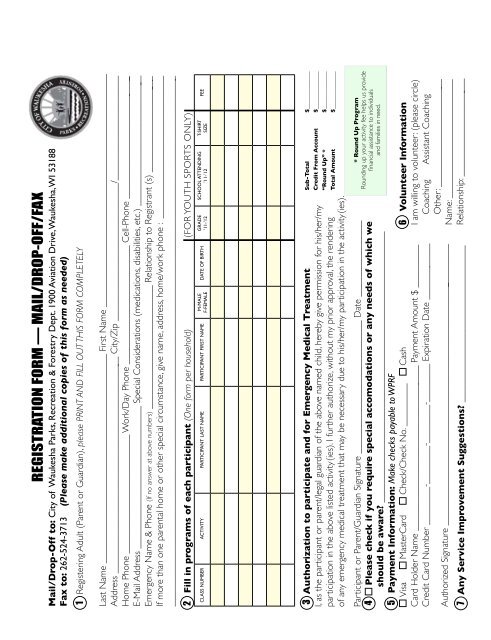
REGISTRATION FORM — MAIL/DROP-<strong>OF</strong>F/FAXMail/Drop-Off to: City of Waukesha Parks, Recreation & Forestry Dept. 1900 Aviation Drive, Waukesha, WI 53188Fax to: 262-524-3713 (Please make additional copies of this form as needed)1 Registering Adult (Parent or Guardian), please PRINT AND FILL OUT THIS FORM COMPLETELYLast Name ____________________________________________ First Name _________________________________________________Address ______________________________________________ City/Zip _____________________________/______________________Home Phone _________________________ Work/Day Phone _________________________ Cell-Phone __________________________E-Mail Address ______________________________ Special Considerations (medications, disabilities, etc.) _________________________ __Emergency Name & Phone (If no answer at above numbers) __________________________ Relationship to Registrant (s) _________________ ___If more than one parental home or other special circumstance, give name, address, home/work phone : ______________________________________________________________________________________________________________________________________________2 Fill in programs of each participant (One form per household) (FOR YOUTH SPORTS ONLY)CLASS NUMBER ACTIVITY PARTICIPANT LAST NAME PARTICIPANT FIRST NAMEM-MALEF-FEMALEDATE <strong>OF</strong> BIRTHGRADE’11-’12<strong>SCHOOL</strong> ATTENDING’11-’12T-SHIRTSIZEFEE3 Authorization to participate and for Emergency Medical TreatmentI, as the participant or parent/legal guardian of the above named child, hereby give permission for his/her/myparticipation in the above listed activity (ies). I further authorize, without my prior approval, the renderingof any emergency medical treatment that may be necessary due to his/her/my participation in the activity (ies).Participant or Parent/Guardian Signature ____________________________ Date ________________4 Please check if you require special accomodations or any needs of which weshould be aware? _________________________________________________________5 Payment Information: Make checks payable to WPRFVisa MasterCard Check/Check No. _________ CashCard Holder Name ___________________________________ Payment Amount $ _________Credit Card Number ________-________-________-________ Expiration Date ____________Authorized Signature ___________________________________________________________7 Any Service Improvement Suggestions? _________________________________Sub-Total $_____________Credit From Account $_____________“Round Up” * $_____________Total Amount $_____________* Round Up ProgramRounding up your activity fee helps us providefinancial assistance to individualsand families in need.6 Volunteer InformationI am willing to volunteer: (please circle)Coaching Assistant CoachingOther: _______________________Name: _________________________Relationship: _____________________