Health Form - Coppin State University
Health Form - Coppin State University
Health Form - Coppin State University
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
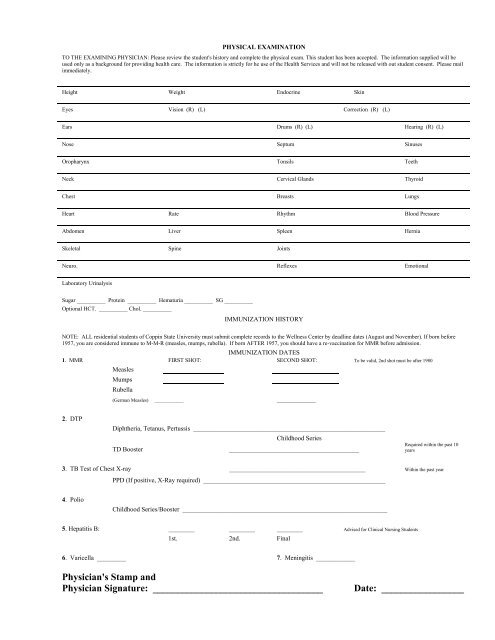
PHYSICAL EXAMINATIONTO THE EXAMINING PHYSICIAN: Please review the student's history and complete the physical exam. This student has been accepted. The information supplied will beused only as a background for providing health care. The information is strictly for he use of the <strong>Health</strong> Services and will not be released with out student consent. Please mailimmediately.Height Weight Endocrine SkinEyes Vision (R) (L) Correction (R) (L)Ears Drums (R) (L) Hearing (R) (L)Nose Septum SinusesOropharynx Tonsils TeethNeck Cervical Glands ThyroidChest Breasts LungsHeart Rate Rhythm Blood PressureAbdomen Liver Spleen HerniaSkeletal Spine JointsNeuro. Reflexes EmotionalLaboratory UrinalysisSugar __________ Protein __________ Hematuria __________ SG __________Optional HCT. __________ Chol. __________IMMUNIZATION HISTORYNOTE: ALL residential students of <strong>Coppin</strong> <strong>State</strong> <strong>University</strong> must submit complete records to the Wellness Center by deadline dates (August and November). If born before1957, you are considered immune to M-M-R (measles, mumps, rubella). If born AFTER 1957, you should have a re-vaccination for MMR before admission.IMMUNIZATION DATES1. MMR FIRST SHOT: SECOND SHOT: To be valid, 2nd shot must be after 1980MeaslesMumpsRubella(German Measles) ____________ ____________2. DTPDiphtheria, Tetanus, Pertussis ___________________________________________________________Childhood SeriesTD Booster________________________________________Required within the past 10years3. TB Test of Chest X-ray __________________________________________ Within the past yearPPD (If positive, X-Ray required) ________________________________________________________4. PolioChildhood Series/Booster _______________________________________________________________5. Hepatitis B: ________ ________ ________ Advised for Clinical Nursing Students1st. 2nd. Final6. Varicella _________ 7. Meningitis ____________Physician's Stamp andPhysician Signature: ___________________________________Date: _________________