14 Postpartum Hemorrhage on Labor and Delivery.pdf - Vtr
14 Postpartum Hemorrhage on Labor and Delivery.pdf - Vtr
14 Postpartum Hemorrhage on Labor and Delivery.pdf - Vtr

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<str<strong>on</strong>g>Postpartum</str<strong>on</strong>g> <str<strong>on</strong>g>Hemorrhage</str<strong>on</strong>g> <strong>on</strong> <strong>Labor</strong> <strong>and</strong> <strong>Delivery</strong><br />
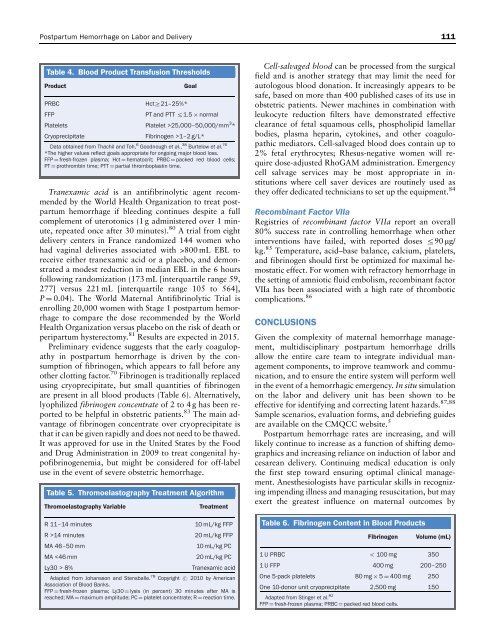
Table 4. Blood Product Transfusi<strong>on</strong> Thresholds<br />
Product Goal<br />
PRBC HctZ21–25%*<br />
FFP PT <strong>and</strong> PTT r1.5 normal<br />
Platelets Platelet >25,000–50,000/mm 3 *<br />
Cryoprecipitate Fibrinogen >1–2 g/L*<br />
Data obtained from Thachil <strong>and</strong> Toh, 6 Goodnough et al., 38 Burtelow et al. 76<br />
*The higher values reflect goals appropriate for <strong>on</strong>going major blood loss.<br />
FFP ¼ fresh-frozen plasma; Hct ¼ hematocrit; PRBC ¼ packed red blood cells;<br />
PT ¼ prothrombin time; PTT ¼ partial thromboplastin time.<br />
Tranexamic acid is an antifibrinolytic agent recommended<br />
by the World Health Organizati<strong>on</strong> to treat postpartum<br />
hemorrhage if bleeding c<strong>on</strong>tinues despite a full<br />
complement of uterot<strong>on</strong>ics (1 g administered over 1 minute,<br />
repeated <strong>on</strong>ce after 30 minutes). 80 A trial from eight<br />
delivery centers in France r<strong>and</strong>omized <str<strong>on</strong>g>14</str<strong>on</strong>g>4 women who<br />
had vaginal deliveries associated with >800 mL EBL to<br />
receive either tranexamic acid or a placebo, <strong>and</strong> dem<strong>on</strong>strated<br />
a modest reducti<strong>on</strong> in median EBL in the 6 hours<br />
following r<strong>and</strong>omizati<strong>on</strong> (173 mL [interquartile range 59,<br />
277] versus 221 mL [interquartile range 105 to 564],<br />
P ¼ 0.04). The World Maternal Antifibrinolytic Trial is<br />
enrolling 20,000 women with Stage 1 postpartum hemorrhage<br />
to compare the dose recommended by the World<br />
Health Organizati<strong>on</strong> versus placebo <strong>on</strong> the risk of death or<br />
peripartum hysterectomy. 81 Results are expected in 2015.<br />
Preliminary evidence suggests that the early coagulopathy<br />
in postpartum hemorrhage is driven by the c<strong>on</strong>sumpti<strong>on</strong><br />
of fibrinogen, which appears to fall before any<br />
other clotting factor. 70 Fibrinogen is traditi<strong>on</strong>ally replaced<br />
using cryoprecipitate, but small quantities of fibrinogen<br />
are present in all blood products (Table 6). Alternatively,<br />
lyophilized fibrinogen c<strong>on</strong>centrate of 2 to 4 g has been reported<br />
to be helpful in obstetric patients. 83 The main advantage<br />
of fibrinogen c<strong>on</strong>centrate over cryoprecipitate is<br />
that it can be given rapidly <strong>and</strong> does not need to be thawed.<br />
It was approved for use in the United States by the Food<br />
<strong>and</strong> Drug Administrati<strong>on</strong> in 2009 to treat c<strong>on</strong>genital hypofibrinogenemia,<br />
but might be c<strong>on</strong>sidered for off-label<br />
use in the event of severe obstetric hemorrhage.<br />
Table 5. Thromoelastography Treatment Algorithm<br />
Thromoelastography Variable Treatment<br />
R 11–<str<strong>on</strong>g>14</str<strong>on</strong>g> minutes 10 mL/kg FFP<br />
R ><str<strong>on</strong>g>14</str<strong>on</strong>g> minutes 20 mL/kg FFP<br />
MA 46–50 mm 10 mL/kg PC<br />
MA 8% Tranexamic acid<br />
Adapted from Johanss<strong>on</strong> <strong>and</strong> Stensballe. 78 Copyright r 2010 by American<br />
Associati<strong>on</strong> of Blood Banks.<br />
FFP ¼ fresh-frozen plasma; Ly30 ¼ lysis (in percent) 30 minutes after MA is<br />
reached; MA ¼ maximum amplitude; PC ¼ platelet c<strong>on</strong>centrate; R ¼ reacti<strong>on</strong> time.<br />
Cell-salvaged blood can be processed from the surgical<br />
field <strong>and</strong> is another strategy that may limit the need for<br />
autologous blood d<strong>on</strong>ati<strong>on</strong>. It increasingly appears to be<br />
safe, based <strong>on</strong> more than 400 published cases of its use in<br />
obstetric patients. Newer machines in combinati<strong>on</strong> with<br />
leukocyte reducti<strong>on</strong> filters have dem<strong>on</strong>strated effective<br />
clearance of fetal squamous cells, phospholipid lamellar<br />
bodies, plasma heparin, cytokines, <strong>and</strong> other coagulopathic<br />
mediators. Cell-salvaged blood does c<strong>on</strong>tain up to<br />
2% fetal erythrocytes; Rhesus-negative women will require<br />
dose-adjusted RhoGAM administrati<strong>on</strong>. Emergency<br />
cell salvage services may be most appropriate in instituti<strong>on</strong>s<br />
where cell saver devices are routinely used as<br />
they offer dedicated technicians to set up the equipment. 84<br />
Recombinant Factor VIIa<br />
Registries of recombinant factor VIIa report an overall<br />
80% success rate in c<strong>on</strong>trolling hemorrhage when other<br />
interventi<strong>on</strong>s have failed, with reported doses r90 mg/<br />
kg. 85 Temperature, acid–base balance, calcium, platelets,<br />
<strong>and</strong> fibrinogen should first be optimized for maximal hemostatic<br />
effect. For women with refractory hemorrhage in<br />
the setting of amniotic fluid embolism, recombinant factor<br />
VIIa has been associated with a high rate of thrombotic<br />
complicati<strong>on</strong>s. 86<br />
CONCLUSIONS<br />
Given the complexity of maternal hemorrhage management,<br />
multidisciplinary postpartum hemorrhage drills<br />
allow the entire care team to integrate individual management<br />
comp<strong>on</strong>ents, to improve teamwork <strong>and</strong> communicati<strong>on</strong>,<br />
<strong>and</strong> to ensure the entire system will perform well<br />
in the event of a hemorrhagic emergency. In situ simulati<strong>on</strong><br />
<strong>on</strong> the labor <strong>and</strong> delivery unit has been shown to be<br />
effective for identifying <strong>and</strong> correcting latent hazards. 87,88<br />
Sample scenarios, evaluati<strong>on</strong> forms, <strong>and</strong> debriefing guides<br />
are available <strong>on</strong> the CMQCC website. 5<br />
<str<strong>on</strong>g>Postpartum</str<strong>on</strong>g> hemorrhage rates are increasing, <strong>and</strong> will<br />
likely c<strong>on</strong>tinue to increase as a functi<strong>on</strong> of shifting demographics<br />
<strong>and</strong> increasing reliance <strong>on</strong> inducti<strong>on</strong> of labor <strong>and</strong><br />
cesarean delivery. C<strong>on</strong>tinuing medical educati<strong>on</strong> is <strong>on</strong>ly<br />
the first step toward ensuring optimal clinical management.<br />
Anesthesiologists have particular skills in recognizing<br />
impending illness <strong>and</strong> managing resuscitati<strong>on</strong>, but may<br />
exert the greatest influence <strong>on</strong> maternal outcomes by<br />
Table 6. Fibrinogen C<strong>on</strong>tent in Blood Products<br />
Fibrinogen Volume (mL)<br />
1 U PRBC o 100 mg 350<br />
1 U FFP 400 mg 200–250<br />
One 5-pack platelets 80 mg 5 ¼ 400 mg 250<br />
One 10-d<strong>on</strong>or unit cryoprecipitate<br />
Adapted from Stinger et al.<br />
2,500 mg 150<br />
82<br />
FFP ¼ fresh-frozen plasma; PRBC ¼ packed red blood cells.<br />
111