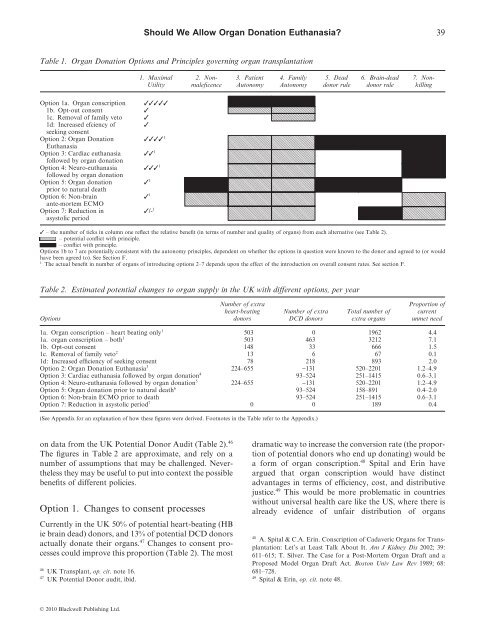
Should We Allow Organ Donation Euthanasia? 39Table 1. Organ Donation Options and Principles governing <strong>organ</strong> transplantation1. MaximalUtility2. Nonmaleficence3. PatientAutonomy4. FamilyAutonomy5. Deaddonor rule6. Brain-deaddonor rule7. NonkillingOption 1a. Organ conscription1b. Opt-out consent1c. Removal of family veto1d: Increased efÞciency ofseeking consentOption 2: Organ DonationEuthanasiaOption 3: Cardiac <strong>euthanasia</strong>follo<strong>we</strong>d by <strong>organ</strong> <strong>donation</strong>Option 4: Neuro-<strong>euthanasia</strong>follo<strong>we</strong>d by <strong>organ</strong> <strong>donation</strong>Option 5: Organ <strong>donation</strong>prior to natural deathOption 6: Non-brainante-mortem ECMOOption 7: Reduction inasystolic period11111/- 1– the number of ticks in column one reflect the relative benefit (in terms of number and quality of <strong>organ</strong>s) from each alternative (see Table 2).– potential conflict with principle.– conflict with principle.Options 1b to 7 are potentially consistent with the autonomy principles, dependent on whether the options in question <strong>we</strong>re known to the donor and agreed to (or wouldhave been agreed to). See Section F.1 The actual benefit in number of <strong>organ</strong>s of introducing options 2–7 depends upon the effect of the introduction on overall consent rates. See section F.Table 2. Estimated potential changes to <strong>organ</strong> supply in the UK with different options, per yearOptionsNumber of extraheart-beatingdonorsNumber of extraDCD donorsTotal number ofextra <strong>organ</strong>sProportion ofcurrentunmet need1a. Organ conscription – heart beating only 1 503 0 1962 4.41a. <strong>organ</strong> conscription – both 1 503 463 3212 7.11b. Opt-out consent 148 33 666 1.51c. Removal of family veto 2 13 6 67 0.11d: Increased efficiency of seeking consent 78 218 893 2.0Option 2: Organ Donation Euthanasia 3 224–655 -131 520–2201 1.2–4.9Option 3: Cardiac <strong>euthanasia</strong> follo<strong>we</strong>d by <strong>organ</strong> <strong>donation</strong> 4 93–524 251–1415 0.6–3.1Option 4: Neuro-<strong>euthanasia</strong> follo<strong>we</strong>d by <strong>organ</strong> <strong>donation</strong> 5 224–655 -131 520–2201 1.2–4.9Option 5: Organ <strong>donation</strong> prior to natural death 6 93–524 158–891 0.4–2.0Option 6: Non-brain ECMO prior to death 93–524 251–1415 0.6–3.1Option 7: Reduction in asystolic period 7 0 0 189 0.4(See Appendix for an explanation of how these figures <strong>we</strong>re derived. Footnotes in the Table refer to the Appendix.)on data from the UK Potential Donor Audit (Table 2). 46The figures in Table 2 are approximate, and rely on anumber of assumptions that may be challenged. Neverthelessthey may be useful to put into context the possiblebenefits of different policies.Option 1. Changes to consent processesCurrently in the UK 50% of potential heart-beating (HBie brain dead) donors, and 13% of potential DCD donorsactually donate their <strong>organ</strong>s. 47 Changes to consent processescould improve this proportion (Table 2). The most46 UK Transplant, op. cit. note 16.47UK Potential Donor audit, ibid.dramatic way to increase the conversion rate (the proportionof potential donors who end up donating) would bea form of <strong>organ</strong> conscription. 48 Spital and Erin haveargued that <strong>organ</strong> conscription would have distinctadvantages in terms of efficiency, cost, and distributivejustice. 49 This would be more problematic in countrieswithout universal health care like the US, where there isalready evidence of unfair distribution of <strong>organ</strong>s48A. Spital & C.A. Erin. Conscription of Cadaveric Organs for Transplantation:Let’s at Least Talk About It. Am J Kidney Dis 2002; 39:611–615; T. Silver. The Case for a Post-Mortem Organ Draft and aProposed Model Organ Draft Act. Boston Univ Law Rev 1989; 68:681–728.49Spital & Erin, op. cit. note 48.© 2010 Black<strong>we</strong>ll Publishing Ltd.
40 Dominic Wilkinson and Julian Savulescu50A.A. Herring, S. Woolhandler & D.U. Himmelstein. InsuranceStatus of US Organ Donors and Transplant Recipients: The UninsuredGive but Rarely Receive. Int J Health Serv 2008; 38: 641–652.51 It is arguable whether dead people can be used as a mere means in thesame way as <strong>we</strong> use live people as a mere means. They are dead, have noongoing interests and are incapable of consenting.52B. Pierscionek. What Is Presumed When We Presume Consent?BMC Med Ethics 2008; 9: 8.53Quigley et al., op. cit. note 11.54 The UK <strong>organ</strong> <strong>donation</strong> taskforce rejected evidence of possibleincreases in donor numbers and recently released a report advisingagainst the adoption of opt-out consent in the UK. Organ DonationTaskforce. 2007. The potential impact of an opt out system for <strong>organ</strong><strong>donation</strong> in the UK: an independent report from the Organ DonationTaskforce. London, UK. Available at: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_090312 [Accessed 07 Jan 2009].55 We are grateful to an anonymous revie<strong>we</strong>r for encouraging us toinvestigate this alternative. Combinations of these measures are possible.For example an opt-out <strong>organ</strong> <strong>donation</strong> consent system could beintroduced without permitting family members to veto <strong>donation</strong>. This issometimes referred to as a ‘hard opt-out’ form of <strong>organ</strong> <strong>donation</strong>(ibid:12). It is not possible from UK figures to estimate what effect thiswould have on overall <strong>organ</strong> supply.according to insurance status. 50 Organ conscriptionmight be applied to individuals who are brain dead, orcould be applied also to patients who have died followingwithdrawal of LST. Thus it has the potential to increasethe number of <strong>organ</strong>s for transplantation in the UK byup to 3212 per year. It would violate the principles ofPatient and Family Autonomy (Principles 3 and 4), andcould be criticized for using patients as a mere means. 51Smaller increments in <strong>organ</strong> <strong>donation</strong> could beachieved in the UK by moving to an opt-out consentsystem for <strong>organ</strong> <strong>donation</strong>. Some have concerns aboutwhether this would violate the wishes of patients. 52Ho<strong>we</strong>ver, since this sort of system would <strong>allow</strong> patientswho have a strong preference not to donate to opt-out of<strong>organ</strong> <strong>donation</strong>, it would appear to respect PatientAutonomy. Most countries that have adopted a form ofopt-out consent (including Spain, with the highest <strong>donation</strong>rates per capita) permit family members to veto<strong>organ</strong> <strong>donation</strong>, even where the patient has not opted outduring life. 53 So Family Autonomy would also berespected. A change to an opt-out consent system in theUK would potentially increase the number of transplantable<strong>organ</strong>s by 666 per year. 54In a small number of cases families decline <strong>organ</strong> <strong>donation</strong>even though the patient had indicated during life thatthey would like to donate by joining the <strong>organ</strong> donorregister. If families <strong>we</strong>re unable to veto <strong>organ</strong> <strong>donation</strong> insuch cases this would potentially make available 67 additional<strong>organ</strong>s per year in the UK (Table 2). 55 This wouldconflict with the Principle of Family Autonomy.Alternatively, there may be ways to improve the efficiencyof <strong>organ</strong> <strong>donation</strong> without changing the nature ofconsent decisions. Much of the success of the ‘Spanishmodel’ of <strong>organ</strong> <strong>donation</strong> may be attributed to the processesand systems that support <strong>organ</strong> <strong>donation</strong> andcounsel families. 56 For example, in the UK potentialdonor audit there <strong>we</strong>re 141 patients who <strong>we</strong>re diagnosedas brain dead in whom <strong>organ</strong> <strong>donation</strong> was not considered,or whose families <strong>we</strong>re never approached. 57 If allpotential HB or DCD donor families <strong>we</strong>re approachedfor consent (and the consent rates <strong>we</strong>re the same as theyare at present), 893 additional <strong>organ</strong>s per year could bemade available. This would not violate any of the listedethical principles governing <strong>organ</strong> transplantation, butwould require significant resources to be made availablefor counselling and support. This would potentiallybe sufficient to resolve the current shortfall in <strong>organ</strong>supply. 58Option 2. Organ Donation EuthanasiaSome have argued that <strong>we</strong> <strong>should</strong> reject the ‘dead donorrule’ (Principle 5). 59 This has mainly been embraced toconsider patients who are permanently unconscious, forexample those in a permanent vegetative state, or anencephalicinfants. 60 According to some views, their <strong>organ</strong>scan be removed because they have no prospect of regainingconsciousness and continued life cannot benefitthem. 61 In James Rachel’s terms, while their biological lifemay continue, their biographical life has ended. 62 Theycannot be harmed by removal of their <strong>organ</strong>s. 63 Ho<strong>we</strong>ver,such a proposal could be more widely cast to includeLSW donors.It is permissible to withdraw life support from a patientwith extremely poor prognosis, in the knowledge that thiswill certainly lead to their death, even if it would bepossible to keep them alive for some time. It is permissibleto remove their <strong>organ</strong>s after they have died. But why56 Quigley et al., op. cit. note 11.57UK Transplant audit, op. cit. note 16.58 This depends whether the <strong>organ</strong>s made available <strong>we</strong>re of the rightsort and tissue type to meet the needs of those currently dying whilewaiting for a transplant. It may not be enough to provide <strong>organ</strong>s forthose patients who at present are arbitrarily excluded from waiting lists(see note 8).59Truog & Robinson, op. cit. note 39; C. Coons & N. Levin. The DeadDonor Rule, Voluntary Active Euthanasia and Capital Punishment.Bioethics 2009. Published online 26 Oct 2009. DOI: 10.1111/j.1467-8519.2009.01767.x60Veatch, op. cit. note 15.61P. Singer. 1994. Rethinking Life and Death. Melbourne: The TextPublishing Company: 207. In two surveys in the US, a majority ofrespondents supported <strong>donation</strong> of <strong>organ</strong>s from patients in permanentcoma or vegetative state. J.M. DuBois & T. Schmidt. Does the PublicSupport Organ Donation Using Higher Brain-Death Criteria? J ClinEthics 2003; 14: 26–36; L.A. Siminoff, C. Burant & S.J. Youngner.Death and Organ Procurement: Public Beliefs and Attitudes. Soc SciMed 2004; 59: 2325–2334.62 J. Rachels. 1986. The End of Life : Euthanasia and Morality. Oxford:Oxford University Press: 24–25.63Truog & Robinson, op. cit. note 39.© 2010 Black<strong>we</strong>ll Publishing Ltd.