pink28in Brisbane, basing his clinical description on the records of some 51 cases in hispractice in the preceding 6 years or so (Wood 1920). In 1935 A J Wood and his son,Ian, in a report to the annual meeting of the British Medical Association inMelbourne, indicated that their series totalled 150, of which 60 had been addedbetween 1920-1935 (Wood & Wood, 1935).The next major contribution to the Australian literature on this disease was madeby Southby in 1949, when he was able to draw upon the records of 502 childrendiagnosed as having had this condition. This total was made up partly from hisexperiences in his private and hospital practices, and partly from the practices ofsome of his colleagues (Southby, 1949).This brief revue of the source material for the major Australian contributionsuggests either a wider recognition or a mounting incidence from the 1st recognitionthrough to the late 1940’s. This would seem to parallel events in England & Wales.Logan (1949) has shown that the death rates from pink disease of children agedunder 5 years rapidly mounted from 0.3 per million in 1923 to a peak of 31.4 permillion in 1936. For a few years the numbers fluctuated and they dropped to a lowerplateau, which continued at around 17.0 per million until 1946.In 1947 there was a sharp rise to 29.0 per million. Logan suggested that thewidening recognition of the disease was probably responsible for the steady rise indeath rates to the plateau which commenced in the early 1940’s. Since 1948 there hasbeen a sharp decline to almost disappearance. This will be discussed later.Control of a disease is dependent upon the definition of the aetiology. For manyyears the aetiology of pink disease has been the subject of much speculation and someexperimentation. Earlier theories covered a wide range of possibilities, including anallergic response, endocrine dysfunction, poisoning by arsenic and ergot, an infectiveagent. Some of these, like the arsenic and ergot theories, were disposed of; but thedifficulties of testing other hypotheses left some of them still possibilities whenFranconi and his co-workers (1947) suggested that mercury poisoning and/orsensitivity was the main or perhaps the only aetiological factor.This hypotheses, which was supported by the work of Warkany and Hubbard, ayear or so later, offered for the first time a possible tangible objective for the controlof pink disease-namely, the removal of mercury from teething powders and syrups,the commonest source for infants and young children, and perhaps the restricted useof mercurial ointments on young children.Action to this end occurred in England before it did in Australia. Colver (1956)points out that the warnings by prominent paediatricians and public-health workersin the early 1950’s (Gaisford, 1949; James, 1951) considerably REDUCED thenumber of prescriptions written by doctors, and ultimately led to the withdrawal bya principal manufacturer of mercury from teething powders.This was effective in December 1953, although some small manufacturers andpharmacists still appeared to be including the metal in locally dispensed powders(Dathan and Macaulay, 1955). It has apparently not been thought necessary tointroduce legislation in England to control the use of mercury in teething powders.Colver (1956) has shown that between 1947-1955 there was a reduction of about 75%in the number of patients with pink disease treated at the Sheffield Children’shttp://www.users.bigpond.com/difarnsworth/pink28.htm (3 of 9) [05/28/2000 1:43:00 AM]
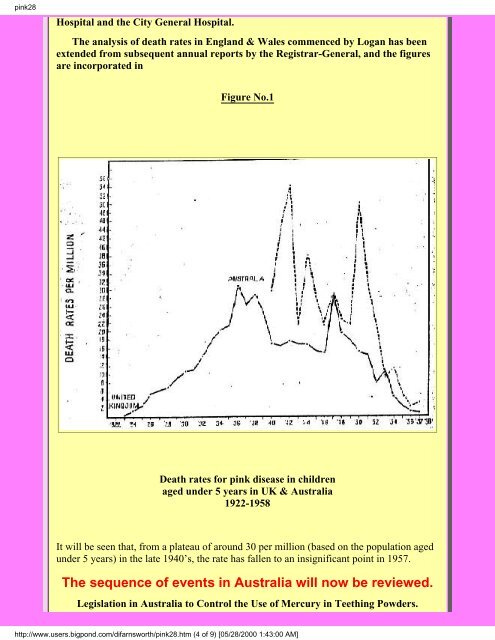
pink28Hospital and the City General Hospital.The analysis of death rates in England & Wales commenced by Logan has beenextended from subsequent annual reports by the Registrar-General, and the figuresare incorporated inFigure No.1Death rates for pink disease in childrenaged under 5 years in UK & Australia1922-1958It will be seen that, from a plateau of around 30 per million (based on the population agedunder 5 years) in the late 1940’s, the rate has fallen to an insignificant point in 1957.The sequence of events in Australia will now be reviewed.Legislation in Australia to Control the Use of Mercury in Teething Powders.http://www.users.bigpond.com/difarnsworth/pink28.htm (4 of 9) [05/28/2000 1:43:00 AM]
- Page 2 and 3: pink2aACRODYNIA-Nelson's book of po
- Page 4 and 5: pink34Acrodynia (the term derived f
- Page 6 and 7: pink3430mg/kg daily in 2-3 divided
- Page 8 and 9: pink disease, acrodynia, mercury po
- Page 10 and 11: pink disease, acrodynia, mercury po
- Page 12 and 13: pink disease, acrodynia, mercury po
- Page 14 and 15: pink disease, acrodynia, mercury po
- Page 16 and 17: pink28THE MEDICAL JOURNAL OF AUSTRA
- Page 20 and 21: pink28On August 20, 1953, The South
- Page 22 and 23: pink28Some interesting facts emerge
- Page 24 and 25: pink28nurses and others. Unfortunat
- Page 26 and 27: pink disease, acrodynia, mercury po
- Page 28 and 29: pink disease, acrodynia, mercury po
- Page 30 and 31: pink disease, acrodynia, mercury po
- Page 32 and 33: pink disease, acrodynia, mercury po
- Page 34 and 35: pink disease, acrodynia, mercury po
- Page 36 and 37: pink disease, acrodynia, mercury po
- Page 38 and 39: pcheek41ACRODYNIA by DONALD B. CHEE
- Page 40 and 41: pcheek41GO to NEXT ARTICLERETURN to
- Page 42 and 43: pink disease, acrodynia, mercury po
- Page 44 and 45: pink disease, acrodynia, mercury po
- Page 46 and 47: pink disease, acrodynia, mercury po
- Page 48 and 49: pink55,pink disease, acrodynia, mer
- Page 50 and 51: pink55,pink disease, acrodynia, mer
- Page 52 and 53: pink55,pink disease, acrodynia, mer
- Page 54 and 55: pink55,pink disease, acrodynia, mer
- Page 56 and 57: pink disease, acrodynia, mercury po
- Page 58 and 59: pink disease, acrodynia, mercury po
- Page 60 and 61: pink disease, acrodynia, mercury po
- Page 62 and 63: pink disease, acrodynia, mercury po