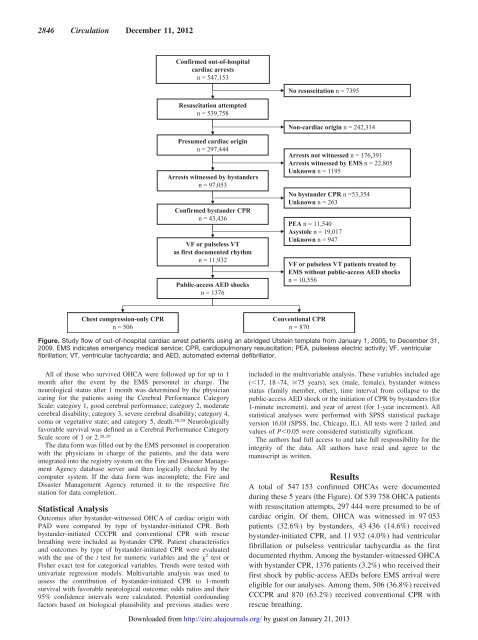
2846 <strong>Circulation</strong> December 11, 2012Figure. <strong>Study</strong> flow of out-of-hospital cardiac arrest patients using an abridged Utstein template from January 1, 2005, to December 31,2009. EMS indicates emergency medical service; CPR, cardiopulmonary resuscitation; PEA, pulseless electric activity; VF, ventricularfibrillation; VT, ventricular tachycardia; and AED, automated external defibrillator.All of those who survived OHCA were followed up <strong>for</strong> up to 1month after <strong>the</strong> event by <strong>the</strong> EMS personnel in charge. Theneurological status after 1 month was determined by <strong>the</strong> physiciancaring <strong>for</strong> <strong>the</strong> patients using <strong>the</strong> Cerebral Per<strong>for</strong>mance CategoryScale: category 1, good cerebral per<strong>for</strong>mance; category 2, moderatecerebral disability; category 3, severe cerebral disability; category 4,coma or vegetative state; and category 5, death. 28,29 Neurologicallyfavorable survival was defined as a Cerebral Per<strong>for</strong>mance CategoryScale score of 1 or 2. 28,29The data <strong>for</strong>m was filled out by <strong>the</strong> EMS personnel in cooperationwith <strong>the</strong> physicians in charge of <strong>the</strong> patients, and <strong>the</strong> data wereintegrated into <strong>the</strong> registry system on <strong>the</strong> Fire and Disaster ManagementAgency database server and <strong>the</strong>n logically checked by <strong>the</strong>computer system. If <strong>the</strong> data <strong>for</strong>m was incomplete, <strong>the</strong> Fire andDisaster Management Agency returned it to <strong>the</strong> respective firestation <strong>for</strong> data completion.Statistical AnalysisOutcomes after bystander-witnessed OHCA of cardiac origin withPAD were compared by type of bystander-initiated CPR. Bothbystander-initiated CCCPR and conventional CPR with rescuebreathing were included as bystander CPR. Patient characteristicsand outcomes by type of bystander-initiated CPR were evaluatedwith <strong>the</strong> use of <strong>the</strong> t test <strong>for</strong> numeric variables and <strong>the</strong> 2 test orFisher exact test <strong>for</strong> categorical variables. Trends were tested withunivariate regression models. Multivariable analysis was used toassess <strong>the</strong> contribution of bystander-initiated CPR to 1-monthsurvival with favorable neurological outcome; odds ratios and <strong>the</strong>ir95% confidence intervals were calculated. Potential confoundingfactors based on biological plausibility and previous studies wereincluded in <strong>the</strong> multivariable analysis. These variables included age(17, 18–74, 75 years), sex (male, female), bystander witnessstatus (family member, o<strong>the</strong>r), time interval from collapse to <strong>the</strong>public-access AED shock or <strong>the</strong> initiation of CPR by bystanders (<strong>for</strong>1-minute increment), and year of arrest (<strong>for</strong> 1-year increment). Allstatistical analyses were per<strong>for</strong>med with SPSS statistical packageversion 16.0J (SPSS, Inc, Chicago, IL). All tests were 2 tailed, andvalues of P0.05 were considered statistically significant.The authors had full access to and take full responsibility <strong>for</strong> <strong>the</strong>integrity of <strong>the</strong> data. All authors have read and agree to <strong>the</strong>manuscript as written.ResultsA total of 547 153 confirmed OHCAs were documentedduring <strong>the</strong>se 5 years (<strong>the</strong> Figure). Of 539 758 OHCA patientswith resuscitation attempts, 297 444 were presumed to be ofcardiac origin. Of <strong>the</strong>m, OHCA was witnessed in 97 053patients (32.6%) by bystanders, 43 436 (14.6%) receivedbystander-initiated CPR, and 11 932 (4.0%) had ventricularfibrillation or pulseless ventricular tachycardia as <strong>the</strong> firstdocumented rhythm. Among <strong>the</strong> bystander-witnessed OHCAwith bystander CPR, 1376 patients (3.2%) who received <strong>the</strong>irfirst shock by public-access AEDs be<strong>for</strong>e EMS arrival wereeligible <strong>for</strong> our analyses. Among <strong>the</strong>m, 506 (36.8%) receivedCCCPR and 870 (63.2%) received conventional CPR withrescue breathing.Downloaded from http://circ.ahajournals.org/ by guest on January 21, 2013
Iwami et al Compression-Only CPR <strong>for</strong> OHCA With PAD 2847Table 1. Characteristics of Out-of-Hospital Cardiac Arrest PatientsWith Public-Access Automated External Defibrillation Shocks by Typeof Bystander-Initiated Cardiopulmonary <strong>Resuscitation</strong>Compression-OnlyCPR (n506)ConventionalCPR (n870)PAge, mean (SD), y 61.3 (16.2) 61.3 (19.1) 0.986Age group, n (%) 0.00317 y 8 (1.6) 36 (4.1)18–74 y 397 (78.5) 621 (71.4)75 y 101 (20.0) 213 (24.5)Sex, n (%) 0.001Male 430 (85.0) 659 (75.7)Female 76 (15.0) 211 (24.3)Type of bystanderwitness status, n (%)0.389Family member 50 (9.9) 99 (11.4)O<strong>the</strong>r 456 (90.1) 771 (88.6)Collapse to public-access 2.9 (4.8) 2.6 (5.1) 0.256AED shock or initiation of CPRby bystanders, mean (SD), minCPR indicates cardiopulmonary resuscitation; AED, automated externaldefibrillator.Characteristics of OHCA patients with PAD by type ofbystander CPR are noted in Table 1. Mean age and bystanderwitness status were similar between <strong>the</strong> groups. The proportionsof children (17 years) and elderly (75 years) werelower in <strong>the</strong> CCCPR group than in <strong>the</strong> conventional CPRgroup, and <strong>the</strong> male/female ratio was higher in <strong>the</strong> CCCPRgroup than in <strong>the</strong> conventional CPR group. Mean timeintervals from collapse to <strong>the</strong> public-access AED shock or <strong>the</strong>initiation of CPR by bystanders were also similar. Theproportion of patients receiving CCCPR among eligiblepatients significantly increased from 5.1% (2 of 37) in 2005to 44.4% (246 of 554) in 2009 (P <strong>for</strong> trend 0.001; Table 2).Table 3 shows <strong>the</strong> outcomes of OHCA patients with PADby type of bystander-initiated CPR. The CCCPR group hadsignificantly better outcomes after OHCA than <strong>the</strong> conventionalCPR group (prehospital return of spontaneous circulation,50.2% [254 of 506] versus 40.5% [352 of 506],P0.001; 1-month survival, 46.4% [235 of 506] versus39.9% [347 of 870], P0.018; neurologically favorable1-month survival, 40.7% [206 of 506] versus 32.9% [286 of870], P0.003, respectively).Table 4 shows <strong>the</strong> factors associated with neurologicallyfavorable 1-month survival after OHCA with PAD.Table 3. Outcomes of Out-of-Hospital Cardiac Arrest PatientsWith Public-Access Automated External Defibrillation Shocksby Type of Bystander-Initiated Cardiopulmonary <strong>Resuscitation</strong>Compression-OnlyCPR (n506)ConventionalCPR (n870)PPrehospital ROSC, n (%) 254 (50.2) 352 (40.5) 0.0011-mo survival, n (%) 235 (46.4) 347 (39.9) 0.018Neurologically favorable 1-mosurvival, n (%)206 (40.7) 286 (32.9) 0.003CPR indicates cardiopulmonary resuscitation; ROSC, return of spontaneouscirculation.Bystander-initiated CCCPR produced more neurologicallyfavorable 1-month survival than conventional CPR (adjustedodds ratio, 1.33; 95% confidence interval, 1.03–1.70). Comparedwith <strong>the</strong> elderly, adults 18 to 74 years of age (adjustedodds ratio, 4.76; 95% confidence interval, 3.27–6.92) andchildren (adjusted odds ratio, 9.46; 95% confidence interval,4.69–19.08) had significantly higher rates of neurologicallyfavorable 1-month survival after OHCA. Earlier shocks(adjusted odds ratio <strong>for</strong> 1-minute increment, 0.93; 95%confidence interval, 0.89–0.96) were also associated withfavorable neurological outcome.DiscussionFrom this nationwide registry of OHCA, we demonstratedthat CCCPR was more effective than conventional CPR withrescue breathing <strong>for</strong> individuals with witnessed OHCA whoare shocked with public-access AEDs. This is <strong>the</strong> first studyto investigate <strong>the</strong> effectiveness of CCCPR compared withconventional CPR in <strong>the</strong> present era when <strong>the</strong>re is anincreasing chance of receiving shocks with public-accessAEDs. Such a large, prospective, population-based studycovering all of Japan, at a time when <strong>the</strong> PAD program hasdeveloped nearly worldwide, makes it possible to evaluate <strong>the</strong>effectiveness of each type of bystander CPR <strong>for</strong> those treatedwith PAD.The present study suggests that <strong>the</strong> combination of earlydefibrillation with public-access AEDs and CCCPR by bystandersis <strong>the</strong> best way to save lives after sudden cardiacarrests. Neurologically favorable survival after witnessedventricular fibrillation was 40% among those who receivedCCCPR and defibrillation with public-access AEDs. This isone of <strong>the</strong> highest survival rates with neurologically favorableoutcome reported 20 and should be <strong>the</strong> target survival afterOHCA. Many reports have shown <strong>the</strong> extreme effectivenessof early defibrillation with public-access AEDs, 20–22 whichTable 2. Proportion of Type of Bystander-Initiated Cardiopulmonary <strong>Resuscitation</strong> AmongOut-of-Hospital Cardiac Arrest Patients With Public-Access Automated External DefibrillationShocks by Year2005(n39)2006(n125)2007(n262)2008(n396)2009(n554)P <strong>for</strong>TrendConventional CPR with 37 (94.9) 101 (80.8) 175 (66.8) 249 (62.9) 308 (55.6) 0.001rescue breathing, n (%)Chest compression–only 2 (5.1) 24 (19.2) 87 (33.2) 147 (37.1) 246 (44.4)CPR, n (%)CPR indicates cardiopulmonary resuscitation.Downloaded from http://circ.ahajournals.org/ by guest on January 21, 2013