Recognising the fact that improvements in health status in <strong>In</strong>dia were not commensurate with growing incomelevels, the Government launched the NRHM in 2005 to address infirmities and problems across PHC andbring about improvement in the health system and the health status of those who live in rural areas. TheMission aims to provide universal access to equitable, affordable, and quality health care that is accountableand at the same time responsive to the needs of people. Largely through the NRHM, the Government will seekto increase its financing of the health sector from 1% to 2% of the GDP over time.The Goals of the NRHM are:• Reduction in IMR, MMR and TFR;• Universal access to public health services such as women’s health;• Child health, water, sanitation and hygiene, immunisation, andnutrition;• Prevention and control of communicable and non-communicablediseases, including locally endemic diseases;• Access to integrated comprehensive PHC;• Population stabilisation, gender and demographic balance;• Revitalise local health traditions and mainstream AYUSH; and• Promotion of healthy lifestyle.Thus, RH is an integral part of the NRHM.Thus, there are manychallenges that remain to bemet. For effectiveimplementation, creatingshared vision and ownership ofthe NRHM and its urgencyneeds to be generated at alllevels. However, ifimplemented well, the NRHMis likely to make significantdifference in the health ofpeople, particularly of mothersand children.The strategies to achieve the above goals include the following:• Strengthen infrastructure. Strengthen (i) Sub-centre through untied funds, (ii) Primary Health Centresand Community Health Centres (Block Level Hospitals) to bring them to <strong>In</strong>dian Public Health Standards,and (iii) mobile medical teams;• Communitise. One Accredited Social Health Activist (ASHA) in every village, Village Health and SanitationCommittee, and strengthen capacity of local government institutions;• Improve administration. <strong><strong>In</strong>ter</strong>-sectoral planning at village and district levels, integrate vertical diseasecontrol programmes, transparent policies for deployment and career development of human resources forhealth, and strengthen capacities for preventive and promotive health care; and• PPP. <strong>In</strong>creased PPP in the delivery of health services.Along with the NRHM, the Janani Suraksha Yojana (JSY), scheme to protect mothers, was launched in 2005.It includes a Conditional Cash Transfer Mechanism and a demand-side intervention for all deliveries in 18focus states and for people living below the poverty line in other states. The financial package of Rs 2,000(about US$ 41, at current exchange rate of US$ 1 - Rs 49) includes the following services:• Early registration of pregnancy (within first trimester);• Delivery care through micro-birth plan;• Referral transport (Home to Health <strong>In</strong>stitution) and incentive;• <strong>In</strong>stitutional births;• Post-delivery visit and reporting; and• FP and counselling.Figure 1 shows an illustrative government health service delivery structure under the NRHM.A review of the NRHM implementation shows that there is a huge backlog of infrastructure in some states.There is also a serious shortage of medical specialists which hampers effective functioning of these institutions.On the other hand, a large number of ASHAs have been recruited and are being trained, but much more effortwould be required for them to effectively perform their roles.27
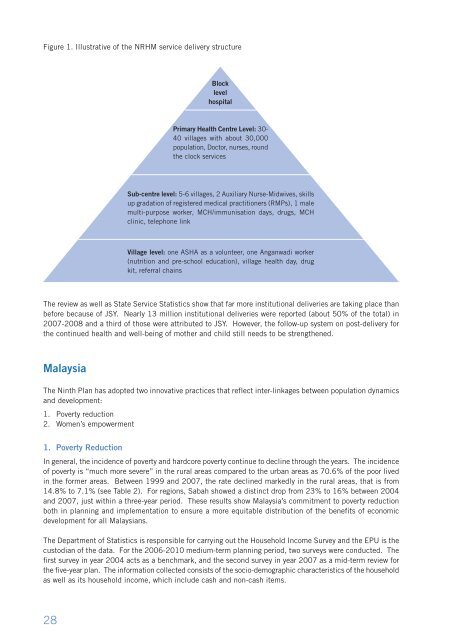
Figure 1. Illustrative of the NRHM service delivery structureBlocklevelhospitalPrimary Health Centre Level: 30-40 villages with about 30,000population, Doctor, nurses, roundthe clock servicesSub-centre level: 5-6 villages, 2 Auxiliary Nurse-Midwives, skillsup gradation of registered medical practitioners (RMPs), 1 malemulti-purpose worker, MCH/immunisation days, drugs, MCHclinic, telephone linkVillage level: one ASHA as a volunteer, one Anganwadi worker(nutrition and pre-school education), village health day, drugkit, referral chainsThe review as well as State Service Statistics show that far more institutional deliveries are taking place thanbefore because of JSY. Nearly 13 million institutional deliveries were reported (about 50% of the total) in2007-2008 and a third of those were attributed to JSY. However, the follow-up system on post-delivery forthe continued health and well-being of mother and child still needs to be strengthened.MalaysiaThe Ninth Plan has adopted two innovative practices that reflect inter-linkages <strong>between</strong> population dynamicsand development:1. Poverty reduction2. Women’s empowerment1. Poverty Reduction<strong>In</strong> general, the incidence of poverty and hardcore poverty continue to decline through the years. The incidenceof poverty is “much more severe” in the rural areas compared to the urban areas as 70.6% of the poor livedin the former areas. Between 1999 and 2007, the rate declined markedly in the rural areas, that is from14.8% to 7.1% (see Table 2). For regions, Sabah showed a distinct drop from 23% to 16% <strong>between</strong> 2004and 2007, just within a three-year period. These results show Malaysia’s commitment to poverty reductionboth in planning and implementation to ensure a more equitable distribution of the benefits of economicdevelopment for all Malaysians.The Department of Statistics is responsible for carrying out the Household <strong>In</strong>come Survey and the EPU is thecustodian of the data. For the 2006-2010 medium-term planning period, two surveys were conducted. Thefirst survey in year 2004 acts as a benchmark, and the second survey in year 2007 as a mid-term review forthe five-year plan. The information collected consists of the socio-demographic characteristics of the householdas well as its household income, which include cash and non-cash items.28