Second Opinion
Download - Research To Practice
Download - Research To Practice
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
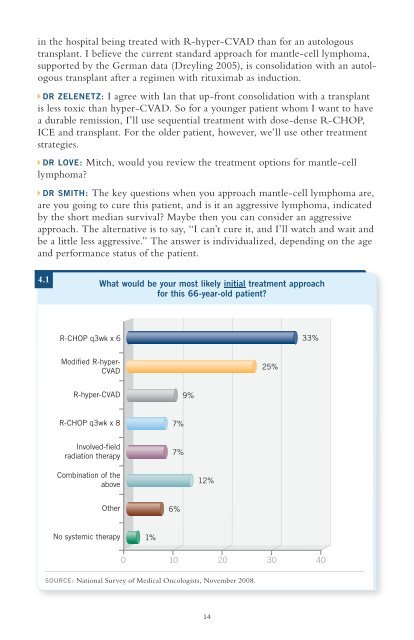
in the hospital being treated with R-hyper-CVAD than for an autologoustransplant. I believe the current standard approach for mantle-cell lymphoma,supported by the German data (Dreyling 2005), is consolidation with an autologoustransplant after a regimen with rituximab as induction.DR ZELENETZ: I agree with Ian that up-front consolidation with a transplantis less toxic than hyper-CVAD. So for a younger patient whom I want to havea durable remission, I’ll use sequential treatment with dose-dense R-CHOP,ICE and transplant. For the older patient, however, we’ll use other treatmentstrategies.DR LOVE: Mitch, would you review the treatment options for mantle-celllymphoma?DR SMITH: The key questions when you approach mantle-cell lymphoma are,are you going to cure this patient, and is it an aggressive lymphoma, indicatedby the short median survival? Maybe then you can consider an aggressiveapproach. The alternative is to say, “I can’t cure it, and I’ll watch and wait andbe a little less aggressive.” The answer is individualized, depending on the ageand performance status of the patient.4.1What would be your most likely initial treatment approachfor this 66-year-old patient?R-CHOP q3wk x 633%Modified R-hyper-CVAD25%R-hyper-CVAD9%R-CHOP q3wk x 8 7%Involved-fieldradiation therapy7%Combination of theabove12%Other 6%No systemic therapy 1%0 10 20 30 40SOURCE: National Survey of Medical Oncologists, November 2008.14