Certified Co-Occurring Disorders Professional Application
Certified Co-Occurring Disorders Professional Application Form
Certified Co-Occurring Disorders Professional Application Form
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
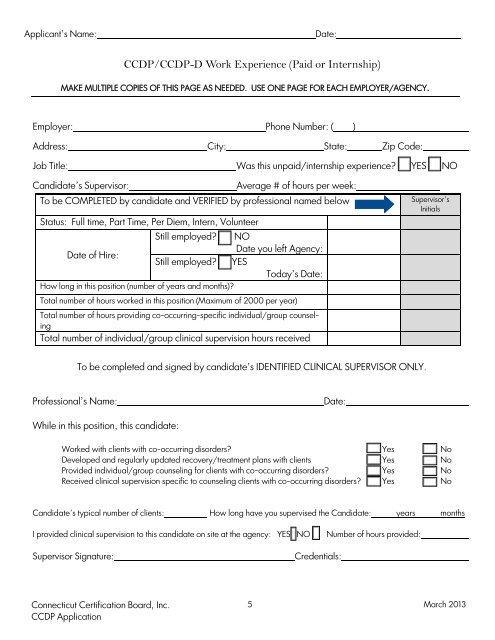
Applicant’s Name:<br />
Date:<br />
CCDP/CCDP-D Work Experience (Paid or Internship)<br />
MAKE MULTIPLE COPIES OF THIS PAGE AS NEEDED. USE ONE PAGE FOR EACH EMPLOYER/AGENCY.<br />
Employer: Phone Number: ( )<br />
Address: City: State: Zip <strong>Co</strong>de:<br />
Job Title:<br />
Candidate’s Supervisor:<br />
Was this unpaid/internship experience? YES NO<br />
Average # of hours per week:<br />
To be COMPLETED by candidate and VERIFIED by professional named below<br />
Status: Full time, Part Time, Per Diem, Intern, Volunteer<br />
Still employed? NO<br />
Date you left Agency:<br />
Date of Hire:<br />
Still employed? YES<br />
Today’s Date:<br />
How long in this position (number of years and months)?<br />
Supervisor’s<br />
Initials<br />
Total number of hours worked in this position (Maximum of 2000 per year)<br />
Total number of hours providing co-occurring-specific individual/group counseling<br />
Total number of individual/group clinical supervision hours received<br />
To be completed and signed by candidate’s IDENTIFIED CLINICAL SUPERVISOR ONLY.<br />
<strong>Professional</strong>’s Name:<br />
Date:<br />
While in this position, this candidate:<br />
Worked with clients with co-occurring disorders? Yes No<br />
Developed and regularly updated recovery/treatment plans with clients Yes No<br />
Provided individual/group counseling for clients with co-occurring disorders? Yes No<br />
Received clinical supervision specific to counseling clients with co-occurring disorders? Yes No<br />
Candidate’s typical number of clients: How long have you supervised the Candidate: years months<br />
I provided clinical supervision to this candidate on site at the agency: YES NO<br />
Number of hours provided:<br />
Supervisor Signature:<br />
Credentials:<br />
<strong>Co</strong>nnecticut Certification Board, Inc.<br />
CCDP <strong>Application</strong><br />
5<br />
March 2013