Unity Through Diversity Registration Booklet 2020

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
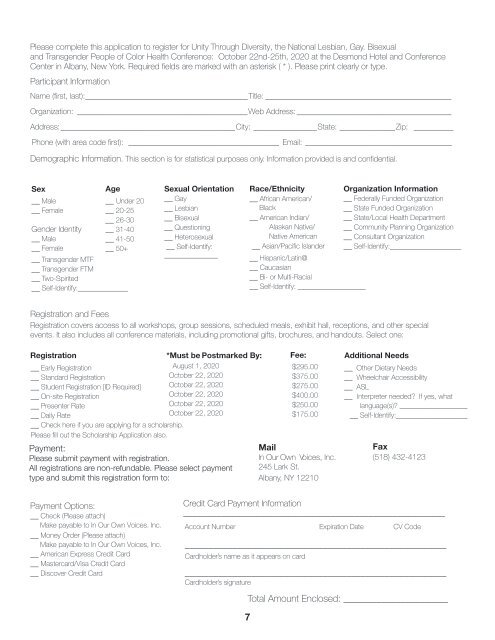
Please complete this application to register for <strong>Unity</strong> <strong>Through</strong> <strong>Diversity</strong>, the National Lesbian, Gay. Bisexual<br />
and Transgender People of Color Health Conference: October 22nd-25th, <strong>2020</strong> at the Desmond Hotel and Conference<br />
Center in Albany, New York. Required fields are marked with an asterisk ( * ). Please print clearly or type.<br />
Participant Information<br />
Name (first, last): _________________________________________Title: _______________________________________________<br />
Organization: ___________________________________________Web Address: _______________________________________<br />
Address: ____________________________________________City: ________________State: ______________Zip: __________<br />
Phone (with area code first): ______________________________________ Email: _____________________________________<br />
Demographic Information. This section is for statistical purposes only. Information provided is and confidential.<br />
Sex<br />
__ Male<br />
__ Female<br />
Age<br />
__ Under 20<br />
__ 20-25<br />
__ 26-30<br />
__ 31-40<br />
__ 41-50<br />
__ 50+<br />
Gender Identity<br />
__ Male<br />
__ Female<br />
__ Transgender MTF<br />
__ Transgender FTM<br />
__ Two-Spirited<br />
__ Self-Identify:______________<br />
Sexual Orientation<br />
__ Gay<br />
__ Lesbian<br />
__ Bisexual<br />
__ Questioning<br />
__ Heterosexual<br />
__ Self-Identify:<br />
_______________<br />
Race/Ethnicity Organization Information<br />
__ African American/ __ Federally Funded Organization<br />
Black<br />
__ State Funded Organization<br />
__ American Indian/ __ State/Local Health Department<br />
Alaskan Native/ __ Community Planning Organization<br />
Native American __ Consultant Organization<br />
__ Asian/Pacific Islander __ Self-Identify:____________________<br />
__ Hispanic/Latin@<br />
__ Caucasian<br />
__ Bi- or MuIti-Racial<br />
__ Self-Identify: ___________________<br />
<strong>Registration</strong> and Fees<br />
<strong>Registration</strong> covers access to all workshops, group sessions, scheduled meals, exhibit hall, receptions, and other special<br />
events. It also includes all conference materials, including promotional gifts, brochures, and handouts. Select one:<br />
<strong>Registration</strong><br />
__ Early <strong>Registration</strong><br />
__ Standard <strong>Registration</strong><br />
__ Student <strong>Registration</strong> [ID Required]<br />
__ On-site <strong>Registration</strong><br />
__ Presenter Rate<br />
__ Daily Rate<br />
__ Check here if you are applying for a scholarship.<br />
Please fill out the Scholarship Application also.<br />
*Must be P o s t m a r k e d By:<br />
August 1, <strong>2020</strong><br />
October 22, <strong>2020</strong><br />
October 22, <strong>2020</strong><br />
October 22, <strong>2020</strong><br />
October 22, <strong>2020</strong><br />
October 22, <strong>2020</strong><br />
Payment:<br />
Please submit payment with registration.<br />
All registrations are non-refundable. Please select payment<br />
type and submit this registration form to:<br />
Fee:<br />
$295.00<br />
$375.00<br />
$275.00<br />
$400.00<br />
$250.00<br />
$175.00<br />
Mail<br />
In Our Own Voices, Inc.<br />
245 Lark St.<br />
Albany, NY 12210<br />
Additional Needs<br />
__ Other Dietary Needs<br />
__ Wheelchair Accessibility<br />
__ ASL<br />
__ Interpreter needed? If yes, what<br />
language(s)? ___________________<br />
__ Self-Identify:____________________<br />
Fax<br />
(518) 432-4123<br />
Payment Options:<br />
__ Check (Please attach)<br />
Make payable to In Our Own Voices. Inc.<br />
__ Money Order (Please attach)<br />
Make payable to In Our Own Voices, Inc.<br />
__ American Express Credit Card<br />
__ Mastercard/Visa Credit Card<br />
__ Discover Credit Card<br />
Credit Card Payment Information<br />
_______________________________________________________<br />
Account Number<br />
Expiration Date<br />
_______________________________________________________<br />
Cardholder’s name as it appears on card<br />
CV Code<br />
_______________________________________________________<br />
Cardholder’s signature<br />
Total Amount Enclosed: ______________________<br />
7<br />
7