Injectables - Plastic Surgery Internal
Injectables - Plastic Surgery Internal
Injectables - Plastic Surgery Internal

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
SRPS • Volume 10 • Issue 28 • 2010<br />
inert surface. The most common biofilm example<br />
is dental plaque. Biofilms have impaired immune<br />
system penetration, reduced growth rates and/<br />
or susceptibility by quorum sensing, altered<br />
micro-environment, altered gene expression, and<br />
display. 132,143<br />
Routine culture techniques might be<br />
inadequate because they are based in the planktonic<br />
as opposed to the biofilm model. Improving culture<br />
results with techniques such as pyrosequencing,<br />
polymerase chain reaction (PCR), 144 fluorescence<br />
in situ hybridization, 145 or ultrasound sonication 146<br />
is an essential advance that should be considered<br />
when biofilms are suspected.<br />
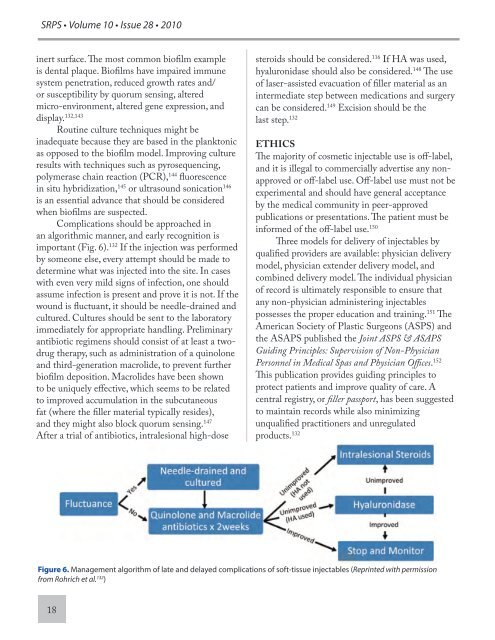
Complications should be approached in<br />
an algorithmic manner, and early recognition is<br />
important (Fig. 6). 132 If the injection was performed<br />
by someone else, every attempt should be made to<br />
determine what was injected into the site. In cases<br />
with even very mild signs of infection, one should<br />
assume infection is present and prove it is not. If the<br />
wound is fluctuant, it should be needle-drained and<br />
cultured. Cultures should be sent to the laboratory<br />
immediately for appropriate handling. Preliminary<br />
antibiotic regimens should consist of at least a twodrug<br />
therapy, such as administration of a quinolone<br />
and third-generation macrolide, to prevent further<br />
biofilm deposition. Macrolides have been shown<br />
to be uniquely effective, which seems to be related<br />
to improved accumulation in the subcutaneous<br />
fat (where the filler material typically resides),<br />
and they might also block quorum sensing. 147<br />
After a trial of antibiotics, intralesional high-dose<br />
18<br />
steroids should be considered. 116 If HA was used,<br />
hyaluronidase should also be considered. 148 The use<br />
of laser-assisted evacuation of filler material as an<br />
intermediate step between medications and surgery<br />
can be considered. 149 Excision should be the<br />
last step. 132<br />
ETHICS<br />
The majority of cosmetic injectable use is off-label,<br />
and it is illegal to commercially advertise any nonapproved<br />
or off-label use. Off-label use must not be<br />
experimental and should have general acceptance<br />
by the medical community in peer-approved<br />
publications or presentations. The patient must be<br />
informed of the off-label use. 150<br />
Three models for delivery of injectables by<br />
qualified providers are available: physician delivery<br />
model, physician extender delivery model, and<br />
combined delivery model. The individual physician<br />
of record is ultimately responsible to ensure that<br />
any non-physician administering injectables<br />
possesses the proper education and training. 151 The<br />
American Society of <strong>Plastic</strong> Surgeons (ASPS) and<br />
the ASAPS published the Joint ASPS & ASAPS<br />
Guiding Principles: Supervision of Non-Physician<br />
Personnel in Medical Spas and Physician Offices. 152<br />
This publication provides guiding principles to<br />
protect patients and improve quality of care. A<br />
central registry, or filler passport, has been suggested<br />
to maintain records while also minimizing<br />
unqualified practitioners and unregulated<br />
products. 132<br />
Figure 6. Management algorithm of late and delayed complications of soft-tissue injectables (Reprinted with permission<br />
from Rohrich et al. 132 )