Versatility of the Pedicled Anterolateral Thigh Flap - The Clinics
Versatility of the Pedicled Anterolateral Thigh Flap - The Clinics
Versatility of the Pedicled Anterolateral Thigh Flap - The Clinics

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
678<br />
Neligan & Lannon<br />
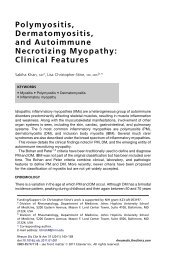
Fig. 1. <strong>The</strong> lateral circumflex artery (A), a branch <strong>of</strong><br />
<strong>the</strong> pr<strong>of</strong>unda femoris, has a lateral (ascending) branch<br />
(B) that supplies <strong>the</strong> tensor fasciae lata muscle (TFL)<br />
and a descending branch (C) that supplies <strong>the</strong> anterolateral<br />
thigh flap. This vessels runs under rectus femoris<br />
(RF) and <strong>the</strong>n in <strong>the</strong> septum, between rectus<br />
femoris and vastus lateralis (VL).<br />
recognizing that this method may not always be<br />
accurate. 15 <strong>The</strong> flap can be raised to include any<br />
<strong>of</strong> <strong>the</strong> elements supplied by <strong>the</strong> vasculature. It<br />
can incorporate muscle (vastus lateralis), fascia,<br />
and skin. <strong>The</strong> choice <strong>of</strong> which tissues to include<br />
will be dictated by <strong>the</strong> reconstructive requirements.<br />
<strong>The</strong> technique may be modified accordingly.<br />
For many <strong>of</strong> <strong>the</strong> reconstructive applications<br />
that a pedicled anterolateral thigh flap can address<br />
in <strong>the</strong> lower abdomen, <strong>the</strong> fascial element <strong>of</strong> <strong>the</strong><br />
Fig. 2. A line drawn between <strong>the</strong> anterior superior<br />
iliac spine and <strong>the</strong> lateral border <strong>of</strong> <strong>the</strong> patella is<br />
<strong>the</strong> surface marking <strong>of</strong> <strong>the</strong> septum between rectus<br />
femoris and vastus lateralis. <strong>The</strong> midportion <strong>of</strong> this<br />
line is where perforators will be found.<br />
flap can be important, which is particularly <strong>the</strong><br />
case when reconstructing through abdominal<br />
wall defects. Often, <strong>the</strong> amount <strong>of</strong> fascia required<br />
is larger than <strong>the</strong> amount <strong>of</strong> skin required. If this<br />
is <strong>the</strong> case, an excess <strong>of</strong> fascia over skin can easily<br />
be harvested (Fig. 3). Vascularized fascia lata in<br />
abdominal wall reconstruction is said to have <strong>the</strong><br />
advantage <strong>of</strong> preventing adhes between <strong>the</strong> fascia<br />
and <strong>the</strong> abdominal viscera. 16 If no fascia is<br />
required for <strong>the</strong> reconstruction, <strong>the</strong>n a skin-only<br />
flap can be designed and <strong>the</strong> fascia simply incised<br />
around <strong>the</strong> perforators (Fig. 4). Fur<strong>the</strong>rmore, if<br />
muscle is a required element <strong>of</strong> <strong>the</strong> reconstruction,<br />
<strong>the</strong> flap can be raised as a myocutaneous flap<br />
incorporating <strong>the</strong> vastus lateralis muscle. <strong>The</strong><br />
technique <strong>of</strong> dissection will depend on what<br />
elements are being included with <strong>the</strong> flap. <strong>The</strong><br />
dimensions <strong>of</strong> <strong>the</strong> flap will obviously be dictated<br />
by <strong>the</strong> size <strong>of</strong> <strong>the</strong> defect to be reconstructed.<br />
However, <strong>the</strong> vascular pedicle <strong>of</strong> <strong>the</strong> anterolateral<br />
thigh can carry a large flap (up to 30 cm). To<br />
perfuse such a large skin paddle, however, more<br />
than 1 perforator may need to be harvested with<br />
<strong>the</strong> flap. If multiple perforators are available, it is<br />
judicious to sequentially clamp <strong>the</strong>m so as to<br />
ensure that <strong>the</strong> selected perforators will perfuse<br />
<strong>the</strong> flap (see Fig. 4). Pedicle length can also be<br />
particularly important when <strong>the</strong> flap is being designed<br />
as a pedicled flap; <strong>the</strong> longer <strong>the</strong> pedicle,<br />
<strong>the</strong> greater <strong>the</strong> arc <strong>of</strong> rotation. Preoperative<br />
imaging may be particularly helpful when planning<br />
a pedicled anterolateral thigh flap because <strong>the</strong><br />
location <strong>of</strong> <strong>the</strong> perforator has a bearing on pedicle<br />
length and, <strong>the</strong>refore, on <strong>the</strong> arc <strong>of</strong> rotation <strong>of</strong> <strong>the</strong><br />
flap. A distally placed perforator, <strong>the</strong> C perforator<br />
according to Yu’s classification, can add considerable<br />
length and can be chosen if it is <strong>of</strong> appropriate<br />
size. <strong>The</strong> more distal perforators, however, tend to<br />
Fig. 3. <strong>The</strong> amount <strong>of</strong> fascia harvested with this flap<br />
exceeds <strong>the</strong> amount <strong>of</strong> skin. This picture shows <strong>the</strong><br />
excess thigh fascia being sutured to <strong>the</strong> abdominal<br />
wall fascia.