

Evaluation & Management of Adult Hypoglycemic Disorders
Evaluation & Management of Adult Hypoglycemic Disorders
Evaluation & Management of Adult Hypoglycemic Disorders

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
AN ENDOCRINE SOCIETY CLINICAL PRACTICE GUIDELINE<br />
12<br />
fall to hypoglycemic levels; hypoglycemia is the result<br />
<strong>of</strong> low rates <strong>of</strong> glucose production rather than high<br />
rates <strong>of</strong> glucose utilization (58). Thus, plasma insulin,<br />
C-peptide, and proinsulin concentrations need not be<br />
high relative to normal euglycemic values but only<br />
inappropriately high in the setting <strong>of</strong> low fasting<br />
plasma glucose concentrations (12–15). Critical<br />
diagnostic findings are plasma insulin concentrations<br />
<strong>of</strong> at least 3 µU/ml (18 pmol/liter), plasma C-peptide<br />
concentrations <strong>of</strong> at least 0.6 ng/ml (0.2 nmol/liter),<br />
and plasma proinsulin concentrations <strong>of</strong> at least<br />
5.0 pmol/liter when the fasting plasma glucose<br />
concentrations are below 55 mg/dl (3.0 mmol/liter)<br />
(14, 15). Ratios employing insulin and glucose have<br />
no diagnostic utility (59). These criteria assume the<br />
absence <strong>of</strong> intercurrent illnesses including renal<br />
insufficiency.<br />
An occasional patient with an insulinoma may not<br />
fulfill these criteria even during a 72-h fast (15, 60),<br />
and a few have plasma insulin levels below 3 µU/ml<br />
(18 pmol/liter) during fasting hypoglycemia, but<br />
plasma C-peptide levels are usually 0.6 ng/ml<br />
(0.2 mmol/liter) or greater and plasma proinsulin<br />
levels are usually 5.0 pmol/liter or greater in the latter<br />
patients. For example, in one series the plasma insulin<br />
criterion was met in 29 <strong>of</strong> 32 patients with an<br />
insulinoma, whereas the C-peptide and proinsulin<br />
criteria were met in all 32 patients (61). Plasma<br />
β-hydroxybutyrate levels <strong>of</strong> 2.7 mmol/liter or less and<br />
an increase in the plasma glucose concentration <strong>of</strong> at<br />
least 25 mg/dl (1.4 mmol/liter) after iv glucagon, the<br />
latter indicating preserved hepatic glycogen stores,<br />
provide biological evidence <strong>of</strong> insulin (or IGF) excess<br />
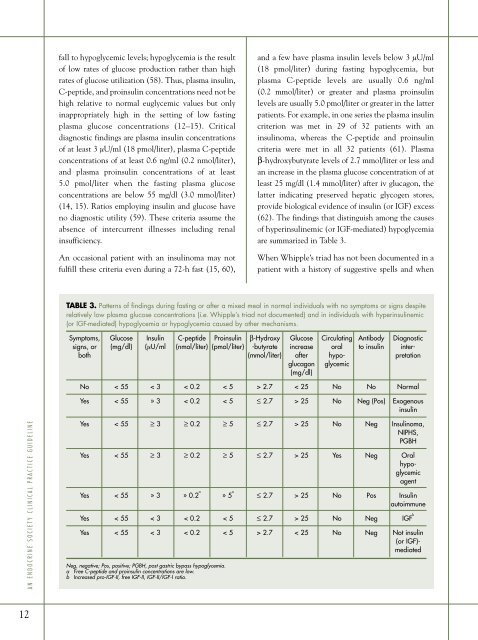
(62). The findings that distinguish among the causes<br />
<strong>of</strong> hyperinsulinemic (or IGF-mediated) hypoglycemia<br />
are summarized in Table 3.<br />
When Whipple’s triad has not been documented in a<br />
patient with a history <strong>of</strong> suggestive spells and when<br />
TABLE 3. Patterns <strong>of</strong> findings during fasting or after a mixed meal in normal individuals with no symptoms or signs despite<br />
relatively low plasma glucose concentrations (i.e. Whipple’s triad not documented) and in individuals with hyperinsulinemic<br />
(or IGF-mediated) hypoglycemia or hypoglycemia caused by other mechanisms.<br />
Symptoms, Glucose Insulin C-peptide Proinsulin β-Hydroxy Glucose Circulating Antibody Diagnostic<br />
signs, or (mg/dl) (µU/ml (nmol/liter) (pmol/liter) -butyrate increase oral to insulin interboth<br />
(mmol/liter) after hypo- pretation<br />
glucagon glycemic<br />
(mg/dl)<br />
No < 55 < 3 < 0.2 < 5 > 2.7 < 25 No No Normal<br />
Yes < 55 » 3 < 0.2 < 5 ≤ 2.7 > 25 No Neg (Pos) Exogenous<br />
insulin<br />
Yes < 55 ≥ 3 ≥ 0.2 ≥ 5 ≤ 2.7 > 25 No Neg Insulinoma,<br />
NIPHS,<br />
PGBH<br />
Yes < 55 ≥ 3 ≥ 0.2 ≥ 5 ≤ 2.7 > 25 Yes Neg Oral<br />
hypoglycemic<br />
agent<br />
Yes < 55 » 3 » 0.2 a<br />
» 5 a<br />
≤ 2.7 > 25 No Pos Insulin<br />
autoimmune<br />
Yes < 55 < 3 < 0.2 < 5 ≤ 2.7 > 25 No Neg IGF b<br />
Yes < 55 < 3 < 0.2 < 5 > 2.7 < 25 No Neg Not insulin<br />
(or IGF)mediated<br />
Neg, negative; Pos, positive; PGBH, post gastric bypass hypoglycemia.<br />
a Free C-peptide and proinsulin concentrations are low.<br />
b Increased pro-IGF-II, free IGF-II, IGF-II/IGF-I ratio.