Anesthetic Considerations for Awake Craniotomy for Epilepsy ... - Vtr
Anesthetic Considerations for Awake Craniotomy for Epilepsy ... - Vtr
Anesthetic Considerations for Awake Craniotomy for Epilepsy ... - Vtr

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
246<br />
Erickson & Cole<br />
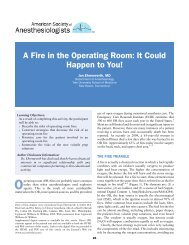
Fig. 1. Open craniotomy showing the cortical surface of a patient with bipolar stimulation<br />
using an Ojemann bipolar stimulator while testing appropriate neurologic function in an<br />
awake patient. Cortical labels shown include A (arm), F (face), and H (hand). (Courtesy of<br />
Fredric B. Meyer, MD.)<br />
aids are use to plan a linear trajectory from parietal surface to thalamus or structures<br />
near-thalamus, which avoids vasculature and ventricles. Once the styleted electrode<br />
lead is in place, microelectrode recordings (MERs) demonstrate changes in spontaneous<br />
neuronal firing as the electrode enters different nuclear or thalamic brain tissue.<br />
Recordings of both spontaneous neuronal discharge and changes in discharges with<br />
patient movement guide lead placement. Macrostimulation then begins and patients<br />
are observed <strong>for</strong> specific symptom amelioration and <strong>for</strong> adverse effects or unpleasant<br />
sensations resulting from stimulation. High-frequency stimulation (above 100 Hz)<br />
seems to improve symptoms whereas low frequencies have no effect. 113 The stylet<br />
is removed when satisfactory feedback is observed, and the lead is ready <strong>for</strong> tunneled<br />
connection to the pulse generator.<br />
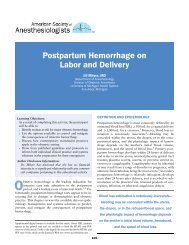
Fig. 2. An awake patient is positioned supine in pinion and under surgical drapes awake and is<br />
undergoing motor testing of the left upper extremity. (Courtesy of Fredric B. Meyer, MD.)