Spring (Vol. 11, No. 1) - San Francisco General Hospital Foundation
Spring (Vol. 11, No. 1) - San Francisco General Hospital Foundation
Spring (Vol. 11, No. 1) - San Francisco General Hospital Foundation

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
2<br />
S a n F r a n c i s c o G e n e r a l H o s p i t a l F o u n d a t i o n N e w s<br />
Palliative Care Service<br />
Continued from Page 1<br />
with the purpose of that room. She was there for several days before<br />
she died.<br />
“Even though she didn’t have family to be with her, she was<br />
comfortable from a physical and emotional standpoint. Our staff<br />
visited with her and held her hand. It was so powerful to see the high<br />
quality of care someone could get, even when she was all alone.”<br />
But usually people who receive Palliative Care Services are not alone.<br />
“A person’s life affects those around them. Often the way that people<br />
address illness is as a family unit,” says Kinderman. “Our service<br />
helps families. People have been able to die here with their loved ones<br />
around them.”<br />
Epperhart recalls one patient who was taken out of the hospital’s<br />
acute setting to live out her last days in a comfort care suite. Family<br />
members were able to sleep in the room and be with her round the<br />
clock.<br />
“I went in late one night and saw about 20 family members around<br />
her bed. They brought lots of food and were able to spend her last days<br />
with her,” Epperhart says. “Four generations were there, including<br />
great-grandchildren. It was important for the children to come to<br />
a place that didn’t look like a hospital room. We gave this woman<br />
respect and dignity, and she died as she lived, with people around.”<br />
In addition to providing a space for family members to be, the<br />
Palliative Care Service helps them communicate with medical teams<br />
and connect with social service programs throughout the city.<br />
“We have helped to fill in some significant holes for patients and<br />
families,” says Kinderman. “Often after someone dies, there’s very<br />
little structure in place to help support the family. We’ve been able to<br />
provide support and continuity for families that are grieving and trying<br />
to navigate a complicated system after their loved ones have passed.”<br />
“Our goal is not only to provide excellent<br />
direct patient care, but to share those<br />
methods with other institutions.”<br />
As with all SFGH programs, cultural sensitivity and competency are<br />
critical components of the Palliative Care Service. Different cultures<br />
bring different views and traditions to the end of life. A recent survey<br />
found that, at the end of life, affordability of care is a top concern<br />
for Asians and Latinos; for African-Americans the concern is about<br />
finding providers who respect their culture; and treating pain and<br />
discomfort is paramount for Caucasians.<br />
“It’s so important to have awareness of different cultures,” says<br />
Epperhart. “About 40 percent of our patients have limited English<br />
proficiency. We work very closely with our interpreters. We have<br />
to understand that in certain cultures it’s not the patient who’s the<br />
decision maker. It can be the spouse or children. That’s part of their<br />
tradition.”<br />
Just as important is the spiritual component of the Palliative Care<br />
Service. In February, chaplain Eric Nefstead joined the Palliative<br />
Care Team.<br />
“Part of human dignity is about making choices that are true to your<br />
spirit. The work of our team is to try and help people do that,” says<br />
Nefstead. “We listen to patients’ hopes and fears. As they give of<br />
themselves, it helps us give of ourselves and then the world is freed of<br />
some fear and pain. We can all recognize the joy of living even in the<br />
sad moments of our dying or that of our loved one.”<br />
Nefstead, who has been working in end-of-life care for 15 years, says<br />
he wears two hats as the Palliative Care Service chaplain. First, he is a<br />
clinician who works directly with patients.<br />
“Many of the people we serve at <strong>San</strong> <strong>Francisco</strong> <strong>General</strong> have<br />
experienced trauma in the form of poverty, immigration and<br />
substance abuse. That can make them afraid and distrustful of<br />
others,” he says. “As a chaplain, I can help them find their own voice<br />
and desire amidst the bigger system.”<br />
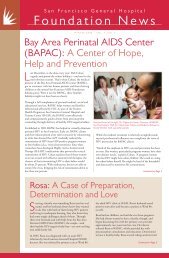
Regina Epperhart, MSW, Social Worker; Caroline Maroten, RN, NP;<br />
and Anne Kinderman, MD, Director, members of the Supportive and<br />
Palliative Care Service, SFGH discuss patient care strategies.<br />
Nefstead is also a teacher in the SFGH Clinical Pastoral Education<br />
program, training those who provide spiritual services at SFGH and<br />
beyond.<br />
“Part of what I teach theological students and religious leaders is how<br />
to listen attentively to people near the end of their lives. As spiritual<br />
leaders, we can help people discover their own spiritual resources as<br />
they face the reality of their death,” he continues. “Then when our<br />
students leave here, they can bring what they’ve learned to others in<br />
other hospitals.”<br />
In fact, just about every aspect of the Palliative Care Service is seen as<br />
a teaching opportunity.<br />
“Our goal is not only to provide excellent direct patient care, but to<br />
share those methods with other institutions,” says Kinderman. “We<br />
can show others around the world what people can experience at the<br />
end of life.”<br />
There is a strong practical element to palliative care, too. While over<br />
half of Americans express a preference to die at home, only onequarter<br />
do and approximately one-half die in a hospital. As a result,<br />
end-of-life care is costly, consuming 10 to 12 percent of all healthcare<br />
costs and the majority of Medicare expenditures in the year prior<br />
to death. With palliative care, the most appropriate services are<br />
provided to each patient, often instead of invasive and unnecessary<br />
medical treatments.<br />
While the Palliative Care Service is a recent addition to SFGH, it<br />
is already receiving a warm reception. Early predictions were that<br />
services would be provided to about 150 patients a year. At the time<br />
of this writing (three months into its existence), the program has<br />
already served more than 70 patients.<br />
“In a short amount of time, we’ve been able to dramatically<br />
improve the level of care that people receive at the end of life,” says<br />
Kinderman. “That’s had a visible impact on patients, family and staff<br />
across the hospital.”<br />
“What’s great about working with the palliative care team is that<br />
each person brings a spirit of appreciation for the fullness of life,”<br />
adds Nefstead. “<strong>No</strong> one is just a doctor or nurse here. Everyone is a<br />
humanitarian.”