Causes :
Causes :
Causes :

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
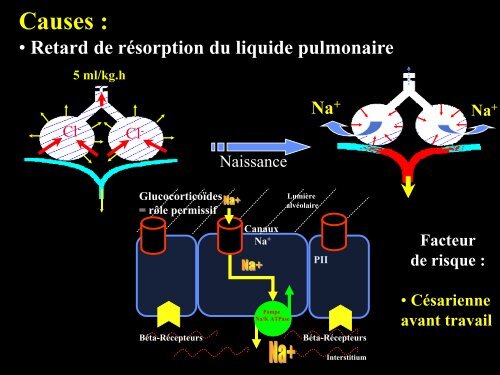
<strong>Causes</strong> :<br />
• Retard de résorption du liquide pulmonaire<br />
Cl -<br />
5 ml/kg.h<br />
Cl -<br />
Glucocorticoïdes<br />
= rôle permissif<br />
Naissance<br />
Canaux<br />
Na +<br />
Pompe<br />
Na/K ATPase<br />
Lumière<br />
alvéolaire<br />
Na +<br />
PII<br />
Béta-Récepteurs Béta-Récepteurs<br />
Interstitium<br />
Na +<br />
Facteur<br />
de risque :<br />
• Césarienne<br />
avant travail
<strong>Causes</strong> :<br />
• Maladie des Membranes Hyalines<br />
Effet<br />
« surfactant »<br />
Facteurs<br />
de risque :<br />
• Césarienne<br />
avant travail<br />
• Prématurité<br />
• Garçon<br />
• Naissance<br />
• Aggravation 24 H<br />
• Plateau 24 - 72 H<br />
• Récupération
<strong>Causes</strong> :<br />
• Autres causes :<br />
Infection materno-fœtale<br />
Inhalation méconiale<br />
Rupture Prématurée des Membranes<br />
Malformations : MAK, CC, omphalocelle, HDC<br />
Prématurité<br />
RPM<br />
Oligoamnios<br />
Détresse respiratoire<br />
« Syndrome<br />
inflammatoire<br />
Fœtal »
Flexion<br />
foetale<br />
Oligoamnios<br />
Augmentation<br />
P Alv-P Amniot<br />
Early Hum Dev 2005 Obstet Gynecol 1995<br />
Compression<br />
thoracique<br />
Réduction du volume pulmonaire foetal<br />
Ralentissement du développement pulmonaire<br />
(alvéolarization, angiogenèse)
Ralentissement du développement pulmonaire<br />
(alvéolarization, angiogenèse)<br />
Réduction du volume pulmonaire<br />
- Moins de générations bronchiques<br />
- Moins d’alvéoles<br />
- Moins de vaisseaux<br />
Inflammation/Infection<br />
Lipopolysaccharide Cytokines : IL1, TNF Sepsis<br />
Accélère<br />
Maturation<br />
pulmonaire<br />
Moins de MMH<br />
Pediatrics, 1996<br />
+<br />
Arrêt<br />
développement<br />
pulmonaire<br />
Inactive<br />
GMP<br />
-<br />
IL1, TNF<br />
eNOS<br />
PDE 5<br />
Anomalies<br />
Vasculaires<br />
fonctionnelles<br />
NO<br />
cGMP<br />
Réactivité anormale<br />
Endothélium<br />
SMC
Détresse respiratoire modérée du nouveau-né<br />
Hypoxémie<br />
= shunt droit-Gauche<br />
= « admission veineuse »<br />
90 90<br />
45 45<br />
PaO PaO22 (mmHg) (mmHg)<br />
30% 30%<br />
40% 40%<br />
Shunt=0 Shunt=0 % %<br />
Shunt=10%<br />
Shunt=10%<br />
FiO FiO22 Effet<br />
« surfactant »<br />
Shunt<br />
intra-pulmonaire
P vO 2<br />
Shunt intra-pulmonaire<br />
P AO 2<br />
(Max effect<br />
at 80 mmHg)<br />
Hypoxémie<br />
P AO 2<br />
Dérecrutement<br />
alvéolaire<br />
Résistance<br />
vasculaire<br />
Eur Respir J. 2002 ;20:6-11
Détresse respiratoire sévère du nouveau-né<br />
Hypoxémie<br />
= shunt droit-Gauche<br />
= « admission veineuse »<br />
55<br />
45<br />
PaO 2<br />
(mmHg)<br />
60%<br />
Shunt=0 %<br />
Shunt=20%<br />
100%
Pathologie parenchymateuse<br />
Shunt intrapulmonaire<br />
Alvéoli<br />
Hypoxémie<br />
HTAPP<br />
Shunt extrapulmonaire<br />
Alvéoli<br />
RA<br />
RV<br />
PA<br />
LA<br />
LV
Prise en charge<br />
1. Traitement préventif +++<br />
33-34 Semaines d’AG<br />
GC Placebo<br />
35-36 Semaines d’AG<br />
Corticothérapie anténatale<br />
Cochrane, 2006
Césarienne avant travail = Facteur de risque de<br />
Détresse Respiratoire<br />
N = 950<br />
Stutchfield P, BMJ, 2005
Prise en charge<br />
1. Traitement préventif +++<br />
Attention à l’orientation anténatale !<br />
Prendre en compte les facteurs de risque associés :<br />
• Rupture Prématurée des Membranes<br />
• Chorio-amniotite<br />
• Diabète gestationnel<br />
• Retard de croissance ….
Prévention de la MMH !<br />
Evolution de la MMH<br />
Naissance<br />
Aggravation : 24 H<br />
Plateau : 24 - 72 H<br />
Récupération<br />
O 2 thérapie<br />
Intubation/Ventilation<br />
Surfactant<br />
O 2<br />
O 2
Alvéoli<br />
PPC nasale<br />
Thorax<br />
Abdomen<br />
Vt<br />
Thoraco-abdominal<br />
synchronie<br />
Thoraco-abdominal<br />
asynchronie<br />
= 0° = 90°
Premature infants > 30 S and < 24 h after birth<br />
Respiratory failure (FiO 2>30% for > 30min)<br />
Headbox CPAP (bubble)<br />
End-Point :<br />
Treatment failure = FiO 2 > 60%, PCO 2 > 60 mmHg<br />
Pediatrics 2007;120:509<br />
16
Headbox<br />
N=149<br />
2920 g<br />
36 S<br />
N=300<br />
CPAP<br />
N=151<br />
2900 g<br />
36 S<br />
Failure: 47 (32%) 30 (20%<br />
Pediatrics 17 2007;120:509
Prophylactic<br />
NCPAP<br />
Premature infants<br />
24-27 weeks GA<br />
Intubation +<br />
Prophylactic Surfactant<br />
End-Point : Death or BPD<br />
Support Study Group, NEJM 2010<br />
18
N=1316<br />
GA 24 - 27 Weeks<br />
NCPAP<br />
N=653<br />
Surfactant<br />
19<br />
N=663<br />
Death or BPD: 48% 54%<br />
MV (days): 24 d 28d<br />
Steroids: 7% 13%<br />
Support Study Group, NEJM 2010
Prophylactic<br />
NCPAP<br />
Premature infants<br />
25-28 weeks GA<br />
Intubation +<br />
Prophylactic Surfactant<br />
(INSURE)<br />
End-Point : Need for MV within the first 5 days of<br />
Sandri, Pediatrics 2010<br />
20
N=208<br />
Mean GA = 27 Weeks<br />
NCPAP<br />
N=105<br />
Prophylactic<br />
Surfactant<br />
21<br />
N=103<br />
Need for MV: 33% 34%<br />
Death or BPD : 22% 22%<br />
Sandri, Pediatrics 2010
Prophylactic<br />
NCPAP<br />
Premature infants<br />
25-28 weeks GA<br />
Systematic<br />
Intubation<br />
End-Point : Death or BPD<br />
Morley, NEJM 2008<br />
22
N=616<br />
Mean GA = 27 Weeks<br />
NCPAP<br />
N=310<br />
Intubation<br />
23<br />
N=316<br />
Death or BPD : 33% 39%<br />
Duration of MV: 3d 4d*<br />
Duration of O 2: 42d 49d<br />
Morley, NEJM 2008
What are the physiological effects<br />
Mechanical characteristics of the<br />
immature respiratory system:<br />
Low lung<br />
compliance<br />
High<br />
chest<br />
compliance<br />
of NCPAP ?<br />
Low functional<br />
residual capacity ;<br />
Thoraco-abdominal<br />
asynchrony ;<br />
Mortola JP. J Appl 24 Physiol 1982
« Alveolar hypoventilation syndrome» :<br />
Increase in FiO 2 ;<br />
Increase in PaCO 2 ;<br />
Increase in RR ;<br />
Decrease in compliance;<br />
Increase in Work of<br />
breathing;<br />
Chest X-ray : distal<br />
atelectasis ;<br />
Episodes of desaturation ;<br />
25
Lung<br />
volumes<br />
Tidal<br />
Volume<br />
Dynamic<br />
Function<br />
al<br />
Residual<br />
Capacity<br />
Inspiration<br />
Closing<br />
volume<br />
Expiration<br />
Mortola JP. J Appl 26 Physiol 1982
Dynamic elevation of FRC through :<br />
Expiratory braking :<br />
• Activation of the inspiratory<br />
muscles ;<br />
• Active glottal narrowing ;<br />
Increase in respiratory rate :<br />
Magnenant E. Pediatr 27 Pulmonol, 200
easurement of the dynamic elevation of<br />
the end-expiratory lung volume (EELV)<br />
Flow<br />
=RC<br />
Dynamic<br />
EELV<br />
Volume<br />
Estimated<br />
passive<br />
EELV<br />
Dynamic<br />
EELV<br />
Passive<br />
EELV<br />
(Vr)<br />
Spontaneous<br />
breathing<br />
Vt<br />
EELV<br />
Passive<br />
breathing<br />
28<br />
Storme L et al. Pediatr Pulmonol, 1992
Effect of NCPAP on the end-expiratory lung<br />
volume<br />
NCPAP 0 2 4 6 8 cm<br />
Elgellab A, et al. Intensive 29 Care Med.<br />
2001.
300<br />
250<br />
200<br />
150<br />
100<br />
50<br />
0<br />
Change in end-expiratory lung volume<br />
with NCPAP (expressed as % Vt)<br />
0 2 4 6 8<br />
Elgellab A, et al. Intensive 30 Care Med.<br />
2001.<br />
cmH 2O
FRC<br />
0 cmH 2O<br />
VT<br />
Closing<br />
volume<br />
4 cmH 2O<br />
Effect of Variable-Flow<br />
NCPAP on FRC<br />
FRC<br />
CPAP=0<br />
31<br />
FRC<br />
CPAP=4
NCPAP = 0<br />
NCPAP = 2<br />
NCPAP = 4<br />
NCPAP = 6<br />
Effect of NCPAP<br />
on the breathing<br />
strategy<br />
Variable-Flow NCPAP :<br />
• Decreased the slope<br />
• Decreased Delta EELV<br />
32<br />
E Magnenant et al. Pediatr Pulmonol. 200
1<br />
0,8<br />
0,6<br />
0,4<br />
0,2<br />
0<br />
Effects of Variable-Flow NCPAP (IF)<br />
on the dynamic elevation of FRC (%Vt0)<br />
CPAP0 CPAP2 CPAP4 CPAP6<br />
*<br />
E Magnenant et al. Pediatr Pulmonol. 2004<br />
33<br />
*
FRC<br />
No<br />
CPAP<br />
Closing volume<br />
E Magnenant et al. Pediatr Pulmonol. 2004<br />
CPAP<br />
34
What are the physiological effects<br />
High<br />
chest<br />
of variable-flow NCPAP ?<br />
compliance<br />
Low lung<br />
compliance<br />
Low functional<br />
residual capacity ;<br />
Thoraco-abdominal<br />
asynchrony ;<br />
35
Rib cage<br />
Abdomen<br />
Vt<br />
Thoraco-abdominal<br />
synchrony<br />
= 0°<br />
Thoraco-abdominal<br />
asynchrony<br />
= 90°<br />
36
Rib cage<br />
Thoraco-abdominal asynchrony<br />
Abdomen<br />
37
Effect of variable-flow CPAP (IF)<br />
on thoraco-abdominal synchrony<br />
Elgellab A, et al. Intensive 38 Care Med.<br />
2001.
Multiple NCPAP devices
Multiple CPAP generators<br />
40
Multiple NCPAP prongs<br />
41
Infant-Flow @<br />
« Coanda » Effect<br />
Childs, Neonatal Intensive Care,<br />
2000
Childs,<br />
Neonatal Intensive<br />
Care,<br />
2000<br />
Inspiration<br />
Infant-Flow @<br />
Expiration
Inspiration<br />
Vortex<br />
Infant-Flow @ LP<br />
Branche<br />
expiratoire<br />
Narine<br />
Fluidic<br />
Flip<br />
Expiration<br />
Vortex
Infant-Flow @ LP<br />
Inspiration Expiration
Expiratory<br />
Gaz flow<br />
Inspiratory<br />
Gaz flow<br />
Pressure sensor<br />
Upper<br />
Airways<br />
During Expiration
Variable-Flow CPAP<br />
High gas flow<br />
High pressure<br />
Kinetic<br />
Energy+++<br />
CPAP<br />
• Resistance=0<br />
• Gradient<br />
Pressure=0<br />
Conventionnal<br />
Constant-Flow CPAP<br />
CPAP<br />
47<br />
• Resistance<br />
• Gradient pressur
Conventional NCPAP<br />
Variable-Flow<br />
NCPAP<br />
De Paoli et al. Arch Dis Child Fetal Ed, 2002<br />
Pressure drop<br />
48
In Premature infants < 1000 g,<br />
Binasal CPAP > Mononasal CPAP<br />
To wean from CMV<br />
><br />
Arch Dis Child Fetal Neonatal 49 Ed. 2001;85:F82-F8
In premature infants,<br />
Infant-Flow CPAP > nasal canula CPAP<br />
><br />
Pediatrics. 2001;107:304-308<br />
Arch Dis Child Fetal Neonatal Ed. 2001;85:F86-F9<br />
50
14<br />
12<br />
10<br />
8<br />
6<br />
4<br />
2<br />
0<br />
Change in FRC (ml/kg)<br />
Infants < 1500 g<br />
0 cmH2O 4 cmH2O 6 cmH2O 8 cmH2O<br />
Pediatrics. 2001;107:304-308<br />
51<br />
Infant-Flow<br />
Binasal<br />
Mononasal
45<br />
40<br />
35<br />
30<br />
25<br />
20<br />
FiO2 (%)<br />
Preterm < 36 S, HMD<br />
Mononasal<br />
H0 H12 H24 H36 H48<br />
Infant-Flow<br />
Arch Dis Child Fetal Neonatal Ed. 2001;85:F86-F<br />
52
In preterm < 2000 g,<br />
Nasal short prongs (2.5 l/mn) = nasal CPAP<br />
In reducing apnea<br />
=<br />
Pediatrics.2001;107:1081-1083<br />
53
In preterm infants,<br />
Mean GA 31 weeks,<br />
Variable flow NCPAP > Bubble CPAP or NIPPV<br />
In reducing apnea<br />
><br />
54<br />
Pantalitschka T, Arch Dis Child 2009
High flow nasal cannula<br />
Lampland A, J Pediatr 2009<br />
55
GA = 29 ± 1<br />
weeks<br />
BW = 1350 ± 1 g<br />
N=19<br />
Random order<br />
H Boumecid et al<br />
Arch Dis Child Fetal Ed,
Résultats<br />
FR / min<br />
Babyflow Infant-<br />
Flow<br />
56 10<br />
52 9<br />
Canule 2L Canule 6L<br />
59 11<br />
59 10<br />
SpO2 % 94 3 94 2 93 2 94 2<br />
FiO2 26 3 25 3 26 3 25 3<br />
TcPCO2 48 7 47 8 51 8 49 8<br />
H Boumecid et al<br />
Arch Dis Child Fetal Ed,
Vt ml/kg<br />
8<br />
7<br />
6<br />
5<br />
4<br />
3<br />
2<br />
*<br />
Baby Flow Infant Flow Lunettes 2L Lunettes 6L<br />
* : p< 0,05<br />
*<br />
*
Constant-Flow<br />
NCPAP<br />
Variable-Flow<br />
NCPAP<br />
Nasal cannulae
Effects of CPAP devices on the dynamic elevation of FR<br />
H Boumecid et al Arch Dis Child Fetal Ed,<br />
60
Effects of CPAP devices on the thoraco-abdominal synch<br />
* P < 0,05<br />
H Boumecid et al Arch Dis 61 Child Fetal Ed,
Effects of CPAP devices on the rib cage contribution to V<br />
* P < 0,05<br />
H Boumecid et al Arch Dis 62 Child Fetal Ed,
In preterm infants,<br />
Mean GA 31.5 weeks,<br />
Constant flow NCPAP > Nasal cannula<br />
In reducing extubation failure<br />
Abdel-Adi, Early Hum Dev 2011
Canule nasale : risques potentiels<br />
Moins efficace que NCPAP<br />
Surpression ???<br />
Lésions narinaires ???<br />
64
20 preterm infants<br />
GA : 26 weeks<br />
BW : 1000 g<br />
CPAP Bi-PAP CPAP Bi-PAP<br />
Migliori C et al. Pediatr Pulmonol, 2005<br />
But low change in P, trigger, technical lag
NCPAP<br />
N=20<br />
GA 28 - 34 Weeks<br />
Mean 30.2 W<br />
Bi level<br />
NCPAP<br />
N=20<br />
NCPAP (d): 6.2 3.8*<br />
O2 (days): 13.8 6.5*<br />
Arch Dis Child Fetal Neonatal Ed 2010 95: F85-F89<br />
66
Pressure controlled NCPAP (SLE1000)<br />
CPAP<br />
setting<br />
Flow<br />
Pressure
« Bubble » effects<br />
J Pediatr 2009;154:645-50
Effet de l’installation sur l’efficacité de la CPAP<br />
LE DECUBITUS VENTRAL
140<br />
120<br />
100<br />
80<br />
60<br />
40<br />
20<br />
Angle (degré) Thorax<br />
0<br />
DD DLG DV<br />
Abdomen<br />
70
2. Traitement curatif<br />
Management<br />
de l’hypoxémie<br />
Réduire le shunt<br />
Shunt intrapulmonaire Shunt extrapulmonaire<br />
"Recrutement alvéolaire" "Recrutement vasculaire"<br />
Observation clinique :<br />
Radiographie<br />
Echo-cardiographie
Alvéoli<br />
Alvéoli<br />
• Anamnèse : Pas de Corticothérapie RPM/Anamnios<br />
• AG : Prématuré Proche du terme<br />
• Pathologie : MMH Inhalation IMF, HDC<br />
• Clinique : Peu sévère à sévère Sévère/Instable<br />
Stable<br />
Pas de Gradient SpO 2 Gradient SpO 2<br />
RA<br />
RV<br />
PA<br />
LA<br />
LV
Valeur cible de SpO 2<br />
Pré-ductal : SpO 2 plus élevée<br />
OD<br />
Ao<br />
PA<br />
RA AP<br />
RV<br />
VD<br />
OG<br />
DA<br />
VG<br />
LV<br />
Post-ductal : SpO 2 plus basse<br />
DO 2= 1.3 x AoFlow x Hb x SpO 2<br />
FiO 2 doit être réglée selon la SpO 2<br />
PRE-DUCTALE !!!!
Alveoli<br />
Alveoli<br />
Shunt intra-pulmonaire Shunt extra-pulmonaire<br />
RA<br />
RV<br />
PA<br />
LA<br />
LV
PA<br />
de 0.25 à 0.35 m.s<br />
LPA<br />
DA<br />
Ao<br />
Doppler Artère<br />
Pulmonaire droite<br />
Para-mediastinal<br />
short axis view<br />
Rozé, Lancet 1994<br />
Gournay, Acta Paediatr 1998<br />
Artère<br />
Pulmonaire<br />
Gauche
PA<br />
LPA<br />
DA<br />
Ao<br />
Para-mediastinal<br />
Short axis view
Alvéoli<br />
Alvéoli<br />
VmoyAPG > 0.2 – 0.3 m.s < 0.2 m.s<br />
Shunt G-D Shunt D-G<br />
RA<br />
RV<br />
PA<br />
LA<br />
LV
Shunt intra-pulmonaire prédominant<br />
« Recrutement alvéolaire »<br />
Alvéoli<br />
= restaurer la CRF<br />
• Surfactant<br />
• Pression +<br />
Réduire le débit<br />
P AO 2<br />
De shunt<br />
P AO 2<br />
• Accentuer la vasoconstriction hypoxique<br />
• Vol vasculaire
Recrutement alvéolaire<br />
1. Pression moyenne de<br />
ventilation<br />
Pression<br />
V<br />
Pmax<br />
PEEP<br />
T insp . T exp.<br />
T insp<br />
Alvéoli<br />
Pression<br />
Moyenne<br />
Temps
Neurally Adjusted Ventilatory Assist<br />
CNS<br />
Phrenic nerve<br />
Diaphragmatic contraction<br />
Pressure, flow, volume<br />
Lung expansion<br />
( NAVA)<br />
NAVA<br />
Synchronised,<br />
proportional<br />
VAC<br />
-Synchronised,<br />
- no proportional<br />
- Asynchronisms<br />
VENTILATOR
Pressure = EaDi x NAVA gain<br />
Measurement of the electrical activity of the<br />
diaphragm (EaDi)<br />
Ventilator
Pression<br />
HFV / HFO<br />
Inspiration<br />
Pic à Pic<br />
P moyenne<br />
Temps
Recrutement alvéolaire<br />
2. Surfactant ….<br />
…Oui mais à quel moment ?<br />
Effet<br />
« surfactant »<br />
Administration « tardive » de surfactant (FiO2 > 45%) :<br />
• Augmente risque de PNO (x2)<br />
• Augmente risque de DBP (x2)<br />
• Augmente le risque de PCA (x2)<br />
Stevens TP, Cochrane, 2007
Shunt extra-pulmonaire prédominant<br />
« Recrutement vasculaire »<br />
Réduire les<br />
Résistances<br />
Vasculaires<br />
pulmonaires<br />
AP<br />
R<br />
A<br />
VD<br />
PV<br />
OG<br />
VG
1. Attention aux facteurs aggravants (déclenchant)<br />
Surdistention pulmonaire<br />
RVP<br />
V Houfflin.<br />
Am J Physiol, 2005<br />
PVR(mmHg/mL/min)<br />
1.2<br />
1.0<br />
0.8<br />
0.6<br />
0.4<br />
Stress<br />
-20 0 20 40 60 80 100 120 140<br />
Time (min)<br />
RVP<br />
suf+formol (n=6) formol (n=8)<br />
Stress<br />
Dopamine<br />
Jaillard S, Am J Physiol. 2001<br />
Bouissou, J Pediatr 2008
2. Recrutement alvéolaire si nécessaire<br />
P AO 2<br />
Gommers D. Crit Care Med. 1997<br />
Kinsella J. J Pediatr. 1997
3. Corriger une acidose respiratoire<br />
Q pulm<br />
PVR<br />
pH<br />
Temps<br />
Abman SH, 1992
Q Lung<br />
PVR<br />
pH<br />
Time<br />
Time<br />
Time<br />
Effet transitoire de l’alcalose respiratoire<br />
Abman SH, 1992
4. NO inhalé (10 à 40 ppm)<br />
Alveole<br />
RA<br />
RV<br />
PV<br />
LA<br />
LV<br />
Ductus<br />
arteriosus<br />
NO i<br />
NO
5. Améliorer la PvO 2<br />
PvO 2<br />
P AO 2
PvO2<br />
VO 2<br />
Débit d’O 2 délivré<br />
= 1.3 x Qc x Hb x SpO 2<br />
Qc<br />
VO 2<br />
Anaérobie<br />
Lactate<br />
DO 2<br />
Critique<br />
Aérobie<br />
PvO 2<br />
Délivrance O 2<br />
EO 2<br />
PvO 2
Hernie Diaphragmatique Congénitale<br />
Diminution volume pulmonaire<br />
- Moins de bronches<br />
- Moins d’alvéoles<br />
- Moins de vaisseaux +++<br />
< 30%<br />
Du volume<br />
Attendu<br />
+<br />
Control<br />
Réactivité<br />
Vasculaire<br />
anormale<br />
+<br />
Remodellage<br />
vasculaire<br />
CDH
NO i ? NO i / PGI 2<br />
HTAP<br />
OD<br />
VD<br />
CA<br />
OG<br />
VG<br />
HTAP + hypoperfusion pulm + IC
Résumé et Conclusion<br />
• La CAN à 33-34S d’AG réduit le risque de DR ;<br />
• La RPM, la macrosomie, la césarienne avant travail, la pré<br />
éclampsie, la chorio-amniotite augmentent le risque et la<br />
gravité des DR chez les enfants proches du terme :<br />
Attention à l’orientation anténatale<br />
• Les formes sévères de DR des enfants proche du terme<br />
nécessitent un transfert en réanimation :<br />
Comprendre le mécanisme de l’hypoxémie est un pré-requis<br />
pour optimiser le traitement<br />
• La MMH est responsable d’une hypoxémie progressivement<br />
croissante :<br />
La prévention est possible !<br />
• La MMH peut se compliquer de PNO, d’une insuffisance<br />
respiratoire sévère, et d’HTAP chez les enfants proche du<br />
terme, notamment après une RPM ou par césarienne avant<br />
travail.