La zircone dans le domaine de la prothèse amovible - Zirkonzahn
La zircone dans le domaine de la prothèse amovible - Zirkonzahn
La zircone dans le domaine de la prothèse amovible - Zirkonzahn
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
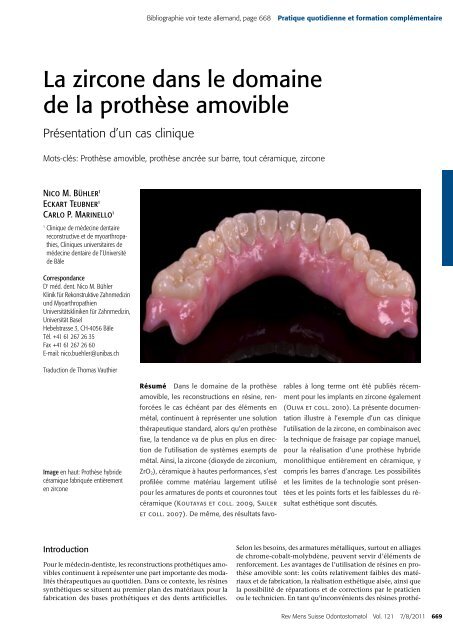
Bibliographie voir texte al<strong>le</strong>mand, page 668 Pratique quotidienne et formation complémentaire<strong>La</strong> <strong>zircone</strong> <strong>dans</strong> <strong>le</strong> <strong>domaine</strong><strong>de</strong> <strong>la</strong> prothèse amovib<strong>le</strong>Présentation d’un cas cliniqueMots-clés: Prothèse amovib<strong>le</strong>, prothèse ancrée sur barre, tout céramique, <strong>zircone</strong>Nico M. Büh<strong>le</strong>r 1Eckart Teubner 1Carlo P. Marinello 11Clinique <strong>de</strong> mé<strong>de</strong>cine <strong>de</strong>ntairereconstructive et <strong>de</strong> myoarthropathies,Cliniques universitaires <strong>de</strong>mé<strong>de</strong>cine <strong>de</strong>ntaire <strong>de</strong> l’Université<strong>de</strong> Bâ<strong>le</strong>CorrespondanceD r méd. <strong>de</strong>nt. Nico M. Büh<strong>le</strong>rKlinik für Rekonstruktive Zahnmedizinund MyoarthropathienUniversitätskliniken für Zahnmedizin,Universität BaselHebelstrasse 3, CH-4056 Bâ<strong>le</strong>Tél. +41 61 267 26 35Fax +41 61 267 26 60E-mail: nico.bueh<strong>le</strong>r@unibas.chTraduction <strong>de</strong> Thomas VauthierImage en haut: Prothèse hybri<strong>de</strong>céramique fabriquée entièrementen <strong>zircone</strong>Résumé Dans <strong>le</strong> <strong>domaine</strong> <strong>de</strong> <strong>la</strong> prothèseamovib<strong>le</strong>, <strong>le</strong>s reconstructions en résine, renforcées<strong>le</strong> cas échéant par <strong>de</strong>s éléments enmétal, continuent à représenter une solutionthérapeutique standard, alors qu’en prothèsefixe, <strong>la</strong> tendance va <strong>de</strong> plus en plus en direction<strong>de</strong> l’utilisation <strong>de</strong> systèmes exempts <strong>de</strong>métal. Ainsi, <strong>la</strong> <strong>zircone</strong> (dioxy<strong>de</strong> <strong>de</strong> zirconium,ZrO 2), céramique à hautes performances, s’estprofilée comme matériau <strong>la</strong>rgement utilisépour <strong>le</strong>s armatures <strong>de</strong> ponts et couronnes toutcéramique (Koutayas et coll. 2009, Sai<strong>le</strong>ret coll. 2007). De même, <strong>de</strong>s résultats favorab<strong>le</strong>sà long terme ont été publiés récemmentpour <strong>le</strong>s imp<strong>la</strong>nts en <strong>zircone</strong> éga<strong>le</strong>ment(Oliva et coll. 2010). <strong>La</strong> présente documentationillustre à l’exemp<strong>le</strong> d’un cas cliniquel’utilisation <strong>de</strong> <strong>la</strong> <strong>zircone</strong>, en combinaison avec<strong>la</strong> technique <strong>de</strong> fraisage par copiage manuel,pour <strong>la</strong> réalisation d’une prothèse hybri<strong>de</strong>monolithique entièrement en céramique, ycompris <strong>le</strong>s barres d’ancrage. Les possibilitéset <strong>le</strong>s limites <strong>de</strong> <strong>la</strong> technologie sont présentéeset <strong>le</strong>s points forts et <strong>le</strong>s faib<strong>le</strong>sses du résultatesthétique sont discutés.IntroductionPour <strong>le</strong> mé<strong>de</strong>cin-<strong>de</strong>ntiste, <strong>le</strong>s reconstructions prothétiques amovib<strong>le</strong>scontinuent à représenter une part importante <strong>de</strong>s modalitésthérapeutiques au quotidien. Dans ce contexte, <strong>le</strong>s résinessynthétiques se situent au premier p<strong>la</strong>n <strong>de</strong>s matériaux pour <strong>la</strong>fabrication <strong>de</strong>s bases prothétiques et <strong>de</strong>s <strong>de</strong>nts artificiel<strong>le</strong>s.Selon <strong>le</strong>s besoins, <strong>de</strong>s armatures métalliques, surtout en alliages<strong>de</strong> chrome-cobalt-molybdène, peuvent servir d’éléments <strong>de</strong>renforcement. Les avantages <strong>de</strong> l’utilisation <strong>de</strong> résines en prothèseamovib<strong>le</strong> sont: <strong>le</strong>s coûts re<strong>la</strong>tivement faib<strong>le</strong>s <strong>de</strong>s matériauxet <strong>de</strong> fabrication, <strong>la</strong> réalisation esthétique aisée, ainsi que<strong>la</strong> possibilité <strong>de</strong> réparations et <strong>de</strong> corrections par <strong>le</strong> praticienou <strong>le</strong> technicien. En tant qu’inconvénients <strong>de</strong>s résines prothé-Rev Mens Suisse Odontostomatol Vol. 121 7/8/2011 669
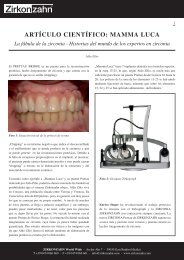
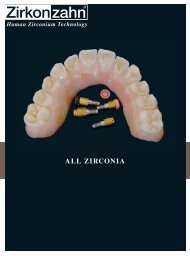
Pratique quotidienne et formation complémentaire <strong>La</strong> <strong>zircone</strong> <strong>dans</strong> <strong>le</strong> <strong>domaine</strong> <strong>de</strong> <strong>la</strong> prothèse amovib<strong>le</strong>tiques, il y a lieu d’évoquer <strong>la</strong> qualité re<strong>la</strong>tivement défavorab<strong>le</strong><strong>de</strong>s surfaces, l’affinité é<strong>le</strong>vée pour <strong>le</strong>s biofilms oraux et l’absorptiond’eau (gonf<strong>le</strong>ment) en comparaison avec <strong>le</strong>s métaux et <strong>le</strong>scéramiques. De plus, <strong>le</strong>s résines subissent assez rapi<strong>de</strong>ment <strong>de</strong>sprocessus <strong>de</strong> vieillissement qui peuvent avoir <strong>de</strong>s répercussionsgênantes sur <strong>le</strong>ur stabilité, <strong>de</strong> même qu’au p<strong>la</strong>n <strong>de</strong> l’esthétiqueet <strong>de</strong> l’hygiène (Bettencourt et coll. 2010). D’autre part, l’utilisation<strong>de</strong> métaux pour <strong>le</strong>s armatures <strong>de</strong> renforcement esttechniquement exigeante et influence <strong>le</strong> résultat esthétique.Dans <strong>de</strong>s cas rares, on observe en outre <strong>de</strong>s réactions al<strong>le</strong>rgiquesaux métaux ou résines (Jorge et coll. 2003, Wirz et coll.2003).<strong>La</strong> <strong>zircone</strong> est une céramique à hautes performances qui seprofi<strong>le</strong> progressivement <strong>dans</strong> <strong>le</strong> <strong>domaine</strong> <strong>de</strong> <strong>la</strong> prothèse fixecomme matériau idéal pour <strong>la</strong> réalisation d’armatures <strong>de</strong> couronneset <strong>de</strong> bridges, <strong>de</strong> tenons radicu<strong>la</strong>ires ainsi que pour <strong>la</strong>fabrication d’imp<strong>la</strong>nts et <strong>de</strong> mésostructures (abutments) (Olivaet coll. 2010, Özkurt & Kazazoglou 2010, Koutayas et coll.2009, Vagkopoulou et coll. 2009, Denry & Kelly 2008, Sai<strong>le</strong>ret coll. 2007). Mais à ce jour, <strong>la</strong> <strong>zircone</strong> reste peu utilisée enprothèse amovib<strong>le</strong>. Quelques travaux se sont limités à documenter<strong>de</strong>s applications <strong>de</strong> <strong>la</strong> <strong>zircone</strong> pour <strong>la</strong> fabrication d’élémentsd’ancrage comme <strong>le</strong>s attachements bou<strong>le</strong> ou <strong>le</strong>s barresen céramique (Büttel et coll. 2008, Rösch & Mericske-Stern2008, Carracho & Razzoog 2006). Depuis peu, certains auteursont décrit <strong>la</strong> possibilité <strong>de</strong> fabriquer l’ensemb<strong>le</strong> <strong>de</strong> <strong>la</strong> prothèseamovib<strong>le</strong> en <strong>zircone</strong> (Karl & Bauernschmidt 2010).<strong>La</strong> présente contribution documente <strong>la</strong> réalisation d’uneprothèse hybri<strong>de</strong> amovib<strong>le</strong> <strong>dans</strong> <strong>le</strong> maxil<strong>la</strong>ire inférieur, entièrementfabriquée en <strong>zircone</strong>, ancrée sur <strong>de</strong>ux barres fraisées,éga<strong>le</strong>ment en <strong>zircone</strong>, coloriées individuel<strong>le</strong>ment, chacune sur<strong>de</strong>ux imp<strong>la</strong>nts. Sur <strong>la</strong> base du système <strong>Zirkonzahn</strong> ® (<strong>Zirkonzahn</strong>GmbH, 39030 Gais, Italie), <strong>le</strong>s auteurs documentent <strong>le</strong>sétapes cliniques du traitement et <strong>le</strong>s techniques <strong>de</strong> <strong>la</strong>boratoirey re<strong>la</strong>tives.Principaux désirs <strong>de</strong> <strong>la</strong> patiente<strong>La</strong> patiente, âgée <strong>de</strong> 70 ans, est gênée par sa prothèse hybri<strong>de</strong>inférieure, pour <strong>de</strong>s raisons esthétiques et fonctionnel<strong>le</strong>s. <strong>La</strong>prothèse existante irrite <strong>la</strong> muqueuse, généra<strong>le</strong>ment sensib<strong>le</strong>,et provoque <strong>de</strong>s dou<strong>le</strong>urs. Objectivement, on observe uneadaptation insuffisante <strong>de</strong> <strong>la</strong> base prothétique <strong>dans</strong> <strong>le</strong>s régions<strong>de</strong>s <strong>de</strong>nts postérieures, ainsi qu’une infra-occlusion, <strong>de</strong>ux raisonsqui entraînent une stabilité réduite <strong>de</strong> <strong>la</strong> prothèse, enparticulier lors <strong>de</strong> <strong>la</strong> mastication. <strong>La</strong> patiente souhaite faireréaliser une nouvel<strong>le</strong> reconstruction amovib<strong>le</strong>, pour <strong>de</strong>s raisonshygiéniques éga<strong>le</strong>ment. Dans <strong>le</strong> maxil<strong>la</strong>ire supérieur, <strong>la</strong> patienteprésente <strong>de</strong>s restaurations par prothèse conjointe. Il estprévu <strong>de</strong> revoir <strong>la</strong> situation <strong>dans</strong> <strong>le</strong> maxil<strong>la</strong>ire supérieur <strong>dans</strong>un <strong>de</strong>uxième temps et <strong>de</strong> procé<strong>de</strong>r alors à une nouvel<strong>le</strong> réhabilitationpar prothèse fixe conventionnel<strong>le</strong>.En raison d’une hypertension artériel<strong>le</strong> et d’une hypercho<strong>le</strong>stérolémie,<strong>la</strong> patiente est traitée par son mé<strong>de</strong>cin <strong>de</strong> famil<strong>le</strong> pardu Cotenolol-Mepha-Neo ® et par Sortis ® , respectivement. Enoutre, <strong>la</strong> patiente prend – à titre prophy<strong>la</strong>ctique, en raison d’uninfarctus <strong>de</strong> <strong>la</strong> rétine survenu <strong>de</strong>ux ans auparavant – un inhibiteur<strong>de</strong> l’agrégation p<strong>la</strong>quettaire (Aspirine Cardio 100 ® ).A <strong>la</strong> suite <strong>de</strong> caries et <strong>de</strong> parodontite, <strong>le</strong>s mo<strong>la</strong>ires et prémo<strong>la</strong>iresinférieures <strong>de</strong> <strong>la</strong> patiente avaient été extraites il y a trenteans environ; à <strong>la</strong> même époque, <strong>le</strong>s <strong>de</strong>nts antérieures du maxil<strong>la</strong>iresupérieur avaient été restaurées par <strong>de</strong>s couronnes unitaires.Depuis 15 ans, <strong>la</strong> patiente porte une prothèse hybri<strong>de</strong><strong>dans</strong> <strong>le</strong> maxil<strong>la</strong>ire inférieur, ancrée par <strong>de</strong>s té<strong>le</strong>scopes sur quatre<strong>de</strong>nts piliers antérieures.Status cliniqueExamen extraoral<strong>La</strong> patiente présente un profil droit avec une légère proéminence<strong>de</strong> <strong>la</strong> mandibu<strong>le</strong>. <strong>La</strong> pointe du nez et en particulier <strong>le</strong>philtrum <strong>de</strong> <strong>la</strong> lèvre supérieure sont légèrement déviés vers <strong>la</strong>droite. Le tonus <strong>de</strong> <strong>la</strong> muscu<strong>la</strong>ture périora<strong>le</strong> est plus marquédu côté gauche. Le trajet <strong>de</strong> <strong>la</strong> ligne du sourire (Tjan et coll.1984) est un élément gênant, du fait qu’el<strong>le</strong> expose <strong>le</strong>s col<strong>le</strong>ts<strong>de</strong>ntaires et <strong>le</strong>s espaces inter<strong>de</strong>ntaires sombres en raison <strong>de</strong>l’absence <strong>de</strong>s papil<strong>le</strong>s (fig. 1).Examen intraoralAu début du traitement, l’hygiène bucco<strong>de</strong>ntaire <strong>de</strong> <strong>la</strong> patienteest insuffisante (indice <strong>de</strong> p<strong>la</strong>que 45%; O’Leary et coll. 1972;indice <strong>de</strong> saignement sulcu<strong>la</strong>ire 49%; Müh<strong>le</strong>mann & Son 1971),avec en revanche peu <strong>de</strong> dépôts <strong>de</strong> tartre.Dans <strong>le</strong> maxil<strong>la</strong>ire inférieur, <strong>le</strong>s quatre <strong>de</strong>nts piliers (43, 41,31 et 32) sont recouvertes <strong>de</strong> couronnes té<strong>le</strong>scopiques unitairespour l’ancrage <strong>de</strong> <strong>la</strong> prothèse hybri<strong>de</strong>. <strong>La</strong> 43 présente une cariesecondaire <strong>dans</strong> <strong>la</strong> région lingua<strong>le</strong> du bord <strong>de</strong> <strong>la</strong> couronne té<strong>le</strong>scopique,<strong>de</strong>s profon<strong>de</strong>urs <strong>de</strong> sondage <strong>de</strong> 4 mm, ainsi qu’unemobilité <strong>de</strong> <strong>de</strong>gré 2 (Müh<strong>le</strong>mann 1951 et 1974). Les 43 et 32 neréagissent pas au test <strong>de</strong> vitalité par <strong>la</strong> neige carbonique. Lerelief <strong>de</strong>s crêtes alvéo<strong>la</strong>ires est p<strong>la</strong>t, avec une atrophie marquée<strong>de</strong>s vestibu<strong>le</strong>s.Le maxil<strong>la</strong>ire supérieur comprend une arca<strong>de</strong> <strong>de</strong>ntaire complète<strong>de</strong> <strong>la</strong> 17 à <strong>la</strong> 26. Les profon<strong>de</strong>urs au sondage ne dépassentpas 5 mm. Dans <strong>la</strong> région <strong>de</strong>s <strong>de</strong>nts antérieures, on observeune mobilité atteignant <strong>le</strong> <strong>de</strong>gré 3 par endroits. A l’exception<strong>de</strong> <strong>la</strong> 13, toutes <strong>le</strong>s <strong>de</strong>nts réagissent positivement au test <strong>de</strong>vitalité par <strong>la</strong> neige carbonique (fig. 2).Status radiologiqueLe status par radiographies apica<strong>le</strong>s montre une perte osseusehorizonta<strong>le</strong> modérée, avec <strong>de</strong>s pertes osseuses vertica<strong>le</strong>s plusprofon<strong>de</strong>s, localisées sur <strong>le</strong>s 12 et 11. Des radiotransparencespériapica<strong>le</strong>s sont visib<strong>le</strong>s sur <strong>le</strong>s 43 et 31 et du côté distal <strong>de</strong><strong>la</strong> 23, au niveau du col<strong>le</strong>t <strong>de</strong> <strong>la</strong> <strong>de</strong>nt. Les 43 et 32 présentent<strong>de</strong>s obturations endodontiques inhomogènes et incomplètes,et <strong>de</strong> plus un tenon radicu<strong>la</strong>ire <strong>de</strong> dimensions importantes sur<strong>la</strong> 43 (fig. 3).Anamnèse médica<strong>le</strong> et <strong>de</strong>ntaireFig. 1Situation initia<strong>le</strong>, vue extraora<strong>le</strong>.670 Rev Mens Suisse Odontostomatol Vol. 121 7/8/2011
<strong>La</strong> <strong>zircone</strong> <strong>dans</strong> <strong>le</strong> <strong>domaine</strong> <strong>de</strong> <strong>la</strong> prothèse amovib<strong>le</strong> Pratique quotidienne et formation complémentaire– Résorption <strong>de</strong> <strong>la</strong> crête alvéo<strong>la</strong>ire <strong>de</strong> C<strong>la</strong>sse V <strong>dans</strong> <strong>le</strong> maxil<strong>la</strong>ireinférieur (Cawood & Howell 1988).Pronostic <strong>dans</strong> <strong>le</strong> maxil<strong>la</strong>ire inférieurEn raison <strong>de</strong> <strong>de</strong>structions jusque <strong>dans</strong> <strong>la</strong> région <strong>de</strong>s racines, <strong>le</strong>s43 et 32 ne peuvent plus être conservées. Il serait en revanchepossib<strong>le</strong> <strong>de</strong> conserver <strong>le</strong>s 41 et 31, malgré <strong>le</strong>ur position en protrusion.Or <strong>la</strong> patiente souhaite explicitement une reconstructionamovib<strong>le</strong> ancrée uniquement sur <strong>de</strong>s imp<strong>la</strong>nts.P<strong>la</strong>n <strong>de</strong> traitementFig. 2Evaluation <strong>de</strong> <strong>la</strong> situation prothétique existante<strong>La</strong> prothèse hybri<strong>de</strong> sur té<strong>le</strong>scopes <strong>dans</strong> <strong>le</strong> maxil<strong>la</strong>ire inférieurse caractérise par une adaptation insuffisante <strong>de</strong> <strong>la</strong> base, <strong>de</strong>ssel<strong>le</strong>s prothétiques raccourcies ainsi que par <strong>de</strong>s abrasionsmarquées <strong>de</strong>s <strong>de</strong>nts prothétiques. Sur <strong>le</strong>s couronnes té<strong>le</strong>scopiquesprimaires, on observe une adaptation margina<strong>le</strong> généra<strong>le</strong>mentinadéquate. Les restaurations prothétiques fixes <strong>dans</strong><strong>la</strong> région <strong>de</strong>s <strong>de</strong>nts antérieures du maxil<strong>la</strong>ire supérieur ne sontesthétiquement plus acceptab<strong>le</strong>s pour <strong>la</strong> patiente, en raison <strong>de</strong>porosités, <strong>de</strong> bords marginaux mal adaptés et <strong>de</strong> l’exposition<strong>de</strong> <strong>de</strong>ntine radicu<strong>la</strong>ire. Compte tenu <strong>de</strong>s désirs <strong>de</strong> <strong>la</strong> patiente,<strong>la</strong> priorité est attribuée à <strong>la</strong> nouvel<strong>le</strong> réhabilitation du maxil<strong>la</strong>ireinférieur, suivie, <strong>dans</strong> un <strong>de</strong>uxième temps, par cel<strong>le</strong> dumaxil<strong>la</strong>ire supérieur.DiagnosticSituation initia<strong>le</strong>, vue intra-ora<strong>le</strong>.Compte tenu <strong>de</strong> <strong>la</strong> perte d’attache et <strong>de</strong>s paramètres cliniques,<strong>le</strong> diagnostic d’une parodontite chronique généralisée est posé(Armitage 1999). Les autres diagnostics sont <strong>le</strong>s suivants:– Abcès parodontal sur <strong>le</strong>s 43 et 31;– Carie profon<strong>de</strong> sur <strong>la</strong> 43;– Granulome externe <strong>dans</strong> <strong>la</strong> région disto-cervica<strong>le</strong> <strong>de</strong> <strong>la</strong> 23;Le p<strong>la</strong>n <strong>de</strong> traitement prévoit <strong>la</strong> réalisation d’une nouvel<strong>le</strong> prothèsehybri<strong>de</strong>, ancrée sur quatre imp<strong>la</strong>nts <strong>dans</strong> <strong>le</strong>s régions <strong>de</strong>scanines et <strong>de</strong>s mo<strong>la</strong>ires. Deux barres séparées <strong>dans</strong> <strong>le</strong>s régions<strong>la</strong>téra<strong>le</strong>s seront <strong>de</strong>stinées à assurer une assise <strong>de</strong> <strong>la</strong> prothèse sansappui muqueux. Afin d’évaluer <strong>le</strong>s possibilités et <strong>le</strong>s limites d’unereconstruction monolithique en <strong>zircone</strong>, il est prévu <strong>de</strong> réaliser<strong>la</strong> totalité <strong>de</strong>s éléments prothétiques entièrement en céramique.Etapes du traitementTraitement préprothétique et pose <strong>de</strong>s imp<strong>la</strong>nts<strong>La</strong> patiente bénéficie tout d’abord d’un nettoyage professionnel<strong>de</strong>s <strong>de</strong>nts du maxil<strong>la</strong>ire supérieur et d’une instruction d’hygiènebucco<strong>de</strong>ntaire. Dans <strong>le</strong> maxil<strong>la</strong>ire inférieur, <strong>le</strong>s quatre<strong>de</strong>nts restantes sont extraites, avant <strong>la</strong> mise en bouche d’uneprothèse tota<strong>le</strong> immédiate confectionnée en se fondant sur <strong>le</strong>sdimensions vertica<strong>le</strong>s et horizonta<strong>le</strong>s <strong>de</strong> l’ancienne prothèsehybri<strong>de</strong>. Après <strong>le</strong> diagnostic et <strong>la</strong> p<strong>la</strong>nification spécifique, onprocè<strong>de</strong> à l’insertion <strong>de</strong> quatre imp<strong>la</strong>nts: un imp<strong>la</strong>nt <strong>dans</strong> <strong>la</strong>région <strong>de</strong> <strong>la</strong> 46, aux dimensions 3,538 mm, <strong>de</strong>ux imp<strong>la</strong>nts <strong>de</strong>4,3313 mm <strong>dans</strong> <strong>le</strong>s régions <strong>de</strong>s 44 et 33 et un imp<strong>la</strong>nt <strong>de</strong>3,5310 mm <strong>dans</strong> <strong>la</strong> région <strong>de</strong> <strong>la</strong> 36 (NobelRep<strong>la</strong>ce Tapered;Nobel Biocare AB, Göteborg, Suè<strong>de</strong>). Trois mois après l’expositiontransgingiva<strong>le</strong> <strong>de</strong>s imp<strong>la</strong>nts, <strong>la</strong> situation ora<strong>le</strong> est stab<strong>le</strong>et exempte d’inf<strong>la</strong>mmation (fig. 4a et 4b). Pour <strong>la</strong> stabilisation<strong>de</strong> <strong>la</strong> prothèse provisoire, <strong>de</strong> même que pour <strong>la</strong> simplification<strong>de</strong>s étapes prothétiques ultérieures, on procè<strong>de</strong> à <strong>la</strong> pose extemporanéed’ancrages amovib<strong>le</strong>s par <strong>de</strong>s abutments Locator ® (ZestAnchors, Escondido, CA, USA). <strong>La</strong> patiente s’est adaptée sansFig. 3Situation initia<strong>le</strong>, status radiologique.Rev Mens Suisse Odontostomatol Vol. 121 7/8/2011 671
Pratique quotidienne et formation complémentaire <strong>La</strong> <strong>zircone</strong> <strong>dans</strong> <strong>le</strong> <strong>domaine</strong> <strong>de</strong> <strong>la</strong> prothèse amovib<strong>le</strong>Fig. 4a Maxil<strong>la</strong>ire inférieur après insertion <strong>de</strong> quatre imp<strong>la</strong>nts <strong>dans</strong> <strong>le</strong>s régions<strong>de</strong>s canines et <strong>de</strong>s mo<strong>la</strong>ires.Fig. 5 Solidarisation exempte <strong>de</strong> tensions <strong>de</strong>s transferts sur <strong>le</strong>s imp<strong>la</strong>ntsavant <strong>la</strong> prise <strong>de</strong> l’empreinte <strong>de</strong> situation.problème à <strong>la</strong> prothèse provisoire qui <strong>de</strong>vra être remp<strong>la</strong>cée parune prothèse définitive six mois après l’extraction <strong>de</strong>s <strong>de</strong>ntsmandibu<strong>la</strong>ires restantes et <strong>la</strong> pose <strong>de</strong>s imp<strong>la</strong>nts.Prise <strong>de</strong>s empreintes et montage <strong>de</strong>s modè<strong>le</strong>s en articu<strong>la</strong>teurEn vue <strong>de</strong> l’empreinte définitive par un matériau polyéther(Impregum; 3M ESPE, Seefeld, Al<strong>le</strong>magne) <strong>dans</strong> un porteempreinteindividuel, <strong>le</strong>s transferts sont solidarisés sans tensionà l’ai<strong>de</strong> <strong>de</strong> fil <strong>de</strong>ntaire enrobé <strong>de</strong> résine (Dura<strong>la</strong>y ® ; RelianceDental Mfg. Co., Worth, IL, Etats-Unis) (fig. 5 et 6). Sur <strong>le</strong>smaîtres modè<strong>le</strong>s en plâtre extra dur, <strong>le</strong> <strong>la</strong>boratoire confectionne<strong>de</strong>s masques gingivaux amovib<strong>le</strong>s en silicone. Le contrô<strong>le</strong> <strong>de</strong><strong>la</strong> précision du maître modè<strong>le</strong> est réalisé à l’ai<strong>de</strong> d’une clé (stent)<strong>de</strong> vérification en plâtre (fig. 7). Les modè<strong>le</strong>s sont ensuite montésen articu<strong>la</strong>teur (SAM ® 2P; SAM Präzisionstechnik GmbH,Gauting, Al<strong>le</strong>magne) par arc facial et enregistrement <strong>de</strong>s re<strong>la</strong>tionsintermaxil<strong>la</strong>ires et <strong>de</strong> <strong>la</strong> dimension vertica<strong>le</strong> d’occlusion.Montage <strong>de</strong>s <strong>de</strong>nts prothétiquesLe <strong>la</strong>boratoire procè<strong>de</strong> alors au montage <strong>de</strong>s <strong>de</strong>nts prothétiques<strong>dans</strong> <strong>le</strong> maxil<strong>la</strong>ire inférieur en utilisant <strong>de</strong>s <strong>de</strong>nts anatomiquesen polyuréthane (Frame A+B; <strong>Zirkonzahn</strong> ® GmbH), <strong>le</strong> montages’inspirant <strong>de</strong> <strong>la</strong> prothèse immédiate. Les <strong>de</strong>nts en polyuréthanese basent sur <strong>de</strong>s duplicata <strong>de</strong> <strong>de</strong>nts naturel<strong>le</strong>s conservés<strong>dans</strong> une bibliothèque du fabricant. Un essai en bouche <strong>de</strong> <strong>la</strong>Fig. 6 Empreinte définitive par matériau polyéther <strong>dans</strong> un porte-empreinteindividuel.patiente (fig. 8) sert au contrô<strong>le</strong> global. Le montage, vérifié etadapté, est ensuite dupliqué en silicone au <strong>la</strong>boratoire et l’ensemb<strong>le</strong>est alors coulé en polyuréthane (Frame A+B). A l’ai<strong>de</strong><strong>de</strong> mésostructures provisoires, il est possib<strong>le</strong> <strong>de</strong> repositionner<strong>de</strong> manière précise <strong>le</strong> duplicata, tant sur <strong>le</strong> maître modè<strong>le</strong> qu’enbouche. L’essai clinique <strong>de</strong> <strong>la</strong> prothèse en polyuréthane estextraordinairement important: tant l’occlusion que l’adapta-Fig. 4bOPT <strong>de</strong> <strong>la</strong> situation imp<strong>la</strong>ntologique avant <strong>le</strong> traitement prothétique.672 Rev Mens Suisse Odontostomatol Vol. 121 7/8/2011
<strong>La</strong> <strong>zircone</strong> <strong>dans</strong> <strong>le</strong> <strong>domaine</strong> <strong>de</strong> <strong>la</strong> prothèse amovib<strong>le</strong> Pratique quotidienne et formation complémentaireFig. 7 Vérification en bouche <strong>de</strong> <strong>la</strong> situation sur <strong>le</strong> maître modè<strong>le</strong> par un gabarit<strong>de</strong> contrô<strong>le</strong> (verification stent) en plâtre.Fig. 10 Fraisage en parallè<strong>le</strong> du profil <strong>de</strong> <strong>la</strong> barre sur <strong>la</strong> base <strong>de</strong> <strong>la</strong> prothèseen polyuréthane.Fig. 8Contrô<strong>le</strong> du montage <strong>de</strong>s <strong>de</strong>nts sur cire.Fig. 11 Les modè<strong>le</strong>s terminés <strong>de</strong>s <strong>de</strong>ux barres après montage <strong>de</strong>s partiesmâ<strong>le</strong>s <strong>de</strong>s glissières avant <strong>le</strong> fraisage par copiage.Fig. 9 Contrô<strong>le</strong> <strong>de</strong>s extensions <strong>de</strong> <strong>la</strong> base et <strong>de</strong> l’occlusion <strong>de</strong> <strong>la</strong> prothèseen polyuréthane.tion <strong>de</strong> <strong>la</strong> base sont soigneusement évaluées sur <strong>le</strong> patient et,<strong>le</strong> cas échéant, modifiées avant <strong>le</strong> fraisage définitif du travailsur <strong>zircone</strong> (fig. 9).Fabrication <strong>de</strong>s barres en <strong>zircone</strong>Le <strong>la</strong>boratoire réalise une clé en silicone <strong>de</strong> <strong>la</strong> prothèse en polyuréthane,<strong>la</strong>quel<strong>le</strong> est ensuite fixée par <strong>de</strong>s analogues <strong>de</strong> <strong>la</strong>boratoiresur un soc<strong>le</strong> en plâtre en vue du fraisage. Deux modè<strong>le</strong>s<strong>de</strong>s barres sont confectionnés par fraisage parallè<strong>le</strong> à partir <strong>de</strong><strong>la</strong> prothèse en polyuréthane (fig. 10). Durant <strong>le</strong> fraisage, <strong>le</strong>sclés en silicone permettent d’évaluer <strong>le</strong>s dimensions et <strong>le</strong>spositions correctes, ainsi que <strong>la</strong> p<strong>la</strong>ce disponib<strong>le</strong> pour <strong>la</strong> suprastructure.Pour finir, <strong>de</strong>s parties mâ<strong>le</strong>s <strong>de</strong> glissière en résine(Vario-Soft 3 zircon mini sv; Bre<strong>de</strong>nt GmbH & Co. KG, Sen<strong>de</strong>n,Al<strong>le</strong>magne) sont montées sur <strong>le</strong>s extrémités dista<strong>le</strong>s et mésia<strong>le</strong>s<strong>de</strong>s modè<strong>le</strong>s <strong>de</strong>s barres (fig. 11).Les modè<strong>le</strong>s <strong>de</strong>s barres, ainsi que <strong>le</strong> bloc <strong>de</strong> <strong>zircone</strong> (PrettauZirkon; <strong>Zirkonzahn</strong> ® GmbH) sé<strong>le</strong>ctionné sont ensuite collés sur<strong>le</strong>s disques <strong>de</strong> montage (fig. 12), <strong>le</strong>squels sont à <strong>le</strong>ur tour fixés<strong>dans</strong> <strong>la</strong> machine <strong>de</strong> fraisage par copiage (Zirkograph; <strong>Zirkonzahn</strong>® GmbH). Le Zirkograph permet <strong>de</strong> réaliser par fraisage <strong>de</strong>copiage manuel une ébauche à l’état non fritté (un «vert») àune échel<strong>le</strong> <strong>de</strong> grossissement <strong>de</strong> 1,25. Le facteur <strong>de</strong> grossissementest <strong>de</strong>stiné à compenser <strong>le</strong> rétrécissement <strong>de</strong>s pièces en<strong>zircone</strong> lors du frittage. Le fraisage se fait par étapes, en commençantpar <strong>de</strong>s fraises grossières, puis <strong>de</strong>s fraises plus fines,guidées par <strong>de</strong>s palpeurs <strong>de</strong> copiage correspondants. Le fraisagecomprend l’ensemb<strong>le</strong> <strong>de</strong>s éléments <strong>de</strong>s barres, y compris <strong>le</strong>sinterfaces sur <strong>le</strong>s imp<strong>la</strong>nts, représentées par <strong>le</strong>s analogues, et<strong>le</strong>s parties mâ<strong>le</strong>s <strong>de</strong>s glissières. Il en résulte une pièce brute <strong>de</strong>chaque barre, homogène et entièrement en <strong>zircone</strong>. A ce sta<strong>de</strong>,il est possib<strong>le</strong> <strong>de</strong> modifier <strong>la</strong> chromie <strong>de</strong>s pièces, selon <strong>le</strong>s besoins,en <strong>le</strong>s trempant <strong>dans</strong> <strong>de</strong>s solutions aqueuses <strong>de</strong> colorants(Colour Liquids; <strong>Zirkonzahn</strong> ® GmbH). L’étape suivante consisteà éliminer <strong>de</strong> l’humidité à l’ai<strong>de</strong> <strong>de</strong> lumière infrarouge (40 min),avant <strong>de</strong> passer à <strong>la</strong> cuisson <strong>de</strong> frittage (8 h à 1600 °C, Keramikofen[four à céramique] 1500; <strong>Zirkonzahn</strong> ® GmbH). Après uneRev Mens Suisse Odontostomatol Vol. 121 7/8/2011 673
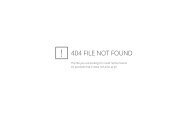
Pratique quotidienne et formation complémentaire <strong>La</strong> <strong>zircone</strong> <strong>dans</strong> <strong>le</strong> <strong>domaine</strong> <strong>de</strong> <strong>la</strong> prothèse amovib<strong>le</strong>Fig. 20bA noter <strong>le</strong> rendu <strong>de</strong>s détails <strong>de</strong> <strong>la</strong> morphologie.Fig. 21b Vue <strong>de</strong> détail <strong>de</strong> <strong>la</strong> Fig. 21a: à noter <strong>le</strong>s surfaces parfaitement lisses,garantissant un entretien hygiénique efficace.Fig. 21a Des paries femel<strong>le</strong>s à friction en nylon sont montées <strong>dans</strong> l’intrados<strong>de</strong> <strong>la</strong> prothèse.Mise en bouche et soins <strong>de</strong> suiviLes barres sont mises en p<strong>la</strong>ce et vissées sur <strong>le</strong>s piliers imp<strong>la</strong>ntairespar <strong>de</strong>s vis d’abutments en titane avec un coup<strong>le</strong> <strong>de</strong>serrage <strong>de</strong> 25 Ncm –1 (Abutment Screw TorqTite ® ; Nobel BiocareAB). Les radiographies <strong>de</strong> contrô<strong>le</strong> confirment <strong>le</strong> positionnementcorrect <strong>de</strong>s barres (fig. 22). Dans un premier temps,<strong>le</strong>s cavités occlusa<strong>le</strong>s d’accès aux vis sont provisoirement ferméespar <strong>de</strong>s pel<strong>le</strong>ts en mousse et du Fermit (Fermit ® ; Ivoc<strong>la</strong>rFig. 23a Insertion <strong>de</strong>s barres en <strong>zircone</strong> et vissage avec un coup<strong>le</strong> <strong>de</strong>25 Ncm –1 . Les pertuis d’accès aux vis ont été obturés par du composite.Viva<strong>de</strong>nt AG, Schaan, Liechtenstein). Des contrô<strong>le</strong>s sont réalisésaprès 24 heures et une semaine. Lors <strong>de</strong> <strong>la</strong> <strong>de</strong>uxièmeséance <strong>de</strong> suivi, on procè<strong>de</strong> au contrô<strong>le</strong> <strong>de</strong> l’assise <strong>de</strong>s vis. Lescavités d’accès sont alors définitivement obturées par <strong>de</strong>s pel<strong>le</strong>tsen mousse et du composite (Tetric EvoCeram ® ; Ivoc<strong>la</strong>rViva<strong>de</strong>nt AG) (fig. 23a, 23b, 23c et 23d). Enfin, <strong>la</strong> patientebénéficie d’une instruction concernant <strong>le</strong> maniement <strong>de</strong> <strong>la</strong>prothèse et l’hygiène spécifique nécessaire; on attire son atten-Fig. 22Contrô<strong>le</strong> radiologique à <strong>la</strong> fin du traitement.676 Rev Mens Suisse Odontostomatol Vol. 121 7/8/2011
<strong>La</strong> <strong>zircone</strong> <strong>dans</strong> <strong>le</strong> <strong>domaine</strong> <strong>de</strong> <strong>la</strong> prothèse amovib<strong>le</strong> Pratique quotidienne et formation complémentaireFig. 23b<strong>La</strong> prothèse en <strong>zircone</strong> après <strong>la</strong> mise en bouche, vue occlusa<strong>le</strong>.Fig. 23c <strong>La</strong> prothèse en <strong>zircone</strong> après <strong>la</strong> mise en bouche, vue fronta<strong>le</strong>. Fig. 23d <strong>La</strong> patiente, souriante à <strong>la</strong> fin du traitement couronné <strong>de</strong> succès.tion sur l’importance d’un suivi régulier chez l’hygiéniste<strong>de</strong>ntaire. Lors du contrô<strong>le</strong> <strong>de</strong> <strong>la</strong> prothèse hybri<strong>de</strong> 18 mois après<strong>la</strong> mise en bouche, <strong>la</strong> reconstruction fonctionne à l’entièresatisfaction <strong>de</strong> <strong>la</strong> patiente, sans qu’aucune intervention prothétiquen’ait été nécessaire.DiscussionLe présent travail a montré <strong>la</strong> réhabilitation réussie d’une patienteâgée <strong>de</strong> 70 ans par une prothèse hybri<strong>de</strong> du maxil<strong>la</strong>ireinférieur, ancrée sur quatre imp<strong>la</strong>nts, pour <strong>la</strong>quel<strong>le</strong> tant <strong>le</strong>sparties primaires que secondaires ont été fabriquées entièrementen <strong>zircone</strong>. Du fait que ces éléments fraisés sont <strong>de</strong>s structuresmonolithiques (Karl & Bauernschmidt 2010), <strong>la</strong> stabilitéà long terme <strong>de</strong> <strong>la</strong> reconstruction est jugée favorab<strong>le</strong>. Le revêtementcosmétique <strong>de</strong> <strong>la</strong> base prothétique sert uniquement àl’individualisation <strong>de</strong>s cou<strong>le</strong>urs. Pour <strong>le</strong>s reconstructionsconventionnel<strong>le</strong>s sur base d’armatures coulées, <strong>de</strong>s donnéescliniques validées à long terme sont disponib<strong>le</strong>s, alors que pource procédé <strong>de</strong> fraisage par copiage d’une part et pour <strong>la</strong> fabrication<strong>de</strong>s parties primaires et secondaires en céramiqued’autre part, <strong>de</strong>s résultats issus d’évaluations cliniques fontencore défaut pour l’instant. Une récente revue <strong>de</strong> <strong>la</strong> littératurepubliée par Har<strong>de</strong>r & Kern (2009) a montré que <strong>de</strong>s reconstructionsconfectionnées par <strong>de</strong>s procédés conventionnels ne sontpas en reste par rapport aux travaux réalisés par CAD/CAM.En tant qu’avantages <strong>de</strong> cette nouvel<strong>le</strong> métho<strong>de</strong> en prothèseamovib<strong>le</strong>, différents auteurs ont particulièrement évoqué <strong>la</strong>biocompatibilité, l’absence <strong>de</strong> métal, l’hygiène facilitée enraison <strong>de</strong>s surfaces céramiques lisses, mais éga<strong>le</strong>ment <strong>le</strong>s possibilités<strong>de</strong> <strong>la</strong> fabrication par CAD/CAM (Scarano et coll. 2004,Rimondini et coll. 2002). <strong>La</strong> technologie CAD/CAM permetnon seu<strong>le</strong>ment une réduction <strong>de</strong>s coûts, à qualité éga<strong>le</strong> <strong>de</strong>smatériaux, mais éga<strong>le</strong>ment une précision d’adaptation normalisée<strong>de</strong> haut niveau (Al-Fadda et coll. 2007, Ortorp et coll.2003). Par contre, <strong>de</strong> tel<strong>le</strong>s reconstructions ne peuvent être utiliséesque <strong>dans</strong> <strong>de</strong>s cas pour <strong>le</strong>squels un rebasage ou <strong>de</strong>s réparations<strong>de</strong> <strong>la</strong> base prothétique ne sont pas prévus. Dernier aspect,on ignore encore <strong>dans</strong> quel<strong>le</strong> mesure <strong>le</strong>s <strong>de</strong>nts prothétiquesen <strong>zircone</strong> risquent d’avoir <strong>de</strong>s répercussions négatives sur <strong>le</strong>s<strong>de</strong>nts <strong>de</strong> l’arca<strong>de</strong> opposée (Steger & Trejo Cabal<strong>le</strong>ro 2010).Le procédé clinique ne se distingue pas fondamenta<strong>le</strong>ment<strong>de</strong> celui <strong>de</strong> <strong>la</strong> réalisation d’une prothèse hybri<strong>de</strong> conventionnel<strong>le</strong>sur une armature métallique. A noter toutefois que l’essaien bouche <strong>de</strong> <strong>la</strong> prothèse en polyuréthane revêt une importanceparticulière, car il faut impérativement éviter toute modification(par <strong>de</strong>s instruments rotatifs) <strong>de</strong> <strong>la</strong> prothèse définitive en<strong>zircone</strong> pour prévenir <strong>le</strong> risque <strong>de</strong> fracture. En fait, <strong>de</strong>s correctionsultérieures ne sont possib<strong>le</strong>s que sous toutes réserves.Bien que <strong>le</strong> système présenté comprenne <strong>la</strong> possibilité <strong>de</strong> fabricationpar CAD/CAM, <strong>la</strong> technique du fraisage par copiagemanuel offre une liberté maxima<strong>le</strong> au technicien <strong>dans</strong> <strong>la</strong> réalisationd’éléments prothétiques en <strong>zircone</strong>, tant sur <strong>de</strong>s <strong>de</strong>ntsnaturel<strong>le</strong>s que sur <strong>de</strong>s imp<strong>la</strong>nts.Le résultat esthétique du travail illustré est jugé fort réussi.Pour <strong>le</strong>s régions esthétiquement délicates, il est recommandéRev Mens Suisse Odontostomatol Vol. 121 7/8/2011 677
Pratique quotidienne et formation complémentaire <strong>La</strong> <strong>zircone</strong> <strong>dans</strong> <strong>le</strong> <strong>domaine</strong> <strong>de</strong> <strong>la</strong> prothèse amovib<strong>le</strong><strong>de</strong> réduire <strong>la</strong> pièce fraisée en <strong>zircone</strong> à l’état brut (non fritté)<strong>dans</strong> <strong>le</strong>s zones vestibu<strong>la</strong>ires et, <strong>le</strong> cas échéant, au niveau <strong>de</strong>sbords incisifs. Les zones ainsi réduites sont ensuite reconstruitespar un revêtement cosmétique en vitrocéramique, <strong>le</strong> résultatétant alors une construction biphasique.Par cette illustration d’un cas clinique, <strong>le</strong>s auteurs ont démontréque <strong>la</strong> <strong>zircone</strong>, céramique à hautes performances, convientéga<strong>le</strong>ment pour <strong>la</strong> fabrication <strong>de</strong> parties primaires et secondairesen prothèse amovib<strong>le</strong> hybri<strong>de</strong>. Concernant <strong>la</strong> pérennité<strong>de</strong> tel<strong>le</strong>s reconstructions, il y a lieu <strong>de</strong> tenir compte <strong>de</strong> <strong>de</strong>uxaspects: d’une part <strong>la</strong> stabilité à long terme et d’autre part <strong>le</strong>comportement <strong>de</strong>s surfaces. Avant d’envisager <strong>de</strong>s utilisations<strong>de</strong> cette métho<strong>de</strong> en pratique, il faudra attendre <strong>de</strong>s étu<strong>de</strong>scliniques contrôlées concernant ces <strong>de</strong>ux paramètres. Nonobstantcette restriction, <strong>la</strong> possibilité d’employer <strong>la</strong> <strong>zircone</strong> entant qu’alternative au métal et aux résines paraît être une solutionattrayante <strong>dans</strong> certains cas individuels.RemerciementsLes auteurs remercient M. Andreas Lorenzon, maître technicien<strong>de</strong>ntiste,Zurich, pour son assistance lors <strong>de</strong> <strong>la</strong> p<strong>la</strong>nification etdu diagnostic. De même, ils expriment <strong>le</strong>ur gratitu<strong>de</strong> à M. GeorgWalcher, maître technicien-<strong>de</strong>ntiste, Bruneck, Italie, pour sonengagement et ses compétences lors <strong>de</strong> <strong>la</strong> réalisation <strong>de</strong>s travaux.Sans <strong>le</strong>s contributions remarquab<strong>le</strong>s <strong>de</strong> ces <strong>de</strong>ux spécialistes,il n’aurait pas été possib<strong>le</strong> <strong>de</strong> mener à bien ce projet.Bibliographie voir texte al<strong>le</strong>mand, page 668.678 Rev Mens Suisse Odontostomatol Vol. 121 7/8/2011