
You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
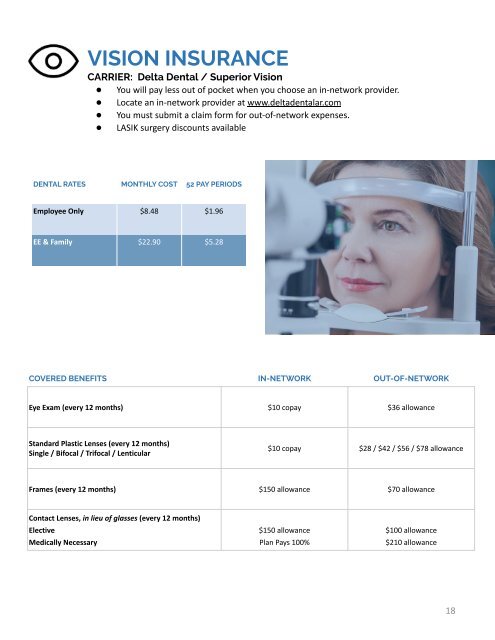
VISION INSURANCE<br />
CARRIER: Delta Dental / Superior Vision<br />
● You will pay less out of pocket when you choose an in-network provider.<br />
● Locate an in-network provider at www.deltadentalar.com<br />
● You must submit a claim form for out-of-network expenses.<br />
● LASIK surgery discounts available<br />
DENTAL RATES MONTHLY COST 52 PAY PERIODS<br />
Employee Only $8.48 $1.96<br />
EE & Family $22.90 $5.28<br />
COVERED BENEFITS IN-NETWORK OUT-OF-NETWORK<br />
Eye Exam (every 12 months) $10 copay $36 allowance<br />
Standard Plastic Lenses (every 12 months)<br />
Single / Bifocal / Trifocal / Lenticular<br />
$10 copay $28 / $42 / $56 / $78 allowance<br />
Frames (every 12 months) $150 allowance $70 allowance<br />
Contact Lenses, in lieu of glasses (every 12 months)<br />
Elective<br />
Medically Necessary<br />
$150 allowance<br />
Plan Pays 100%<br />
$100 allowance<br />
$210 allowance<br />
18