
You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
24<br />
heart rhythm was significant in group II<br />
patients and in 1/3 of them heart rate was<br />
47-53.<br />
Sinus, atrial and ventricular<br />
extrasystoles were found rarely and<br />
equally in both groups. However, only<br />
in group II we had interatrial,<br />
atrioventricular and interventricular<br />
damages of conduction.<br />
Supraventricular paroxysmal<br />
tachycardia was found only in 2 patients<br />
who had pulse rate of 133-155. We had<br />
,fdidsf rfhlbjkjubf<br />
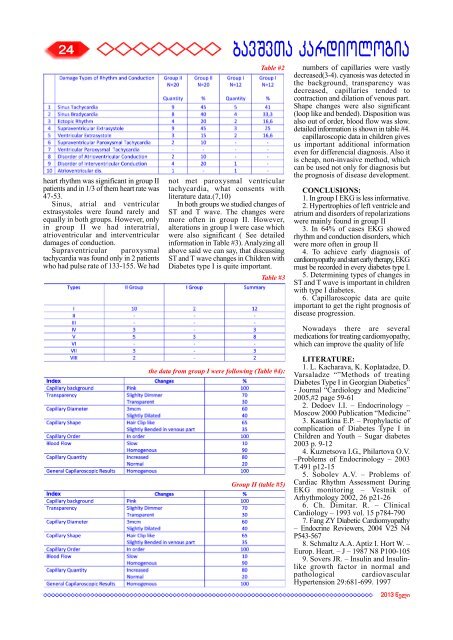
Table #2<br />
not met paroxysmal ventricular<br />
tachycardia, what consents with<br />
literature data.(7,10)<br />
In both groups we studied changes of<br />
ST and T wave. The changes were<br />
more often in group II. However,<br />
alterations in group I were case which<br />
were also significant ( See detailed<br />
<strong>info</strong>rmation in Table #3). Analyzing all<br />
above said we can say, that discussing<br />
ST and T wave changes in Children with<br />
Diabetes type I is quite important.<br />
Table #3<br />
the data from group I were following (Table #4):<br />
Group II (table #5)<br />
numbers of capillaries were vastly<br />
decreased(3-4). cyanosis was detected in<br />
the background, transparency was<br />
decreased, capillaries tended to<br />
contraction and dilation of venous part.<br />
Shape changes were also significant<br />
(loop like and bended). Disposition was<br />
also out of order, blood flow was slow.<br />
detailed <strong>info</strong>rmation is shown in table #4.<br />
capillaroscopic data in children gives<br />
us important additional <strong>info</strong>rmation<br />
even for differencial diagnosis. Also it<br />
is cheap, non-invasive method, which<br />
can be used not only for diagnosis but<br />
the prognosis of disease development.<br />
CONCLUSIONS:<br />
1. In group I EKG is less <strong>info</strong>rmative.<br />
2. Hypertrophies of left ventricle and<br />
atrium and disorders of repolarizations<br />
were mainly found in group II<br />
3. In 64% of cases EKG showed<br />
rhythm and conduction disorders, which<br />
were more often in group II<br />
4. To achieve early diagnosis of<br />
cardiomyopathy and start early therapy, EKG<br />
must be recorded in every diabetes type I.<br />
5. Determining types of changes in<br />
ST and T wave is important in children<br />
with type I diabetes.<br />
6. Capillaroscopic data are quite<br />
important to get the right prognosis of<br />
disease progression.<br />
Nowadays there are several<br />
medications for treating cardiomyopathy,<br />
which can improve the quality of life<br />
LITERATURE:<br />
1. L. Kacharava, K. Koplatadze, D.<br />
Varsaladze “”Methods of treating<br />
Diabetes Type I in Georgian Diabetics”<br />
- Journal “Cardiology and Medicine”<br />
2005,#2 page 59-61<br />
2. Dedoev I.I. – Endocrinology –<br />
Moscow 2000 Publication “Medicine”<br />
3. Kasatkina E.P. – Prophylactic of<br />
complication of Diabetes Type I in<br />
Children and Youth – Sugar diabetes<br />
2003 p. 9-12<br />
4. Kuznetsova I.G., Philartova O.V.<br />
–Problems of Endocrinology – 2003<br />
T.491 p12-15<br />
5. Sobolev A.V. – Problems of<br />
Cardiac Rhythm Assessment During<br />
EKG monitoring – Vestnik of<br />
Arhythmology 2002, 26 p21-26<br />
6. Ch. Dimitar. R. – Clinical<br />
Cardiology – 1993 vol. 15 p784-790<br />
7. Fang ZY Diabetic Cardiomyopathy<br />
– Endocrine Reviewers, 2004 V25 N4<br />
P543-567<br />
8. Schmaltz A.A. Aptiz I. Hort W. –<br />
Europ. Heart. – J – 1987 N8 P100-105<br />
9. Sovers JR. – Insulin and Insulinlike<br />
growth factor in normal and<br />
pathological cardiovascular<br />
Hypertension 29:681-699. 1997<br />
2013 weli