

APPENDICES FORMS Word Documents EI 5031 ATD Request EI ...
APPENDICES FORMS Word Documents EI 5031 ATD Request EI ...
APPENDICES FORMS Word Documents EI 5031 ATD Request EI ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
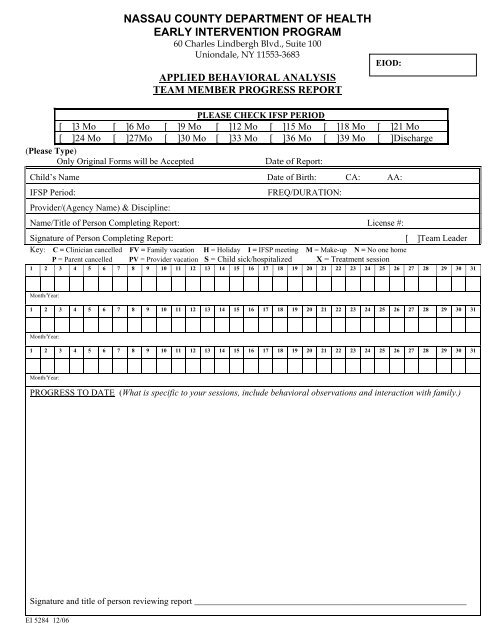
NASSAU COUNTY DEPARTMENT OF HEALTH<br />
EARLY INTERVENTION PROGRAM<br />
60 Charles Lindbergh Blvd., Suite 100<br />
Uniondale, NY 11553-3683<br />
APPLIED BEHAVIORAL ANALYSIS<br />
TEAM MEMBER PROGRESS REPORT<br />
<strong>EI</strong>OD:<br />
PLEASE CHECK IFSP PERIOD<br />
[ ]3 Mo [ ]6 Mo [ ]9 Mo [ ]12 Mo [ ]15 Mo [ ]18 Mo [ ]21 Mo<br />
[ ]24 Mo [ ]27Mo [ ]30 Mo [ ]33 Mo [ ]36 Mo [ ]39 Mo [ ]Discharge<br />
(Please Type)<br />
Only Original Forms will be Accepted Date of Report:<br />
Child’s Name Date of Birth: CA: AA:<br />
IFSP Period: FREQ/DURATION:<br />
Provider/(Agency Name) & Discipline:<br />
Name/Title of Person Completing Report: License #:<br />
Signature of Person Completing Report: [ ]Team Leader<br />
Key: C = Clinician cancelled FV = Family vacation H = Holiday I = IFSP meeting M = Make-up N = No one home<br />
P = Parent cancelled PV = Provider vacation S = Child sick/hospitalized X = Treatment session<br />
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31<br />
Month/Year:<br />
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31<br />
Month/Year:<br />
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31<br />
Month/Year:<br />
PROGRESS TO DATE (What is specific to your sessions, include behavioral observations and interaction with family.)<br />
Signature and title of person reviewing report _____________________________________________________________<br />
<strong>EI</strong> 5284 12/06