Salmonella Ovarian Abscess: A Case Report*
Salmonella Ovarian Abscess: A Case Report*
Salmonella Ovarian Abscess: A Case Report*

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Salmonella</strong> <strong>Ovarian</strong> <strong>Abscess</strong>: A <strong>Case</strong> <strong>Report*</strong><br />
Eileen G. Aniceto, M.D.,** Adrian C. Pena, M.D.,*** Adelia M. Quijano, M.D.**** and Charito<br />
Saludades, M.D. *****<br />
(*From the University of the East Ramon Magsaysay Memorial Medical Center (UERMMMC) University Hospital;<br />
**Chief Resident, Department of Medicine; ***Assistant Professor of Medicine and Chief, Section of Infectious<br />
Diseases, Department of Medicine; ****Consultant, Department of Obstetrics and Gynecology; *****Senior<br />
Resident, Department of Obstetrics and Gynecology)<br />
ABSTRACT<br />
<strong>Ovarian</strong> abscesses are rare conditions. <strong>Ovarian</strong> abscesses secondary to <strong>Salmonella</strong> spp. are even rarer entities.<br />
This is a report of a 23-year old primigravid who developed ovarian abscess, pelvic inflammatory disease (PID) and<br />
peri-appendicitis three weeks after an episode of typhoid fever. [Phil J Microbiol Infect Dis 1990; 19(2):68-71]<br />
Key words: ovarian abscess, salmonella infection, pelvic inflammatory disease<br />
INTRODUCTION<br />
<strong>Ovarian</strong> abscesses are rare conditions. <strong>Ovarian</strong> abscesses secondary to <strong>Salmonella</strong> spp.<br />
are even rarer entities. Localization of infection may occur at any site after salmonella bacteremia<br />
irrespective of the associated clinical syndrome. Although bacteremia can be assumed to develop<br />
in all patients with typhoid fever, localized infections actually occur only in 1% of cases.<br />
Localization of the infection in the ovaries occurs even less frequently. We report a case of a 23year<br />
old G1P0 (0070) primigravid who developed left ovarian abscess, PID and peri-appendicitis 3<br />
weeks after an episode of typhoid fever .<br />
<strong>Case</strong> History<br />
A 23-year old female, G1PO (0010) was admitted for the third time because of severe<br />
continuous hypogastric pains. of 2 days duration. She was first admitted to this center 25 days<br />
prior to admission because of a five day history of moderate to high grade fever, malaise and bifrontal<br />
headache. There were also severe crampy hypogastric pains followed by vaginal spotting<br />
noted 2 days after.<br />
On admission, physical examination revealed a febrile patient with essentially normal<br />
findings except that the uterus was enlarged to 8 weeks size, and the cervix was soft, closed, and<br />
non-tender with no adnexal masses. Work-up revealed WBC count of 4.8 x 10 9 /1 with a normal<br />
differential count; urinalysis showed 4-6 WBC/HPF; ultra sound examination showed a<br />
gestational sac with no fetal pole; Widal test showed positive titers at 1/320 for <strong>Salmonella</strong> D.<br />
Blood culture was positive for <strong>Salmonella</strong> typhi. Diagnosis then was typhoid fever, intrauterine<br />
pregnancy, blighted ovum 9-2/7 weeks. Patient was started on chloramphenicol at 3 grams per<br />
day. A dilatation and curettage was performed on the first hospital day. The patient was<br />
discharged asymptomatic after one week with instructions to continue chloramphenicol for 2<br />
weeks.<br />
Eight days prior to admission, the patient developed intermittent mild to moderate<br />
crampy hypogastric pains without associated fever. Internal examination then revealed slight<br />
tenderness at left adnexae. She was admitted with an impression of pelvic inflammatory disease<br />
(PID), rule out ectopic pregnancy. Work up showed a negative monoclonal pregnancy test and a<br />
culdocentesis showed only serosanguinous fluid. WBC and differential count showed 9 x 10 9 /L<br />
with 52% neutrophils, 47% lymphocytes and 1 % eosinophils. Penicillin G was given. The patient<br />
was discharged asymptomatic after 3 days of hospitalization.
Two days prior to admission, severe hypogastric pains developed. This was associated<br />
with nausea, vomiting, diarrhea, and undocumented fever. Physical examination on admission<br />
showed a fairly nourished, fairly developed individual who was not in distress. A low-grade fever<br />
of 37.8 O C was noted. Abdominal examination showed voluntary guarding, direct and rebound<br />
tenderness on both lower quadrants. Internal examination showed an ill-defined tender mass<br />
about 2 centimeters in its widest diameter with exquisite tenderness of the cervix on wriggling.<br />
No discharge was noted. Admitting impression was acute abdomen, rule out ectopic pregnancy.<br />
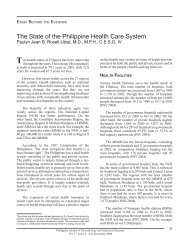
On admission, an exploratory laparotomy was done which revealed mucopurulent<br />
discharge in the pelvic cavity amounting to 250 cc. The left ovary was cystic, measured 4 x 3 x 2<br />
cm, and with a mucopurulent discharge oozing from a point of rupture at its superior pole, Figure<br />
1. The right ovary was grossly normal except for the presence of a follicular cyst. Both fallopian<br />
tubes were slightly edematous, although the uterus was grossly normal. The appendix was<br />
edematous and hyperemic. There was no point of rupture. However, there was fibrin coating the<br />
whole structure. A left oophorectomy and appendectomy was performed with pelvic drainage.<br />
The patient was started on intravenous preparations of metronidazole 500 mg q 8h and<br />
clindamycin 300 mg IV q 6h for three days after whic h therapy was changed to oral preparations.<br />
Culture of the ovarian discharge showed a heavy growth of <strong>Salmonella</strong> typhi. Oral ciprofloxacin<br />
500 mg q 8 hours for ten days was given and metronidazole was continued at 500 mg tablets q 6<br />
hours for possible co-existing anaerobic infection. The patient remained afebrile and was<br />
discharged asymptomatic.<br />
Figure 1. Schematic representation of operative findings showing the left ovarian abscess and its point of<br />
rupture<br />
DISCUSSION<br />
Localization of salmonella infection following a bacteremia is not very common. It has<br />
been said to commonly follow salmonella bacteremia although it may occur after enteric fever or
gastroenteritis. 1 <strong>Abscess</strong>es secondary to salmonella infection was reported by Saphra et al (1957)<br />
as occurring in 1% (136/7779) cases of salmonellosis. These were frequently directly or indirectly<br />
connected with the gastrointestinal tract as peri-proctal, perineal, subphrenic or appendiceal. 2<br />
<strong>Salmonella</strong> infections of the liver, spleen, peritoneum and bone associated with enteric fever have<br />
been reported but localized ovarian abscesses are very rare. Since 1893, when it was first<br />
reported, there have only been 41 cases reported. 3,4,5<br />
Clinical manifestations of localized <strong>Salmonella</strong> infection would largely depend on the<br />
structures involved. The usual presenting symptoms in ovarian abscesses were abdominal pain,<br />
nausea and vomiting. Purulent cervical discharge was seen only in 16% of cases. 5 Fever is also a<br />
consistent symptom seen in all patients in whom temperatures were recorded. These symptoms<br />
would occur from several weeks to months after the initial salmonella infection.<br />
Physical examination usually reveals abdominal pain or pelvic tenderness, and/or<br />
palpable adnexal masses. Laboratory data in over half the patients had leukocytosis, 2/7 had<br />
bacteremia, 3/9 had positive stool cultures. In females, the most common serotype seen was<br />
<strong>Salmonella</strong> typhi. 6 Bacteriologic diagnosis can usually be obtained from the material taken in situ.<br />
<strong>Ovarian</strong> abscesses, in general, are usually associated with tubal or pelvic infections, when<br />
the normal ovary is involved by direct spread of organisms from the lower genital tract. In such<br />
cases, the infecting organisms are usually normal vaginal flora or gonococci. 5 Isolated ovarian<br />
abscesses are much less common and in these patients some abnormality of the ovary encourages<br />
the seeding of an organism during a septicemia. 7<br />
It can be noted from previous reports that almost all typhoid infections had been noted in<br />
dermoid cysts with the minority occuring in cystadenomas. From 1893 to 1971, 2 of 20 patients<br />
reported by J.C. Evans-Jones occurred in normal ovaries. 8 In the report of Cohen et al (1987),<br />
anatomic abnormalities were noted in 4/12 women (3 were dermoid cysts and 1 with<br />
cystadenoma). 5<br />
Three mechanisms by which salmonella spread to uterine adnexae are: organisms in the<br />
abdominal cavity gain access during ovulation; an inflamed bowel may have adhered to an ovary<br />
and allowed direct extension of the infection; and spread via blood stream or lymphatics.<br />
The surface of the ovary is damaged during ovulation and in the process any organism<br />
present in the peritoneal cavity will gain access and may proliferate causing abscess formation.<br />
Any infection in the surrounding adnexae or intestine may, by direct extension, involve<br />
the ovaries. Intra-ovarian abscesses are characteristically seen in patients with pelvic<br />
inflammatory disease associated with an intrauterine device (IUD). 10 IUD causes colonization of<br />
the female genital tract by bacteria, which then gain access to the peritoneum through the<br />
fallopian tube. 11 The patient, however, had no history of IUD use. <strong>Ovarian</strong> abscess may also be<br />
seen after a pelvic surgical procedure, especially if there had been ovarian trauma. 10 The most<br />
common type of purulent infection of the ovary is a tubovarian abscess due to ovarian<br />
involvement secondary to acute salpingitis. 11 In contrast, ovarian abscesses unrelated to tubal<br />
disease is very rare. 12 With the history of dilatation and curettage done during the time the patient<br />
had typhoid fever, it is highly likely that PID developed as a consequence with subsequent<br />
ovarian abscess formation.<br />
Early in the course of salmonella bacteremia, the ovaries with a collection of stagnant<br />
blood would have been a likely site for salmonella to establish themselves. 9 The presence of preexisting<br />
disease resulting in necrotic scarred or hyperplastic tissue favors localization of blood<br />
borne organisms. Localized salmonella infections have been seen in many types of benign and<br />
malignant tumors, cysts, aneurysms, bone infarctions and effusions in serous cavities. 13 The<br />
presence of hair, bone, teeth or other tissues in a dermoid cyst or the mucus of a cystadenoma<br />
may act as a similar protected site with chronic infection which may develop into an ovarian<br />
abscess many months or years after the initial septicemic illness. 3<br />
The development of salmonella ovarian abscess in our patient can be explained on the<br />
basis of two hypotheses. First, she had enteric fever during the time that a gynecological
procedure was performed. <strong>Salmonella</strong> infection may have set in resulting in PID, periappendicitis<br />
and ultimately ovarian abscess formation in a pre-existing ovarian cyst. Hence, the<br />
condition may be nosocomially acquired. Second, she may have had salmonella secondarily<br />
infecting an ovarian cyst during the bacteremic phase of typhoid fever, producing a latent<br />
infection, which was activated by a more recent infection.<br />
<strong>Salmonella</strong> genital infections are difficult to eradicate with medical therapy alone,<br />
presumably because of the abscess formation requiring surgical intervention. Surgical drainage of<br />
the localized collection of purulent material and antibiotic coverage are the cornerstones of<br />
therapy. Common antibiotics proven effective in treating salmonella infection are ampicillin,<br />
chloramphenicol, trimethoprim-sulfamethoxazole and amoxicillin. 6 Ampicillin or<br />
chloramphenicol is commonly used for extra intestinal salmonella infections. Trimethoprimsulfamethoxazole<br />
is generally used for organisms resistant to the above two drugs. Evans-Jones<br />
used chloramphenicol successfully in the treatment of salmonella ovarian abscess given at a dose<br />
of 4 gms/day iv for 5 days followed by 2 gms/day PO for 5 more days. 3 Salztsmann et al used<br />
chloramphenicol in combination with ampicillin for 14 days. 14 Ghose et al on the other hand<br />
combined amoxycillin with cotrimoxazole successfully for 2 weeks. 9 These antibiotics had been<br />
used either alone or in combination in the treatment of salmonella ovarian abscess, with varying<br />
degrees of success.<br />
<strong>Salmonella</strong> isolates have become increasingly resistant to these antibiotics. Outbreaks of<br />
salmonella resistant to multiple antibiotics are being reported with increasing frequency. 15,16,17<br />
Since typhoid fever remains an important health problem especially in the Philippines emergence<br />
of resistance makes it necessary to develop potential therapeutic alternatives.<br />
Ciprofloxacin, a quinolone carboxylic acid derivative, has a greater antibacterial activity<br />
than earlier compounds such as nalidixic acid, pipemidic acid, or norfloxacin. Its bactericidal<br />
activity against members of the Enterobacteriaceae, to which salmonella belongs, suggests its<br />
usefulness in the treatment of typhoid fever. Several studies have shown its success in the<br />
treatment of patients with uncomplicated typhoid fever. 18,19,20<br />
There have been no reports however, on the use of ciprofloxacin in localized infections.<br />
The use of ciprofloxacin in this patient may be a precedent for future therapy of salmonella<br />
ovarian abscess.<br />
CONCLUSION<br />
Although salmonella ovarian abscess is a rare condition, it should be considered in the<br />
differential diagnosis of patients with pelvic inflammatory disease who have had a history of<br />
typhoid fever. Treatment must be surgical and suitable antibiotics must be started.<br />
Chloramphenicol is still the drug of choice for uncomplicated typhoid fever.<br />
The onset of complications while on chloramphenicol therapy should make one consider<br />
clinical resistance inspite of in vitro sensitivity of S. typhi. It has also been shown in this report<br />
that ciprofloxacin may be used successfully in the treatment of salmonella ovarian abscess.<br />
REFERENCES<br />
1. Hook EW. <strong>Salmonella</strong> Species (including Typhoid Fever). In Mandell, GL, et al (eds). Principles And Practices of Infectious<br />
Diseases. Third ed. New York: John Wiley and Sons, 1990. pp 1700-1713<br />
2. Saphra I, Winter J. Clinical manifestation of salmonellosis in man. New Engl J Med 1956; 256(24):1128-1134.<br />
3. Evans-Jones JC. An ovarian cyst infected with <strong>Salmonella</strong> typhi. <strong>Case</strong> Report. J Obstet Gynecol 1983; 90:680-682.<br />
4. Taylor TE. Typhoid infection of ovarian cyst. J Obstet Gynecol Br Emp 1907; 12:367-383.<br />
5. Cohen JI, et al. Extraintestinal manifestations of salmonella infections. Medicine 1987; 66(4):349-388.<br />
6. Soloff LA, Hermann CS. Chronic typhoid abscess of the ovary. Am J Obstet Gynecol 1935; 30:290-292.<br />
7. Black WT. <strong>Abscess</strong>es of the ovary. Am J Obstet Gynecol 1936; 31:487-494.<br />
8. Wilson JK, Black JR. <strong>Ovarian</strong> abscess. Am J Obstet Gynecol 1964; 90:34-43.<br />
9. Ghose AR,. et al. Bilateral salmonella salphingooophoritis. Post Grad Med 1986; 62:228.<br />
10. <strong>Case</strong> Records of Massachusetts General Hospital. New Engl I ofMed 1986 835-842.
11. Lander DV, et al. Current trends in the diagnosis and treatment of tubo-ovarian abscess. Am J Obstet Gynecol 1985; 151:1098-<br />
1110.<br />
12. Wetchler SI. <strong>Ovarian</strong> abscess: a report of a case and a review of literature. Obstet Gynecol Surg 1986; 151:1098-110.<br />
13. Bennet Itw, Ir, et al. Infectious Diseases (some aspects of salmonellosis) Ann Rev Med 1959; 10:1.<br />
14. Saltzmann DH, et al. Nongonococcal pelvic abscess caused by <strong>Salmonella</strong> enteritidis. Obstet Gynecol 1984; 64: 585.<br />
15. Neu HC, et al. Antimicrobial resistance and R-factor transfer among isolates of salmonella in Northeastern United States. A<br />
comparison of human and animal isolates. J Infect Dis 1975; 132:617-22.<br />
16. Bryan JP, et al. Problems in salmonellosis: Rationale for clinical trials with newer B-lactam agents and quinolones. Rev Infect<br />
Dis 1986 ; 8:189-107.<br />
17. McHugh G, et al. <strong>Salmonella</strong> typhimurium resistant to silver nitrate, chloramphenicol and ampicillin. Lancet 1975 ; 1:235-239.<br />
18. Limson BM, et al. Summary of clinical trials with ciprofloxacin in the Philippines. The Philippine Society for Microbiology and<br />
Infectious Diseases. The First Philippine Ciprofloxacin Symposium and Clinical Experiences in the Philippines, 1985. pp. 73-74.<br />
19. Limson BM. Efficacy and safety of ciprofloxacin in uncomplicated typhoid fever. Neu H, Wenta (eds.) Proceedings of the First<br />
International Ciprofloxacin Workshop. Excepta medica, 1985. pp. 362-364<br />
20. Ramirez CA. Clinical efficacy of ciprofloxacin. Neu, H, Wenta (eds.) Proceedings of the First International Cipro-floxacin<br />
Workshop. Excerpta medica, 1985. pp. 365-369.