Management of morbid obesity - The Journal of Family Practice
Management of morbid obesity - The Journal of Family Practice
Management of morbid obesity - The Journal of Family Practice

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Free<br />
2.5 CME<br />
credits<br />
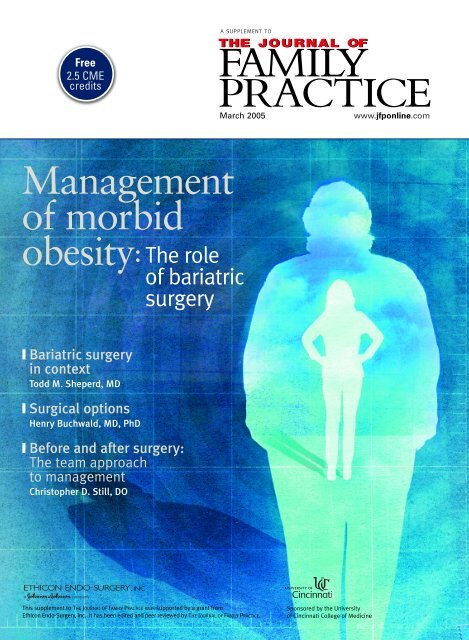
<strong>Management</strong><br />
<strong>of</strong> <strong>morbid</strong><br />
<strong>obesity</strong>:<br />
❙ Bariatric surgery<br />
in context<br />
Todd M. Sheperd, MD<br />
❙ Surgical options<br />
Henry Buchwald, MD, PhD<br />
❙ Before and after surgery:<br />
<strong>The</strong> team approach<br />
to management<br />
Christopher D. Still, DO<br />
A SUPPLEMENT TO<br />
<strong>The</strong> role<br />
<strong>of</strong> bariatric<br />
surgery<br />
This supplement to THE JOURNAL OF FAMILY PRACTICE was supported by a grant from<br />
Ethicon Endo-Surgery, Inc. It has been edited and peer reviewed by THE JOURNAL OF FAMILY PRACTICE.<br />
THE JOURNAL OF<br />
FAMILY<br />
PRACTICE<br />
March 2005 www.jfponline.com<br />
Sponsored by the University<br />
<strong>of</strong> Cincinnati College <strong>of</strong> Medicine
<strong>Management</strong> <strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>: <strong>The</strong> role <strong>of</strong> bariatric surgery<br />
<strong>Management</strong><br />
<strong>of</strong> <strong>morbid</strong><br />
<strong>obesity</strong>:<br />
Publication date: March 2005<br />
Expiration date: March 2006<br />
Learning objectives:<br />
Upon completion <strong>of</strong> this program, participants should be able to:<br />
■ Place bariatric surgery in the context <strong>of</strong><br />
overall management <strong>of</strong> <strong>obesity</strong><br />
<strong>The</strong> role<br />
<strong>of</strong> bariatric<br />
surgery<br />
■ Identify and refer patients who may be candidates<br />
for bariatric surgery<br />
■ Advise patients on the benefits and risks associated<br />
with various bariatric surgical procedures, as well as<br />
the long-term commitment required<br />
■ Participate in preoperative assessment and treatment,<br />
if indicated<br />
■ Participate in postoperative management and follow-up<br />
Sponsorship<br />
<strong>The</strong> University <strong>of</strong> Cincinnati College <strong>of</strong> Medicine designates this<br />
educational activity for a maximum <strong>of</strong> 2.5 category 1 credits<br />
toward the AMA Physician’s Recognition Award. Each physician<br />
should claim only those hours that he/she actually spent on the<br />
activity. This CME activity has been planned and implemented in<br />
accordance with the Essential Areas and Policies <strong>of</strong> the<br />
Accreditation Council for Continuing Medical Education (ACCME)<br />
through the joint sponsorship <strong>of</strong> the University <strong>of</strong> Cincinnati College<br />
<strong>of</strong> Medicine and Dowden Health Media. <strong>The</strong> University <strong>of</strong><br />
Cincinnati College <strong>of</strong> Medicine is accredited by the ACCME to provide<br />
continuing medical education for physicians.<br />
Audience<br />
<strong>Family</strong> physicians and other primary care practitioners.<br />
Acknowledgment:<br />
This CME activity is supported by an unrestricted educational<br />
grant from Ethicon Endo-Surgery, Inc.<br />
Faculty Disclosures<br />
■ Dr Sheperd reports no financial relationship with any<br />
company whose products are mentioned in this supplement.<br />
■ Drs Buchwald and Still serve as consultants to Ethicon Endo-<br />
Surgery, Inc.<br />
COPYRIGHT © 2005 BY DOWDEN HEALTH MEDIA, MONTVALE, NJ<br />
2 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> March 2005<br />
Bariatric surgery in context . . . . . . . . . . . . . . . . . . 3<br />
Todd M. Sheperd, MD<br />
Assistant Clinical Pr<strong>of</strong>essor<br />
Department <strong>of</strong> <strong>Family</strong> Medicine<br />
Michigan State University College <strong>of</strong> Human Medicine<br />
Traverse City, Mich<br />
Surgical options . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10<br />
Henry Buchwald, MD, PhD<br />
Pr<strong>of</strong>essor, Department <strong>of</strong> Surgery<br />
Owen H. and Sarah Davidson Wangensteen Chair<br />
in Experimental Surgery Emeritus<br />
University <strong>of</strong> Minnesota Medical School<br />
Minneapolis, Minn<br />
Before and after surgery:<br />
<strong>The</strong> team approach to<br />
management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18<br />
Christopher D. Still, DO<br />
Director, Center for Nutrition and Weight <strong>Management</strong><br />
Geisinger Health Care System<br />
Danville, Pa<br />
CME posttest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26<br />
CME registration form and<br />
program evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Bariatric surgery in context<br />
Todd M. Sheperd, MD<br />
Assistant Clinical Pr<strong>of</strong>essor<br />
Department <strong>of</strong> <strong>Family</strong> Medicine<br />
Michigan State University College <strong>of</strong> Human Medicine<br />
Traverse City, Mich<br />
Obesity is now pandemic in the United States and<br />
other industrialized countries (FIGURE 1), 1-3 the<br />
result by and large <strong>of</strong> a combination <strong>of</strong> inappropriate<br />
diets and inadequate exercise. And the problem is<br />
no longer confined to industrialized countries. Rapid<br />
Westernization <strong>of</strong> diet and lifestyle among urban<br />
dwellers in India, China, and elsewhere has been followed<br />
by an alarming rise in <strong>obesity</strong>-related health<br />
problems. 4,5<br />
<strong>The</strong> <strong>morbid</strong>ly obese patient presents a particular<br />
challenge because <strong>of</strong> the massive weight loss that<br />
needs to be achieved. It was for this patient that<br />
bariatric surgery was first proposed in the 1950s,<br />
leading to emergence <strong>of</strong> a surgical specialty that last<br />
year performed more than 140,000 operations in the<br />
United States. As Henry Buchwald will discuss in the<br />
next article, the safety and efficacy <strong>of</strong> bariatric surgical<br />
techniques have improved over the years and a<br />
substantial body <strong>of</strong> evidence has been accumulated.<br />
<strong>The</strong> clinician <strong>of</strong>ten is reluctant to consider bariatric<br />
surgery as an option even though nonsurgical treatments<br />
for severe <strong>obesity</strong> remain far from ideal. When all<br />
available options for managing <strong>morbid</strong> <strong>obesity</strong> are compared,<br />
it is difficult to dismiss operative therapy as a<br />
viable consideration.<br />
Startling statistics<br />
Obesity is defined as a body mass index (BMI) greater<br />
than 30 kg/m 2 . <strong>The</strong> pre-<strong>obesity</strong> or overweight stage<br />
includes BMIs <strong>of</strong> at least 25 kg/m 2 but less than 30 kg/m 2 .<br />
Patients with BMIs greater than 40 kg/m 2 are considered<br />
to be extremely or <strong>morbid</strong>ly obese (class III <strong>obesity</strong>), as<br />
are those with BMIs greater than 37 kg/m 2 and <strong>obesity</strong>related<br />
co<strong>morbid</strong>ity. 6 Although other measures <strong>of</strong> <strong>obesity</strong><br />
are available, BMI is easily determined; moreover, it is<br />
THE JOURNAL OF<br />
FAMILY<br />
PRACTICE<br />
used as the standard for weight determination in the<br />
majority <strong>of</strong> clinical studies <strong>of</strong> <strong>obesity</strong>. 7<br />
On basis <strong>of</strong> these BMI criteria, approximately 65%<br />
<strong>of</strong> adults in the United States are overweight, and<br />
31%—an 8% increase in 1 decade—are obese. 1 More<br />
than 15% <strong>of</strong> adolescents are overweight, up from about<br />
5% in the early 1970s (FIGURE 2). 7 In the last 10 to 15<br />
years, the average BMI <strong>of</strong> the US population has<br />
increased from 24.9 to 26.5 kg/m 2 . 8<br />
<strong>The</strong> prevalence <strong>of</strong> class III <strong>obesity</strong> rose even<br />
faster—today, an estimated 2.2% to 4.7% <strong>of</strong><br />
Americans are <strong>morbid</strong>ly obese. 1,2,8 <strong>The</strong> prevalence is<br />
particularly high among US women, 6.3% <strong>of</strong> whom<br />
are now <strong>morbid</strong>ly obese, while among non-Hispanic<br />
black women the rate is now 15%. 1 Using data from<br />
the Behavioral Risk Factor Surveillance System, Sturm<br />
calculated that the prevalence <strong>of</strong> BMIs <strong>of</strong> 40 kg/m 2 and<br />
higher quadrupled between 1986 and 2000, while the<br />
prevalence <strong>of</strong> BMIs <strong>of</strong> 50 kg/m 2 and higher—the heaviest<br />
Americans—increased by a factor <strong>of</strong> 5. 9<br />
When <strong>obesity</strong> remains untreated<br />
Left untreated, <strong>obesity</strong> is implicated in the development<br />
<strong>of</strong> multiple co<strong>morbid</strong>ities including hypertension, type 2<br />
diabetes, coronary artery disease, osteoarthritis, and<br />
some types <strong>of</strong> cancer (TABLE 1). 10,11 Because most <strong>of</strong><br />
these diseases are correlated directly with BMI, 10,12 the<br />
patient with class III <strong>obesity</strong> is most likely to have them.<br />
Not surprisingly, <strong>obesity</strong> also is associated with<br />
increased risk <strong>of</strong> mortality—it contributes directly to<br />
approximately 280,000 deaths per year. 13 Even though<br />
class III patients represent a minority <strong>of</strong> the obese population,<br />
mortality in this subgroup is disproportionately<br />
high (relative risk, 1.9-2.6). 13,14<br />
Recent analyses have estimated that in 2000,<br />
March 2005 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> 3
<strong>Management</strong> <strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>: <strong>The</strong> role <strong>of</strong> bariatric surgery<br />
FIGURE 1<br />
400,000 deaths in the United States were attributable to<br />
poor diet and lack <strong>of</strong> regular physical activity. 15 In addition,<br />
loss <strong>of</strong> normal life expectancy for 25-year-olds<br />
with class III <strong>obesity</strong> is estimated to be as much as 20<br />
years for black men, 13 years for white men, 5 years for<br />
black women, and 8 years for white women. 16<br />
Whether <strong>obesity</strong> contributes directly to mortality<br />
independently <strong>of</strong> poor diet and sedentary lifestyle<br />
remains controversial. 17 Moreover, there is disagreement<br />
about the effect <strong>of</strong> weight loss on mortality because <strong>of</strong><br />
the difficulty in separating intentional weight loss from<br />
disease-related weight loss. In a recent prospective<br />
study, Gregg et al concluded that intentional weight loss<br />
is associated with a 24% reduction (relative risk, 0.76;<br />
95% CI, 0.60-0.97) in mortality. 18<br />
Diabetes<br />
Type 2 diabetes mellitus is clearly linked to <strong>obesity</strong>.<br />
<strong>The</strong> estimated 10-year odds ratio for the development<br />
<strong>of</strong> type 2 diabetes is 17 in men and women with BMIs<br />
greater than 30 kg/m 2 . For patients with BMIs greater<br />
than 35 kg/m 2 , the odds ratio increases to 34 in women<br />
and 41 in men. 10 Approximately 11% <strong>of</strong> men and<br />
20% <strong>of</strong> women with class III <strong>obesity</strong> also have type 2<br />
Prevalence <strong>of</strong> <strong>obesity</strong> among US adults<br />
1991 2003<br />
In 1991, the highest <strong>obesity</strong> (BMI ≥30 kg/m2 ) prevalence rate by state among US adults was 15% to 19%, and it was documented in only 4<br />
states. In 2003, this prevalence rate was noted in 15 states; moreover, 31 states had rates <strong>of</strong> 20% to 24%, and 4 states had rates <strong>of</strong> more than<br />
25%. Adapted from Behavioral Risk Factor Surveillance System (BRFSS), Centers for Disease Control and Prevention, and Mokdad et al. 2<br />
No data 25%<br />
4 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> March 2005<br />
diabetes. 10 Multiple studies involving men, women,<br />
and various ethnic groups have confirmed an association<br />
between <strong>morbid</strong> <strong>obesity</strong> and type 2 diabetes. 10,11,19<br />
<strong>The</strong> effect <strong>of</strong> weight loss on type 2 diabetes can be<br />
significant. For example, Anderson and Konz reported<br />
that for every 5-kg weight loss, the average fasting glucose<br />
level decreased by 18 mg/dL. 12 In particular, bariatric<br />
surgery is associated with dramatic and prolonged<br />
improvement in blood glucose control. Blood glucose values<br />
are normalized in 77% to 86% <strong>of</strong> patients with type<br />
2 diabetes who undergo surgery for <strong>morbid</strong> <strong>obesity</strong>. 20-23<br />
Coronary artery disease<br />
Obesity has been identified as an independent risk factor<br />
for the development <strong>of</strong> coronary artery disease<br />
(CAD) in both men and women. <strong>The</strong> magnitude <strong>of</strong> the<br />
risk is similar to that <strong>of</strong> other coronary risk factors,<br />
including hyperlipidemia, hypertension, and cigarette<br />
smoking. 12,24 <strong>The</strong> relative risk for the development <strong>of</strong><br />
CAD in patients with BMIs greater than 30 kg/m 2 is<br />
approximately 1.6 times that <strong>of</strong> their normal-weight<br />
counterparts, even after adjusting for other CAD risk<br />
factors. 11,24,25 In <strong>morbid</strong>ly obese patients, the relative risk<br />
<strong>of</strong> CAD is approximately 1.7 to 2.2 times greater than
in their normal-weight<br />
counterparts. 10,11 It has been<br />
calculated that for every<br />
kilogram <strong>of</strong> weight gained<br />
after high school, the risk<br />
<strong>of</strong> CAD increases by 5.7%<br />
in women and by 3.1% in<br />
men. 12 Data on the effects<br />
<strong>of</strong> bariatric surgery on the<br />
onset or progression <strong>of</strong><br />
CAD are lacking, and<br />
prospective cohort studies<br />
have failed to demonstrate<br />
a reduction in cardiovascular<br />
mortality when intentional<br />
weight loss is<br />
achieved nonsurgically. 26<br />
FIGURE 2<br />
Hypertension<br />
Men with class III <strong>obesity</strong><br />
are 1.7 to 4.6 times more<br />
likely to have hypertension than matched normal-weight<br />
controls. In <strong>morbid</strong>ly obese women, the risk increases by<br />
a factor <strong>of</strong> 1.4 to 5.5. 2,10<br />
As with diabetes, weight loss ameliorates hypertension.<br />
In obese patients, every 1-kg decrease in body<br />
weight is accompanied by an average decrease <strong>of</strong> 0.6<br />
mm Hg in systolic blood pressure and 0.34 mm Hg in<br />
diastolic pressure. 12 <strong>The</strong> beneficial effect <strong>of</strong> weight loss<br />
on blood pressure is consistently seen when weight loss<br />
is achieved through lifestyle modification; 27 however, it<br />
may not occur when weight loss is achieved with<br />
appetite-suppressing drugs. 6,12,28,29 Bariatric surgery is<br />
associated with complete resolution <strong>of</strong> hypertension in<br />
60% to 70% <strong>of</strong> patients with <strong>morbid</strong> <strong>obesity</strong>. 22,30<br />
Arthritis<br />
<strong>The</strong> risk <strong>of</strong> osteoarthritis, predominantly in the weightbearing<br />
joints, is increased in all obese patients. 11,31 In<br />
patients with class III <strong>obesity</strong>, the relative risk for<br />
osteoarthritis is 10. 11 <strong>The</strong> knee joint is particularly vulnerable—for<br />
every 5-unit increase in BMI, the relative<br />
risk for bilateral knee arthritis increases by 2.6. 31 An<br />
increasing prevalence <strong>of</strong> hip arthritis also has been correlated<br />
directly with increasing BMI.<br />
Total knee and hip arthroplasty rates are strongly<br />
associated with progressive <strong>obesity</strong>. In <strong>morbid</strong>ly obese<br />
THE JOURNAL OF<br />
FAMILY<br />
PRACTICE<br />
Prevalence <strong>of</strong> overweight among US children and adolescents<br />
Prevalence (%)<br />
20<br />
15<br />
10<br />
5<br />
0<br />
■ 1971-1974<br />
■ 1988-1994<br />
■ 1999-2000<br />
2-5 6-11<br />
Age (yr)<br />
12-19<br />
From 1977 to 2000, the prevalence <strong>of</strong> overweight (95% <strong>of</strong> BMI for age) increased 5% among children<br />
aged 2 to 5 years, 11% among children aged 6 to 11 years, and 10% among adolescents (12-19 yr). Data<br />
derived from First National Health and Nutrition Examination Survey (NHANES I), 1971-1974; NHANES<br />
III, 1988-1994; and NHANES 1999-2000. Adapted from Ogden et al. 7<br />
men, the odds ratios <strong>of</strong> total knee and hip arthroplasty<br />
are 16 and 9, respectively. 32 Morbidly obese women are<br />
19 times more likely to undergo knee replacement than<br />
normal-weight controls. 32<br />
In patients with established arthritis, weight loss is<br />
associated with decreased pain and increased function.<br />
33 Weight loss also has been associated with<br />
decreased progression <strong>of</strong> knee arthritis, 34 but not <strong>of</strong> hip<br />
arthritis. 35 Joint pain is alleviated after bariatric surgery,<br />
and surgical patients also are more likely to be physically<br />
active than their nonsurgical counterparts. 36,37<br />
Cancer<br />
Observational studies have noted that elevated BMIs<br />
were associated with increasing risk <strong>of</strong> several cancers,<br />
including but not limited to, cancer <strong>of</strong> the breast, colon,<br />
prostate, ovaries, and uterus (FIGURE 3). 10,38 Although<br />
precise mechanisms have not been elucidated, a likely<br />
hypothesis is that accumulating adipose tissue affects<br />
circulating levels <strong>of</strong> tumor-promoting peptides and<br />
steroid hormones. 39<br />
<strong>The</strong> relative risk <strong>of</strong> colon cancer in patients with<br />
BMIs greater than 35 kg/m 2 is 1.8 to 2.2. 9,38 As is seen<br />
with other <strong>obesity</strong> related conditions, increasing <strong>obesity</strong><br />
escalates the risk <strong>of</strong> cancer. Studies <strong>of</strong> women have shown<br />
that intentional weight loss was associated with a reduced<br />
March 2005 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> 5
<strong>Management</strong> <strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>: <strong>The</strong> role <strong>of</strong> bariatric surgery<br />
TABLE 1<br />
Cardiovascular<br />
Dyslipidemia<br />
Coronary artery disease<br />
Cardiomyopathy<br />
Hypertension<br />
Congestive heart failure<br />
Deep vein thrombosis<br />
Pulmonary embolism<br />
Pulmonary hypertension<br />
Cor pulmonale<br />
Cerebrovascular<br />
Stroke<br />
Idiopathic intracranial<br />
hypertension<br />
Medical conditions that may be associated with severe <strong>obesity</strong><br />
Respiratory<br />
Sleep apnea<br />
Asthma<br />
Hypoventilation syndrome<br />
Chronic obstructive<br />
pulmonary disease<br />
Gastrointestinal<br />
Gastroesophageal reflux<br />
Fatty liver<br />
Nonalcoholic steatohepatitis<br />
Cholelithiasis<br />
Hernia<br />
Genitourinary<br />
Urinary stress incontinence<br />
Hypogonadism<br />
Psychoneurologic<br />
Depression<br />
Migraine headache<br />
Pseudotumor cerebri<br />
Carpal tunnel syndrome<br />
Integumentary<br />
Venous stasis<br />
Superficial thrombophlebitis<br />
Cellulitis<br />
Panniculitis<br />
Postoperative wound infection<br />
Fungal infections<br />
Adapted from Mun EC, Blackburn GL, Matthews JB. Current status <strong>of</strong> medical and surgical therapy for <strong>obesity</strong>.<br />
Gastroenterology. 2001;120:669-681; American Obesity Association. AOA fact sheets: health effects <strong>of</strong> <strong>obesity</strong>.<br />
Available at http://www.<strong>obesity</strong>.org/subs/fastfacts/Health_Effects.shtml. Accessed December 29, 2004.<br />
incidence <strong>of</strong> all cancers, as well as breast and colon cancer.<br />
40,41 <strong>The</strong>se studies did not specify the methods <strong>of</strong><br />
weight loss, and it has yet to be determined whether surgically<br />
induced weight loss reduces cancer risk.<br />
<strong>The</strong> high cost <strong>of</strong> <strong>obesity</strong><br />
About $50 billion annually are spent on direct care <strong>of</strong> <strong>obesity</strong>-related<br />
complications and another $30 billion are<br />
spent on weight-loss products and programs. 6 This sum<br />
accounts for nearly 5% <strong>of</strong> all medical costs in the United<br />
States. 6 In addition to the cost <strong>of</strong> treating associated medical<br />
conditions, obese patients are less productive and<br />
more prone to disability. 42 Thus, strategies aimed at reducing<br />
the burden <strong>of</strong> <strong>obesity</strong> are likely to have a major impact<br />
on the US health care system and society as a whole.<br />
Psychosocial impact<br />
Patients with class III <strong>obesity</strong> <strong>of</strong>ten have significant psy-<br />
6 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> March 2005<br />
Endocrine<br />
Insulin resistance<br />
Impaired glucose tolerance<br />
Type 2 diabetes<br />
Impotence<br />
Amenorrhea<br />
Dysmenorrhea<br />
Polycystic ovary syndrome<br />
Infertility<br />
Hirsutism<br />
Gynecomastia<br />
Musculoskeletal<br />
Low back pain<br />
Vertebral disc herniation<br />
Osteoarthritis<br />
Malignancies<br />
Breast cancer<br />
Endometrial cancer<br />
Colon cancer<br />
Prostate cancer<br />
Uterine cancer<br />
chosocial complications that can be attributed to their<br />
weight. In particular, <strong>morbid</strong>ly obese patients report<br />
impaired mobility, reduced energy levels, a high degree <strong>of</strong><br />
emotional distress, and impaired psychosocial functioning<br />
(eg, social isolation, feelings <strong>of</strong> failure and hopelessness).<br />
43,44 Psychosocial complications are reinforced by<br />
social, educational, and workplace stigmatization—potential<br />
partners, teachers, school administrators, employers,<br />
and even physicians and other health pr<strong>of</strong>essionals tend to<br />
rate obese individuals unfavorably compared with individuals<br />
<strong>of</strong> normal weight. 44,45 Several studies have used validated<br />
survey instruments to demonstrate that the quality<br />
<strong>of</strong> life decreases as BMI increases and that as weight is lost,<br />
patients report improved quality <strong>of</strong> life. 44-46<br />
Nonsurgical treatment<br />
Nonsurgical treatment for extremely obese patients<br />
includes lifestyle changes (eg, diet and exercise), pharmacologic<br />
therapy, alternative drug therapies and tech-
niques, and psychotherapy<br />
(TABLE 2). A substantial<br />
body <strong>of</strong> literature is available<br />
for assessment <strong>of</strong> these<br />
options.<br />
Morbidly obese patients<br />
typically are more than 100<br />
lb (~45 kg) overweight.<br />
<strong>The</strong>refore, they need to be<br />
managed with treatments<br />
that have the potential to<br />
achieve substantial weight<br />
reductions and thereby correct<br />
<strong>obesity</strong>-related metabolic<br />
abnormalities. To date,<br />
all nonsurgical treatments<br />
for <strong>obesity</strong> have demonstrated<br />
maximum average<br />
weight-losses <strong>of</strong> 3 to 6 kg. 6,47<br />
In addition, noncompliance<br />
rates approximate 50%,<br />
and relapse rates after cessa-<br />
FIGURE 3<br />
Relative risk for any cancer<br />
tion <strong>of</strong> treatment approach nearly 100%. 6,47 Clearly, the<br />
primary care physician has few effective nonsurgical<br />
options for the <strong>morbid</strong>ly obese patient.<br />
Lifestyle changes<br />
Modification <strong>of</strong> diet (restriction <strong>of</strong> caloric intake) and<br />
aerobic exercise (increased energy consumption) form<br />
the mainstay <strong>of</strong> lifestyle changes. Dietary changes can<br />
decrease weight approximately 3 to 6 kg and adding<br />
exercise to a diet may be more effective than diet alone. 6<br />
No specific type <strong>of</strong> diet (eg, low-calorie vs low-carbohydrate)<br />
has been shown to be superior when caloric<br />
intakes <strong>of</strong> the diets are equivalent. 6,48 When used as<br />
monotherapy, exercise <strong>of</strong>fers minimal improvement, but<br />
it may prevent additional weight gain and improves cardiovascular<br />
fitness. 6<br />
As mentioned, the major concerns about using<br />
lifestyle changes in the treatment for the <strong>morbid</strong>ly obese<br />
patient are the relatively small impact on the patient’s<br />
total weight, the high rates <strong>of</strong> attrition, and the high rates<br />
<strong>of</strong> weight regain over time. 47<br />
Pharmacologic therapy<br />
Numerous medications have been used in the management<br />
<strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>, but only two <strong>of</strong> them,<br />
2.0<br />
1.5<br />
1.0<br />
0.5<br />
0.0<br />
■ Men<br />
■ Women<br />
1.00 1.00 0.97<br />
BMI and cancer mortality<br />
1.08<br />
THE JOURNAL OF<br />
FAMILY<br />
PRACTICE<br />
18.5-24.9 25.0-29.9 30.0-34.9 35.0-39.9 ≥40<br />
Risk for death from all cancers increased as BMI increased in more than 900,000 US adults followed for<br />
16 years. Morbidly obese persons (BMI ≥40 kg/m 2 ) had the highest cancer death rates, with overall rates<br />
52% higher in men and 62% higher in women, compared with normal-weight adults. <strong>The</strong> most common<br />
weight-related cancer was liver cancer in men (combined risk ratio, 4.52 for BMI ≥35 kg/m 2 ) and cancer <strong>of</strong><br />
the corpus and uterus in women (combined risk ratio, 6.25 for BMI ≥35 kg/m 2 ). Overweight and <strong>obesity</strong><br />
were linked to 14% <strong>of</strong> deaths from cancer in men and 20% in women. Adapted from Calle et al. 39<br />
1.09<br />
BMI (kg/m 2 )<br />
1.23 1.20<br />
1.32<br />
1.52<br />
1.62<br />
sibutramine and orlistat, have been approved for longterm<br />
use. <strong>The</strong> US Food and Drug Administration includes<br />
the proviso that these 2 agents be administered in conjunction<br />
with a reduced-calorie diet.<br />
Sibutramine suppresses appetite through its inhibition<br />
<strong>of</strong> norepinephrine, serotonin, and dopamine reuptake.<br />
In clinical studies, patients taking sibutramine had<br />
a weight loss that was about 4 to 5 kg greater than that<br />
in placebo patients after 1 year <strong>of</strong> treatment. 28,29,47,49<br />
Even more significant, these studies excluded patients<br />
with BMIs greater than 40 kg/m 2 . Indeed, no studies <strong>of</strong><br />
the efficacy <strong>of</strong> sibutramine in <strong>morbid</strong>ly obese patients<br />
have been completed.<br />
Attrition rates in sibutramine trials have ranged<br />
from 17% to 47%. <strong>The</strong> most common side effects<br />
were dry mouth, anorexia, insomnia, constipation,<br />
and headache. 28,29,49 <strong>The</strong> agent also has been associated<br />
with small elevations <strong>of</strong> blood pressure and heart<br />
rate and should be administered with caution in<br />
patients with hypertension, particularly when it is<br />
uncontrolled or poorly controlled.<br />
Orlistat is a lipase inhibitor that prevents absorption<br />
<strong>of</strong> dietary fats in the stomach and small intestine.<br />
A Cochrane review <strong>of</strong> 11 orlistat trials indicated that<br />
patients taking orlistat had a 2.7-kg weight loss<br />
March 2005 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> 7
<strong>Management</strong> <strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>: <strong>The</strong> role <strong>of</strong> bariatric surgery<br />
TABLE 2<br />
NIH guidelines for treatment <strong>of</strong> <strong>obesity</strong><br />
BMI (kg/m 2 )<br />
25-26.9 27-29.9 30-34.9 35-39.9 ≥40<br />
Lifestyle Yes, with ≥2 Yes, with ≥2<br />
therapy risk factors or risk factors or Yes Yes Yes<br />
co<strong>morbid</strong>ities co<strong>morbid</strong>ities<br />
Drug Yes, with<br />
therapy* No risk factors or Yes Yes Yes<br />
co<strong>morbid</strong>ities<br />
Bariatric No No No Yes, with Yes<br />
surgery co<strong>morbid</strong>ities<br />
*Drug therapy is indicated in patients who fail to lose 0.45 kg a week during 6 months <strong>of</strong> lifestyle therapy.<br />
Adapted from NHLBI Obesity Education Initiative. <strong>The</strong> Practical Guide to the Identification, Evaluation,<br />
and Treatment <strong>of</strong> Overweight and Obesity in Adults. NIH Publication No. 00-4084. October 2000.<br />
greater than patients taking placebo (95% CI, 2.3-<br />
3.1). 49 Attrition rates ranged from 14% to 52% (average,<br />
33%). Orlistat is associated with a high incidence<br />
<strong>of</strong> gastrointestinal side effects; they occurred 16% to<br />
40% more <strong>of</strong>ten in orlistat patients than in placebo<br />
patients. <strong>The</strong> most common <strong>of</strong> these, occurring in 15%<br />
to 30% <strong>of</strong> patients taking orlistat, were fatty/oily stool,<br />
fecal urgency, and oily spotting. Fecal incontinence<br />
occurred in 6% <strong>of</strong> patients in the 3 studies that reported<br />
this side effect.<br />
Most orlistat trials also excluded patients with<br />
BMIs greater than 40 kg/m 2 , which limits application <strong>of</strong><br />
these data to patients with class III <strong>obesity</strong>. 49 Both orlistat<br />
and sibutramine may improve quality-<strong>of</strong>-life parameters<br />
and may have a modest beneficial impact on lipid<br />
levels and metabolic parameters (eg, blood glucose,<br />
hemoglobin A 1c). However, discontinuation <strong>of</strong> therapy<br />
is associated with return <strong>of</strong> previously lost weight. 49<br />
Alternative therapies<br />
Obese patients <strong>of</strong>ten turn to alternative therapies such as<br />
hypnosis, acupuncture, and over-the-counter dietary supplements.<br />
Studies <strong>of</strong> hypnosis and acupuncture have<br />
shown that these techniques do not provide consistent<br />
improvement over placebo (ie, sham procedure). 50,51<br />
Over-the-counter dietary supplements that have been<br />
studied include chitosan, chromium picolate, Ephedra<br />
8 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> March 2005<br />
sinica, Garcinia cambogia,<br />
glucomannan, guar gum,<br />
hydroxy-methyl butyrate,<br />
plantago psyllium, pyruvate,<br />
yerba maté, and yohimbe. A<br />
systematic review <strong>of</strong> such<br />
studies concluded that none<br />
<strong>of</strong> these agents have shown<br />
consistent results in promoting<br />
weight loss; moreover,<br />
safety is a significant concern<br />
with several <strong>of</strong> them. 52 Thus,<br />
they cannot be recommended<br />
for use in clinical practice,<br />
at least until further research<br />
has been performed.<br />
Psychotherapy<br />
Structured psychotherapy<br />
aimed at weight reduction includes behavioral modification<br />
techniques (eg, stimulus control, self-monitoring,<br />
and cognitive restructuring) that increase compliance<br />
with dietary changes, exercise regimens, or both. 53 No<br />
one technique has been proven superior when judged by<br />
the amount <strong>of</strong> weight lost. 6 <strong>The</strong> majority <strong>of</strong> weight loss in<br />
patients undergoing psychotherapy and supervised<br />
lifestyle change occurred during the first year <strong>of</strong> treatment.<br />
At 5-year follow-up, there was no statistically significant<br />
difference between intervention and control<br />
groups. 6 Programs with the most patient contact tended<br />
to produce the largest weight loss. 6<br />
Summary<br />
<strong>The</strong> family physician is <strong>of</strong>ten the <strong>morbid</strong>ly obese patient’s<br />
first contact with the health care system, there by providing<br />
an opportunity to influence management in a patientoriented<br />
manner that focuses on outcomes such as weight<br />
loss, associated co<strong>morbid</strong>ities, and quality <strong>of</strong> life.<br />
Nonsurgical treatments for <strong>morbid</strong> <strong>obesity</strong> have significant<br />
limitations including minimal total weight loss, little<br />
or no effect on co<strong>morbid</strong>ities and quality <strong>of</strong> life, and lack<br />
<strong>of</strong> sustainment over time. Bariatric surgery, on the other<br />
hand, <strong>of</strong>fers greater and longer-lasting weight loss 54 and<br />
better improvement in clinically relevant outcomes. 21,22<br />
Sackett wrote that evidence-based medicine is “the<br />
integration <strong>of</strong> the best research evidence with clinical
expertise and patient values.” 55 Because we now have<br />
access to a significant body <strong>of</strong> literature on the management<br />
<strong>of</strong> <strong>obesity</strong>, we can initiate evidence-based discussions<br />
with patients, which may help to create a treatment plan<br />
aimed at reducing the <strong>morbid</strong>ity associated with severe<br />
<strong>obesity</strong>. For the patient with <strong>morbid</strong> <strong>obesity</strong>, this will likely<br />
include a discussion about bariatric surgery. ■<br />
REFERENCES<br />
1. Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in<br />
<strong>obesity</strong> among US adults, 1999-2000. JAMA. 2002;288:1723-1727.<br />
2. Mokdad AH, Ford ES, Bowman BA, Dietz WH, Vinicor F, Bales VS, Marks<br />
JS. Prevalence <strong>of</strong> <strong>obesity</strong>, diabetes, and <strong>obesity</strong>-related health risk factors,<br />
2001. JAMA. 2003;289:76-79.<br />
3. Wang Y, Monteiro C, Popkin BM. Trends <strong>of</strong> <strong>obesity</strong> and underweight in<br />
older children and adolescents in the United States, Brazil, China, and Russia.<br />
Am J Clin Nutr. 2002;75:971-977.<br />
4. World Health Organization. World Health Report 2002. Available at:<br />
http://www.who.int/whr/2002/en/. Accessed November 6, 2004.<br />
5. Sinha R, Anderson DE, McDonald SS, Greenwald P. Cancer risk and diet in<br />
India. J Postgrad Med. 2003;49:222-228.<br />
6. National Institutes <strong>of</strong> Health. Clinical guidelines on the identification, evaluation,<br />
and treatment <strong>of</strong> overweight and <strong>obesity</strong> in adults: <strong>The</strong> evidence<br />
report. Bethesda, MD: US Department <strong>of</strong> Health and Human Services; 1998.<br />
7. Ogden CL, Flegal KM, Carroll MD, Johnson CL. Prevalence, and trends in<br />
overweight among US children and adolescents, 1999-2000. JAMA.<br />
2002;288:1728-1732.<br />
8. Freedman DS, Khan LK, Serdula MK, Galuska DA, Dietz WH. Trends and<br />
correlates <strong>of</strong> class 3 <strong>obesity</strong> in the United States from 1990 through 2000.<br />
JAMA. 2002;288:1758-1761.<br />
9. Sturm R. Increases in clinically severe <strong>obesity</strong> in the United States, 1986-<br />
2000. Arch Intern Med. 2003;163:2146-2148.<br />
10. Field AE, Coakley EH, Must A, et al. Impact <strong>of</strong> overweight on the risk <strong>of</strong><br />
developing common chronic diseases during a 10-year period. Arch Intern<br />
Med. 2001;161:1581-1586.<br />
11. Must A, Spadano J, Coakley EH, Field AE, Colditz G, Dietz WH. <strong>The</strong> disease<br />
burden associated with overweight and <strong>obesity</strong>. JAMA. 1999;282:1523-<br />
1529.<br />
12. Anderson JW, Konz EC. Obesity and disease management: Effects <strong>of</strong> weight<br />
loss on co<strong>morbid</strong> conditions. Obes Res. 2001;9(suppl 4):326S-334S.<br />
13. Allison DB, Fontaine KR, Manson JE, Stevens J, VanItallie TB. Annual<br />
deaths attributable to <strong>obesity</strong> in the United States. JAMA. 1999;282:1530-<br />
1538.<br />
14. Calle EE, Thun MJ, Petrelli JM, Rodriguez C, Heath CW Jr. Body-mass index<br />
and mortality in a prospective cohort <strong>of</strong> US adults. N Engl J Med.<br />
1999;341:1097-1105.<br />
15. Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes <strong>of</strong> death in<br />
the United States, 2000. JAMA. 2004;291:1238-1245.<br />
16. Fontaine KR, Redden DT, Wang C, Westfall AO, Allison DB. Years <strong>of</strong> life lost<br />
due to <strong>obesity</strong>. JAMA. 2003;289:187-193.<br />
17. Beasley JW. Obesity and years <strong>of</strong> life lost. Letter to the editor. JAMA.<br />
2003;289:1777.<br />
18. Gregg EW, Gerz<strong>of</strong>f, RB, Thompson TJ, Williamson DF. Intentional weight<br />
loss and death in overweight and obese US adults 35 years <strong>of</strong> age and older.<br />
Ann Intern Med. 2003;138:383-390.<br />
19. Stevens J, et al. Sensitivity and specificity <strong>of</strong> anthropometrics for the prediction<br />
<strong>of</strong> diabetes in a biracial cohort. Obes Res. 2001;9:696-705.<br />
20. Schauer PR, et al. Effect <strong>of</strong> laparoscopic Roux-en-Y gastric bypass on type 2<br />
diabetes mellitus. Ann Surg. 2003;238:467-484.<br />
21. Pories WJ, MacDonald, KG Jr, Morgan EJ, Sinha MK, et al. Surgical treatment<br />
<strong>of</strong> <strong>obesity</strong> and its effect on diabetes: 10-year follow-up. Am J Clin Nutr.<br />
1992;55:582-585.<br />
22. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic<br />
review and meta-analysis. JAMA. 2004;292:1724-1737.<br />
23. Sugerman HJ, Wolfe LG, Sica DA, Clore JN. Diabetes and hypertension in<br />
severe <strong>obesity</strong> and effects <strong>of</strong> gastric bypass-induced weight loss. Ann Surg.<br />
2003;237:751-756.<br />
24. Mahamat A, et al. Body mass index, hypertension, and 5-year coronary heart<br />
disease incidence in middle aged men: the PRIME study. J Hypertens.<br />
2003;21:519-524.<br />
25. Wilson PWF, D’Agostino RB, Sullivan L, Parise H, Kannel WB. Overweight<br />
and <strong>obesity</strong> as determinants <strong>of</strong> cardiovascular risk: the Framingham experience.<br />
Arch Intern Med. 2002;162:1867-1872.<br />
26. Williamson DF, Pamuk E, Thun M, Flanders D, Byers T, Heath C.<br />
Prospective study <strong>of</strong> intentional weight loss and mortality in overweight<br />
THE JOURNAL OF<br />
FAMILY<br />
PRACTICE<br />
white men aged 40-64 years. Am J Epidemiol. 1999;149:491-503.<br />
27. Mulrow CD, Chiquette E, Angel L, et al. Dieting to reduce body weight for<br />
controlling hypertension in adults. In: <strong>The</strong> Cochrane Library. Issue 4.<br />
Chichester, UK: John Wiley & Sons, Ltd; 2004.<br />
28. Smith MB. Randomized placebo-controlled trial <strong>of</strong> long-term treatment with<br />
sibutramine in mild to moderate <strong>obesity</strong>. J Fam Pract. 2001;50:505-512.<br />
29. Wirth A, Krause J. Long-term weight loss with sibutramine: a randomized<br />
controlled trial. JAMA. 2001;286:1331-1339.<br />
30. Sjörström CD, Lissner L, Wedel H, Sjöström L. Reduction in incidence <strong>of</strong> diabetes,<br />
hypertension and lipid disturbances after intentional weight loss<br />
induced by bariatric surgery: the SOS intervention study. Obes Res.<br />
1999;7:477-484.<br />
31. Stürmer T, Gunther KP, Brenner H. Obesity, overweight and patterns <strong>of</strong><br />
osteoarthritis: the Ulm Osteoarthritis Study. J Clin Epidemiol. 2000;53:307-<br />
313.<br />
32. Wendelboe AM, Hegmann KT, Biggs JJ, et al. Relationships between body<br />
mass indices and surgical replacements <strong>of</strong> knee and hip joints. Am J Prev<br />
Med. 2003;25:290-295.<br />
33. Messier SP, Loeser RF, Miller GD, et al. Exercise and dietary weight loss in<br />
overweight and obese older adults with knee osteoarthritis: the Arthritis,<br />
Diet, and Activity Promotion Trial. Arthritis Rheum. 2004;50:1501-1510.<br />
34. Huang MH, Chen CH, Chen TW, et al. <strong>The</strong> effects <strong>of</strong> weight reduction on<br />
the rehabilitation <strong>of</strong> patients with knee osteoarthritis and <strong>obesity</strong>. Arthritis<br />
Care Res. 2000;13:398-405.<br />
35. Flugsrud GB, Nordsletten L, Espehaug B, Havelin LI, Meyer HE. Weight<br />
change and the risk <strong>of</strong> total hip replacement. Epidemiology. 2003;14:578-<br />
584.<br />
36. Sjörström L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes and cardiovascular<br />
risk factors 10 years after bariatric surgery. N Engl J Med.<br />
2004;351:2683-2693.<br />
37. Dixon JB, Dixon ME, O’Brien PE. Quality <strong>of</strong> life after Lap-Band placement:<br />
influence <strong>of</strong> time, weight loss and co<strong>morbid</strong>ities. Obes Res. 2001;11:713-<br />
721.<br />
38. Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJN. Overweight, <strong>obesity</strong>,<br />
and mortality from cancer in a prospectively studied cohort <strong>of</strong> US adults.<br />
N Engl J Med. 2003;348:1625-1638.<br />
39. Calle EE, Thun MJ. Obesity and cancer. Oncogene. 2004;23:6365-6378.<br />
40. Trentham-Dietz A, Newcomb, PA, Egan KM, et al. Weight change and risk<br />
<strong>of</strong> postmenopausal breast cancer (United States). Cancer Causes Control.<br />
2000;11:533-542.<br />
41. Parker ED, Folsom AR. Intentional weight loss and incidence <strong>of</strong> <strong>obesity</strong>related<br />
cancers: the Iowa Women’s Health Study. Int J Obes. 2003;27:1447-<br />
1452.<br />
42. Wolf AM. Economic outcomes <strong>of</strong> the obese patient. Obes Res.<br />
2002;10(suppl 1):58S-62S.<br />
43. Kolotkin RL, Crosby RD, Williams GR, Hartley GG, Nicol S. <strong>The</strong> relationship<br />
between health-related quality <strong>of</strong> life and weight loss. Obes Res.<br />
2001;9:564-571.<br />
44. Van Gemert WG, Van Dielen F, Soeters PB, Greve JW. Quality <strong>of</strong> life before<br />
and after weight-reducing surgery and cost-effectiveness analysis. In: Dietal<br />
M, Cowan SM, eds. Update: Surgery for the <strong>morbid</strong>ly obese patient.<br />
Toronto, Ont: FD communications; 2000:595-602.<br />
45. Puhl R, Brownell KD. Bias, discrimination, and <strong>obesity</strong>. Obes Res.<br />
2001;9:788-805.<br />
46. Larsson U, Karlsson J, Sullivan M. Impact <strong>of</strong> overweight in <strong>obesity</strong> on healthrelated<br />
quality <strong>of</strong> life: a Swedish population study. Int J Obes. 2002;26:417-424.<br />
47. Jain A. What Works for Obesity? A Summary <strong>of</strong> the Research Behind<br />
Obesity Interventions. London, England: BMJ Publishing Group; April<br />
2004.<br />
48. Pirozzo S, Summerbell C, Cameron C, Glasziou P. Advice on low-fat diets for<br />
<strong>obesity</strong>. In: <strong>The</strong> Cochrane Library. Issue 4, 2004. Oxford, England: update<br />
s<strong>of</strong>tware.<br />
49. Padwal R, Li SK, Lau DCW. Long-term pharmacotherapy for <strong>obesity</strong> and<br />
overweight (Cochrane Review). In: <strong>The</strong> Cochrane Library. Issue 3.<br />
Chichester, UK: John Wiley & Sons, Ltd; 2004.<br />
50. Ernst E. Acupuncture/acupressure for weight reduction? A systematic review.<br />
Wien Klin Wochenschr. 1997;109:60-62.<br />
51. Allison DB, Faith MS. Hypnosis as an adjunct to cognitive-behavioral psychotherapy<br />
for <strong>obesity</strong>: a meta analytical reappraisal. J Consult Clin Psychol.<br />
1995;54:513-515.<br />
52. Pittler MH, Ernst E. Dietary supplements for body-weight reduction: a systematic<br />
review. Am J Clin Nutr. 2004;79:529-536.<br />
53. Poston WS 2nd, Foreyt JP. Successful management <strong>of</strong> the obese patient. Am<br />
Fam Phys. 2000;61:3615-3622.<br />
54. Colquitt J, Clegg A, Sidhu M, Royle P. Surgery for <strong>morbid</strong> <strong>obesity</strong>. (Cochrane<br />
Review). In: <strong>The</strong> Cochrane Library. Issue 3. Chichester, UK: John Wiley &<br />
Sons, Ltd; 2004.<br />
55. Sackett DL, Straus SE, Richardson WS, Haynes RB. Evidence-based medicine:<br />
How to practice and teach EBM, second edition. London, England:<br />
Churchill Livingstone; 2000.<br />
March 2005 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> 9
<strong>Management</strong> <strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>: <strong>The</strong> role <strong>of</strong> bariatric surgery<br />
Surgical options<br />
Henry Buchwald, MD, PhD<br />
Pr<strong>of</strong>essor, Department <strong>of</strong> Surgery<br />
Owen H. and Sarah Davidson Wangensteen Chair<br />
in Experimental Surgery Emeritus<br />
University <strong>of</strong> Minnesota Medical School<br />
Minneapolis, Minn<br />
<strong>The</strong> weight loss that occurs after bariatric surgery<br />
is achieved and maintained through restriction<br />
<strong>of</strong> food intake, malabsorption <strong>of</strong> food, or both.<br />
Ideally, eating behavior will be modified after surgery—patients<br />
are likely to consume smaller quantities<br />
<strong>of</strong> food more slowly.<br />
<strong>The</strong> number <strong>of</strong> bariatric procedures performed<br />
around the world has grown markedly and probably<br />
will increase exponentially as surgery is recognized as an<br />
effective treatment. Its risks are decreasing, and its benefits<br />
include the reduction, if not elimination, <strong>of</strong> many<br />
co<strong>morbid</strong>ities. A 31-country survey performed by the<br />
International Federation for the Surgery <strong>of</strong> Obesity<br />
(IFSO) showed that the worldwide frequency <strong>of</strong><br />
bariatric surgery has increased from 40,000 in 1998 to<br />
more than 146,000 in 2003. 1<br />
In the United States, about 103,000 bariatric operations<br />
were performed in 2003, and more than 140,000<br />
were performed in 2004. France, which reported<br />
12,000 procedures in 2003, ranks second in frequency,<br />
followed by Brazil and Italy. <strong>The</strong> United States also has<br />
the greatest number <strong>of</strong> bariatric surgeons (850, according<br />
to the 2003 IFSO survey), followed by France, Italy,<br />
and the United Kingdom, with about 200 each.<br />
Weight loss after surgery<br />
For practical and ethical reasons, it is currently impossible<br />
to perform a true randomized controlled trial (RCT)<br />
<strong>of</strong> bariatric surgery; that is, a blinded study in which<br />
patients are randomized to surgery or placebo. Most<br />
studies have been RCTs that compared different surgical<br />
procedures or surgery to nonsurgical management<br />
(drugs and/or diet or no treatment), nonrandomized<br />
controlled studies <strong>of</strong> surgery vs nonsurgery, and<br />
prospective cohort studies <strong>of</strong> surgery vs nonsurgery. In<br />
10 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> March 2005<br />
recent years, several systematic reviews <strong>of</strong> these data<br />
have been completed, permitting an assessment <strong>of</strong> the<br />
effects <strong>of</strong> bariatric surgery on weight loss, co<strong>morbid</strong>ities,<br />
and quality <strong>of</strong> life.<br />
Analysis <strong>of</strong> pooled data from randomized controlled<br />
trials <strong>of</strong> bariatric surgery in the United States, United<br />
Kingdom, and Canada found dramatic weight reduction<br />
across the board. 2 In 5 US trials reviewed by the National<br />
Institutes <strong>of</strong> Health, mean weight loss was 76 kg (range,<br />
9.7-159) after 1 to 4 years. 2 Mean weight loss in a UK<br />
National Health Service review <strong>of</strong> 6 trials was 45.1 kg<br />
(range, 9.7-57.9) after 1 to 4 years, while mean weight<br />
loss in 4 randomized trials and 1 prospective cohort<br />
study reviewed by the Canadian Task Force on<br />
Preventive Health Care was 29.9 kg (range, 17-45.5)<br />
after 2 to 5 years. 2 Wound infection, gastric leaks, and<br />
other complications were reported, and up to 25% <strong>of</strong><br />
patients required revisional procedures within 5 years.<br />
However, operative mortality was extremely low (
loss <strong>of</strong> 20 kg (CI, 18-22) in surgical patients and <strong>of</strong> 0.7<br />
kg (CI, -0.8 to 2.2) in controls. 4<br />
Operative procedures<br />
Since bariatric surgery is the only broadly successful treatment<br />
for <strong>morbid</strong> <strong>obesity</strong>, physicians should familiarize<br />
themselves with commonly used operative procedures<br />
and their impact on the co<strong>morbid</strong>ities associated with<br />
extreme <strong>obesity</strong>. <strong>The</strong>re are 4 main categories <strong>of</strong> procedures:<br />
malabsorptive (eg, biliopancreatic diversion, duodenal<br />
switch), malabsorptive/restrictive (eg, Roux-en-Y<br />
gastric bypass), restrictive (eg, vertical banded gastroplasty,<br />
gastric banding), and neither malabsorptive nor<br />
restrictive (eg, gastric or vagal pacing). Despite their relative<br />
complexity, all can be performed laparoscopically, as<br />
well as by open abdominal surgery. Recently, robotics<br />
have been introduced into laparoscopic bariatric surgery.<br />
Malabsorptive procedures<br />
<strong>The</strong> current generation <strong>of</strong> malabsorptive procedures is<br />
descended from the jejunoileal bypass, the first operation<br />
to be performed for the purpose <strong>of</strong> weight reduction.<br />
5,6 Introduced in 1953-1954 by Varco and the team<br />
<strong>of</strong> Kremen, Linner, and Nelson, the jejunoileal bypass<br />
was highly effective for weight loss, but had unacceptably<br />
high <strong>morbid</strong>ity. 5,6 Gas-bloat syndrome, steatorrhea,<br />
electrolyte imbalance, hepatic fibrosis and failure,<br />
nephrolithiasis, and impaired mentation were among<br />
the complications that led to gradual abandonment <strong>of</strong><br />
the jejunoileal bypass in favor <strong>of</strong> the gastric bypass in<br />
the 1970s and 1980s.<br />
Newer malabsorptive procedures such as the biliopancreatic<br />
diversion and the duodenal switch share a<br />
key feature that averts most <strong>of</strong> these complications<br />
(FIGURE 2). No segment <strong>of</strong> the intestine is allowed to<br />
remain stagnant and become a breeding ground for bacteria.<br />
<strong>The</strong> surgeon creates an enteric limb for transit <strong>of</strong><br />
food and a biliopancreatic limb for transit <strong>of</strong> bile and<br />
pancreatic juice. <strong>The</strong>se join in a common channel where<br />
digestion and nutrient absorption take place. <strong>The</strong> biliopancreatic<br />
diversion is also known as the Scopinaro<br />
procedure after Nicola Scopinaro, its creator and<br />
staunchest advocate. 6 Since introducing the procedure in<br />
1979, Scopinaro has made a number <strong>of</strong> modifications.<br />
<strong>The</strong> current operation consists <strong>of</strong> a horizontal partial<br />
gastrectomy with closure <strong>of</strong> the duodenal stump, gastrojejunostomy<br />
with a long Roux limb, and anastomo-<br />
FIGURE 1<br />
Weight (kg)<br />
130<br />
120<br />
110<br />
100<br />
90<br />
80<br />
70<br />
THE JOURNAL OF<br />
FAMILY<br />
PRACTICE<br />
Weight change in the<br />
Swedish Obese Subjects Study<br />
Controls (n=1,031)<br />
Gastric banding (n=255)<br />
Vertical banded<br />
gastroplasty (n=834)<br />
Adapted from Sjöström et al.<br />
Gastric bypass (n=88)<br />
8<br />
0<br />
-2 0 2<br />
Years<br />
4 6<br />
sis <strong>of</strong> the long biliopancreatic limb to the Roux limb to<br />
create a short (50 cm) common channel. Potential complications<br />
include malodorous diarrhea, flatulence, anemia,<br />
stomal ulcers, bone demineralization, and protein<br />
malabsorption.<br />
<strong>The</strong> duodenal switch was pioneered by Marceau<br />
and colleagues (1993) and Hess and Hess (1998). 6 This<br />
is a complicated procedure in which a greater curvature<br />
sleeve gastrectomy is performed to leave a stomach with<br />
a capacity <strong>of</strong> approximately 100 mL, the duodenum is<br />
divided, and the enteric limb is anastomosed to the postpyloric<br />
duodenum. Like biliopancreatic diversion, the<br />
duodenal switch may be associated with diarrhea, flatulence,<br />
iron malabsorption, and calcium and protein<br />
malabsorption. <strong>The</strong>se can be reduced or avoided by the<br />
use <strong>of</strong> mild antidiarrheal agents and mineral supplements,<br />
and maintenance <strong>of</strong> a diet containing 65 to 80<br />
gm <strong>of</strong> protein per day.<br />
Malabsorptive/restrictive procedures<br />
<strong>The</strong> first gastric bypass procedure was developed by<br />
Mason and Ito in the mid-1960s, with subsequent variations<br />
by Alden, Griffen, and associates; Linner and<br />
Drew; Torres and Oca; and others. 6 All combine intestinal<br />
malabsorption with gastric restriction, but rely<br />
March 2005 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> 11
<strong>Management</strong> <strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>: <strong>The</strong> role <strong>of</strong> bariatric surgery<br />
FIGURE 2<br />
Biliopancreatic<br />
diversion<br />
Malabsorptive procedures<br />
Biliopancreatic diversion<br />
with duodenal switch<br />
primarily on the latter for weight loss. <strong>The</strong> Roux-en-Y<br />
bypass involves construction <strong>of</strong> a small upper gastric<br />
pouch (currently 20 mL or less) that empties food into the<br />
small intestine through a Roux limb gastrojejunostomy<br />
(FIGURE 3). <strong>The</strong> degree <strong>of</strong> malabsorption is determined<br />
by the extent <strong>of</strong> the bypass, which at a minimum<br />
includes the distal stomach, the duodenum, and the first<br />
segment <strong>of</strong> the jejunum.<br />
A modification known as the long-limb or distal<br />
Roux-en-Y bypass, involving a long Roux limb and a<br />
long bypassed limb that join to create a short common<br />
channel, was designed by Torres and Oca (and later<br />
12 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> March 2005<br />
FIGURE 3<br />
Malabsorptive/restrictive procedure<br />
Roux-en-Y<br />
gastric bypass<br />
Brolin) to further enhance malabsorption. 6 It may cause<br />
severe vitamin, mineral, and nutrient malnutrition and<br />
should be reserved for patients who are super-obese or<br />
have failed primary Roux-en-Y bypass.<br />
While considerably safer than the jejunoileal<br />
bypass, the Roux-en-Y gastric bypass is not without<br />
problems. Postoperative complications include the<br />
“dumping” syndrome, iron deficiency anemia, and lifelong<br />
vitamin B 12 malabsorption. Should the bypassed<br />
distal stomach become obstructed, the resulting dilation<br />
can lead to gastric rupture—a life-threatening complication.<br />
<strong>The</strong> procedure also deprives care providers <strong>of</strong> the<br />
ability to visualize the distal stomach and duodenum.<br />
Restrictive procedures<br />
In the 1970s and 1980s, bariatric surgery was simplified<br />
by introduction <strong>of</strong> a number <strong>of</strong> purely restrictive<br />
gastric operations: gastroplasty, gastric partitioning,<br />
banded or ringed vertical gastroplasty (partial gastric<br />
partitioning at the proximal gastric segment), and<br />
gastric banding (placement <strong>of</strong> an adjustable or nonadjustable<br />
band around the stomach to create a small<br />
pouch) (FIGURE 4). <strong>The</strong>se are the least invasive <strong>of</strong><br />
bariatric procedures because the stomach is not cut or<br />
stapled, no anastomoses are required, and the natural<br />
physiologic passage <strong>of</strong> food is not altered.<br />
Patients who eat more than can be tolerated at one
sitting may experience vomiting, especially during the<br />
early postoperative period. Other complications include<br />
the lodging <strong>of</strong> food particles or pills within the band or<br />
ring, and occasional band slippage or erosion. While<br />
<strong>morbid</strong>ity is low, weight loss also may tend to be less<br />
dramatic than with other forms <strong>of</strong> bariatric surgery.<br />
New procedures<br />
In the 1990s, procedures that do not rely on either malabsorption<br />
or restriction were introduced into bariatric<br />
surgery. Gastric and vagal pacing have been tested in<br />
animals and in preliminary human trials. 6 A hypothesis<br />
behind this approach is that induced gastric paresis<br />
and/or afferent vagal central nervous system stimulation<br />
will produce satiety and, as a consequence, weight loss.<br />
<strong>The</strong> electrical stimulation procedures are simple and<br />
easy to perform, but it is too early to determine their<br />
place in the armamentarium <strong>of</strong> bariatric surgery.<br />
Frequency <strong>of</strong> surgery by type<br />
Gastric bypass operations account for 65% <strong>of</strong> bariatric<br />
procedures performed worldwide, according to the<br />
IFSO survey. 1 <strong>The</strong> most common procedure in the<br />
world is laparoscopic Roux-en-Y gastric bypass (26%<br />
<strong>of</strong> all operations), followed by laparoscopic gastric<br />
banding (24%), open gastric bypass (23%), laparoscopic<br />
long-limb gastric bypass (9%), open long-limb gastric<br />
bypass (7%), vertical banded gastroplasty (5%), and<br />
biliopancreatic diversion/duodenal switch (5%).<br />
About 57% <strong>of</strong> bariatric procedures in the United<br />
States are performed laparoscopically, compared with<br />
63% worldwide. Similarly, gastric banding is performed<br />
less frequently than gastric bypass in the United States;<br />
it was not approved by the US Food and Drug<br />
Administration until the middle <strong>of</strong> 2001. About 20,000<br />
gastric bands were placed from 2001 to 2003 and<br />
another 40,000 were expected in 2004.<br />
Is there a clear winner?<br />
<strong>The</strong> heterogeneity <strong>of</strong> the bariatric surgery data makes it<br />
difficult to draw conclusions about the superiority <strong>of</strong> one<br />
procedure over another. Studies differ with regard to procedural<br />
variations, measures <strong>of</strong> weight change, and length<br />
<strong>of</strong> follow-up. Degree <strong>of</strong> weight loss must be balanced<br />
against operative risk, short- and long-term <strong>morbid</strong>ity,<br />
and the need for later revisional surgery. Moreover, while<br />
later <strong>morbid</strong>ity is heavily procedure-dependent, operative<br />
FIGURE 4<br />
Vertical banded<br />
gastroplasty<br />
Gastric banding<br />
THE JOURNAL OF<br />
FAMILY<br />
PRACTICE<br />
Restrictive procedures<br />
risk depends largely on the skill <strong>of</strong> the surgeon and may<br />
vary for patients undergoing the same operation.<br />
In the Cochrane review previously cited, 3 gastric<br />
bypass was associated with significantly greater weight<br />
loss and fewer revisions or conversions than gastroplasty,<br />
but also with more side effects and postoperative<br />
deaths. Greater weight loss, and fewer side effects and<br />
reoperations, occurred with adjustable gastric banding<br />
than with vertical banded gastroplasty. Weight loss was<br />
similar with open and laparoscopic procedures; however,<br />
the laparoscopic approach had fewer serious complications.<br />
Laparoscopic surgery was associated with<br />
March 2005 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> 13
<strong>Management</strong> <strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>: <strong>The</strong> role <strong>of</strong> bariatric surgery<br />
TABLE 1<br />
Meta-analysis <strong>of</strong> changes in weight and<br />
<strong>obesity</strong>-related co<strong>morbid</strong>ities after bariatric surgery *<br />
reduced blood loss, fewer intensive care unit stays,<br />
reduced length <strong>of</strong> hospital stay, reduced days to return<br />
to activities <strong>of</strong> daily living, and reduced days <strong>of</strong> return<br />
to work. Because all studies included in the Cochrane<br />
analysis had the potential for significant bias, the investigators<br />
cautioned that these results should be viewed as<br />
tentative—the relative safety and efficacy <strong>of</strong> different<br />
bariatric procedures remain to be determined.<br />
Impact on co<strong>morbid</strong>ities<br />
<strong>The</strong> effects <strong>of</strong> bariatric surgery on <strong>obesity</strong> co<strong>morbid</strong>ities<br />
are rapid and pr<strong>of</strong>ound (TABLE 1). In a landmark 1995<br />
article, Pories et al reported achievement <strong>of</strong> long-term<br />
14 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> March 2005<br />
Mean change/value P Value<br />
Weight loss Absolute weight 40 kg
ing surgery. Gastric bypass also corrected or alleviated<br />
other co<strong>morbid</strong>ities <strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>, including hypertension,<br />
obstructive sleep apnea, cardiopulmonary failure,<br />
arthritis, and infertility. 7<br />
In the SOS study, incidence <strong>of</strong> diabetes was reduced<br />
32-fold in surgical patients relative to controls at 2<br />
years. At 8 years, there was still a 5-fold reduction in<br />
diabetes incidence. 4 Incidence <strong>of</strong> hypertension was<br />
reduced 2.6-fold in surgical patients relative to controls<br />
at 2 years. However, by 8 years the surgical patients’<br />
blood pressure had reverted to control values despite<br />
maintenance <strong>of</strong> a 16% weight reduction. 4,8,9<br />
Buchwald and colleagues recently conducted a systematic<br />
review <strong>of</strong> published observational and interventional<br />
trials involving bariatric surgery. 10 A total <strong>of</strong> 134<br />
studies (5 randomized controlled trials, 28 nonrandomized<br />
controlled trials or series with comparison groups,<br />
and 101 uncontrolled case series) that included 22,094<br />
patients were analyzed to determine the impact <strong>of</strong> specific<br />
bariatric surgical procedures on weight loss, operative<br />
mortality outcome, and 4 <strong>obesity</strong> co<strong>morbid</strong>ities<br />
(diabetes, hyperlipidemia, hypertension, and obstructive<br />
sleep apnea). Results are summarized in Table 1.<br />
For purposes <strong>of</strong> analysis, surgical procedures were<br />
grouped into 5 main categories: (1) gastric banding, (2)<br />
gastric bypass (this category consisted principally <strong>of</strong><br />
Roux-en-Y variations but included all procedures with<br />
a gastric bypass component, such as gastroplasty with<br />
gastric bypass and banding with gastric bypass), (3) gastroplasty,<br />
(4) biliopancreatic diversion or duodenal<br />
switch, and (5) mixed or other. A random-effects model<br />
was used. Weight loss was reported as the mean percentage<br />
<strong>of</strong> excess weight loss; changes in absolute<br />
weight (kg), body mass index (BMI), and percentage <strong>of</strong><br />
initial weight were also reported where appropriate.<br />
<strong>The</strong> baseline mean BMI for 16,944 patients was<br />
46.9 kg/m 2 (range, 32.3-68.8). Mean percentage <strong>of</strong><br />
excess weight loss was 61.2% (95% CI, 58.1-64.4) for<br />
all patients. Mean percentage excess weight loss by procedure<br />
was: gastric banding, 47.5%; gastric bypass,<br />
61.6%; gastroplasty, 68.2%; biliopancreatic diversion<br />
or duodenal switch, 70.1%. Operative mortality in the<br />
first 30 days was 0.1% for the purely restrictive procedures,<br />
0.5% for gastric bypass, and 1.1% for biliopancreatic<br />
diversion or duodenal switch.<br />
Diabetes was completely resolved in 76.8% <strong>of</strong><br />
patients and resolved or improved in 86.0%. <strong>The</strong>re<br />
FIGURE 5<br />
THE JOURNAL OF<br />
FAMILY<br />
PRACTICE<br />
Risk <strong>of</strong> mortality after bariatric surgery *<br />
(Kaplan Meier analysis)<br />
Percent surviving<br />
100<br />
90<br />
80<br />
70<br />
60<br />
50<br />
Surgery (n=1,035)<br />
Control (n=5,746)<br />
1 2 3 4 5<br />
Years<br />
* Relative risk vs controls, 0.11 (95% CI, 0.04-0.27)<br />
Adapted from Christou et al. 11<br />
P
<strong>Management</strong> <strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>: <strong>The</strong> role <strong>of</strong> bariatric surgery<br />
FIGURE 6<br />
Quality <strong>of</strong> life after bariatric surgery<br />
Mobility<br />
Energy<br />
Pain<br />
Sleep<br />
Social<br />
isolation<br />
Emotional<br />
reaction<br />
0<br />
0<br />
0<br />
0<br />
7<br />
16<br />
13<br />
19<br />
20<br />
30<br />
33<br />
■ Control<br />
■ Surgery<br />
0 10 20 30 40 50 60 70<br />
Best Median score Worst<br />
Shown here are results <strong>of</strong> the Nottingham Health Pr<strong>of</strong>ile I as completed<br />
by 62 patients who underwent vertical banded gastroplasty<br />
or Roux-en-Y gastric bypass and 20 preoperatively <strong>morbid</strong>ly obese<br />
controls. Mean follow-up was 7 years (range, 0.5-14). Adapted<br />
from van Gemert et al. 13<br />
prising, since even a modest (eg, 10%) weight loss can<br />
significantly lower blood pressure. Unlike the case with<br />
type 2 diabetes and hyperlipidemia, the reduction in<br />
hypertension appeared to be independent <strong>of</strong> the type <strong>of</strong><br />
surgery performed.<br />
Obstructive sleep apnea was resolved in 85.7% <strong>of</strong><br />
patients and was resolved or improved in 83.6% <strong>of</strong><br />
patients. <strong>The</strong> extracted studies showed improvements in<br />
oxygen saturation, decreases in arterial carbon dioxide,<br />
and increases in arterial oxygen content. All <strong>of</strong> these<br />
changes resulted primarily from the increase in<br />
diaphragmatic excursion brought about by reduction in<br />
<strong>obesity</strong>-induced intra-abdominal pressure.<br />
Increased life expectancy<br />
Given the scope <strong>of</strong> the reductions in diabetes, hyperlipidemia,<br />
hypertension, obstructive sleep apnea, and other<br />
<strong>obesity</strong> co<strong>morbid</strong>ities that accompany bariatric surgery, it<br />
should come as no surprise that patient life expectancy is<br />
also increased. Christou et al recently conducted a large<br />
observational study to test the hypothesis that surgically<br />
induced weight loss reduces long-term <strong>morbid</strong>ity, mortality,<br />
and healthcare use in patients with <strong>morbid</strong> <strong>obesity</strong>. 11<br />
None <strong>of</strong> the 1,035 surgery patients or 5,746 age- and gender-matched<br />
severely obese controls had medical conditions<br />
other than <strong>morbid</strong> <strong>obesity</strong> at study entry. Mean follow-up<br />
was 5 years (range, 1-16). Bariatric surgery (Rouxen-Y<br />
gastric bypass) resulted in a mean percentage excess<br />
16 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> March 2005<br />
63<br />
weight loss <strong>of</strong> 67.1% (P
have shown similar increases in employment and/or<br />
income after bariatric surgery. It should be noted that<br />
US law prohibits employment discrimination based on<br />
physical attributes that do not affect job performance.<br />
In both <strong>of</strong> the studies cited above, postoperative<br />
quality <strong>of</strong> life tended to decrease somewhat over the long<br />
term. Since HRQOL correlates with the degree <strong>of</strong> weight<br />
loss, this may simply reflect the well-known tendency <strong>of</strong><br />
bariatric surgery patients to regain a modest portion <strong>of</strong><br />
their lost weight after 2 years. In addition, it has been<br />
suggested that patients derive considerable psychological<br />
support from their postoperative visits and may experience<br />
an emotional downturn when those visits cease.<br />
At no time, however, did quality <strong>of</strong> life drop to the<br />
level <strong>of</strong> obese controls. Van Gemert and colleagues<br />
emphasized that this remained true even in patients who<br />
experienced significant surgical complications such as<br />
stoma stenosis or band erosion or disruption. Noting<br />
that other studies have also found surgical complications<br />
to be a nonissue, they commented: “<strong>The</strong> fact that<br />
patients with complications nevertheless experienced a<br />
significant improvement in quality <strong>of</strong> life compared with<br />
the control group highlights the severity <strong>of</strong> the mental<br />
and physical suffering ... before surgery. Apparently,<br />
these patients prefer a nonobese state with surgical complications<br />
over an obese state.” 13<br />
Matching patient and procedure<br />
A <strong>morbid</strong>ly obese patient may be broadly matched to<br />
the most suitable bariatric procedure on the basis <strong>of</strong> several<br />
variables: 14<br />
1) BMI. Some bariatric procedures induce more<br />
weight loss than others. Patients with the highest BMIs<br />
may be guided to procedures that achieve the most<br />
weight loss (eg, biliopancreatic diversion with duodenal<br />
switch, long-limb Roux-en-Y gastric bypass).<br />
2) Age. Older patients (>40 years) may be candidates<br />
for the more definitive procedures (eg, biliopancreatic<br />
diversion, duodenal switch, and long-limb Rouxen-Y<br />
gastric bypass). Despite their complexity, increased<br />
operative risk, and long-term surgically induced <strong>morbid</strong>ity,<br />
such procedures have a lower risk for failure and<br />
need for reoperation.<br />
3) Gender, race, and body habitus. Women may lose<br />
less weight after a given procedure than men. Similarly,<br />
African Americans and possibly Hispanics tend to lose<br />
less weight after a given procedure than Caucasians.<br />
Central (as opposed to peripheral) <strong>obesity</strong> in men and<br />
android (as opposed to gynecoid) <strong>obesity</strong> in women<br />
THE JOURNAL OF<br />
FAMILY<br />
PRACTICE<br />
appear to be associated with more co<strong>morbid</strong>ities that<br />
increase operative risk.<br />
Patients in whom combined gender, race, and body<br />
habitus is ‘unfavorable’ are candidates for a more definitive<br />
operation. If combined status is ‘favorable,’ a simpler<br />
operation (eg, gastric banding) may be appropriate.<br />
4) Co<strong>morbid</strong>ities. <strong>The</strong> patient with few serious preoperative<br />
co<strong>morbid</strong>ities clearly has a better long-term<br />
prognosis than the patient with numerous serious<br />
co<strong>morbid</strong>ities. <strong>The</strong>y can be guided to a simpler, faster<br />
operation, despite the increased risk for subsequent revisional<br />
surgery. When co<strong>morbid</strong>ities predict a poor longterm<br />
prognosis, a more definitive operation with a<br />
lower risk for reoperation is recommended.<br />
Conclusion<br />
Morbidly obese patients who elect to undergo bariatric<br />
surgery experience significant reductions not only <strong>of</strong><br />
weight but also <strong>of</strong> <strong>obesity</strong> co<strong>morbid</strong>ities, including diabetes,<br />
hyperlipidemia, hypertension, and obstructive<br />
sleep apnea, with resultant improved life expectancy.<br />
<strong>The</strong> quality <strong>of</strong> life <strong>of</strong> these patients also has been shown<br />
to improve. While bariatric surgical procedures differ<br />
with regard to degree <strong>of</strong> weight loss, short- and longterm<br />
<strong>morbid</strong>ity, and need for revisional surgery, the data<br />
are difficult to interpret. Thus far, no single bariatric procedure<br />
has emerged as clearly superior to others. ■<br />
REFERENCES<br />
1. Buchwald H, Williams SE. Bariatric surgery worldwide 2003. Obes Surg.<br />
2004;14:1157-1164.<br />
2. McTigue KM, Harris R, Hemphill B, Lux L, Sutton S, Bunton AJ, et al.<br />
Screening and interventions for <strong>obesity</strong> in adults: summary <strong>of</strong> the evidence for<br />
the U.S. Preventive Services Task Force. Ann Intern Med. 2003;139:933-949.<br />
3. Colquitt J, Clegg A, Sidhu M, Royle P. Surgery for <strong>morbid</strong> <strong>obesity</strong> (Cochrane<br />
Review). In: <strong>The</strong> Cochrane Library. Issue 3. Chichester, UK: John Wiley &<br />
Sons, Ltd; 2004.<br />
4. Torgerson JS, Sjöström L. <strong>The</strong> Swedish Obese Subjects (SOS) study—rationale<br />
and results. Int J Obes Relat Metab Disord. 2001;25(suppl 1):S2-S4.<br />
5. Buchwald H. Overview <strong>of</strong> bariatric surgery. J Am Coll Surg. 2002;194:367-<br />
375.<br />
6. Buchwald H, Buchwald JN. Evolution <strong>of</strong> operative procedures for the management<br />
<strong>of</strong> <strong>morbid</strong> <strong>obesity</strong> 1950-2000. Obes Surg. 2002;12:705-717.<br />
7. Pories WJ, Swanson MS, MacDonald KG, Long SB, Morris PG, Brown BM,<br />
et al. Who would have thought it? An operation proves to be the most effective<br />
therapy for adult-onset diabetes mellitus. Ann Surg. 1995;222:339-350.<br />
8. Sjöström CD, Peltonen M, Sjöström L. Blood pressure and pulse pressure during<br />
long-term weight loss in the obese: the Swedish Obese Subjects (SOS)<br />
Intervention Study. Obes Res. 2001;9:188-195.<br />
9. Sjöström CD, Lissner L, Wedel H, Sjöström L. Reduction in incidence <strong>of</strong> diabetes,<br />
hypertension and lipid disturbances after intentional weight loss induced<br />
by bariatric surgery: the SOS Intervention Study. Obes Res. 1999;7:477-484.<br />
10. Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, Fahrbach K,<br />
Schoelles K. Bariatric surgery: a systematic review and meta-analysis. JAMA.<br />
2004;292:1724-1737.<br />
11. Christou NV, Sampalis JS, Liberman M, Look D, Auger S, McLean AP, et al.<br />
Surgery decreases long-term mortality, <strong>morbid</strong>ity, and health care use in <strong>morbid</strong>ly<br />
obese patients. Ann Surg. 2004;240:416-423.<br />
12. Kolotkin RL, Meter K, Williams GR. Quality <strong>of</strong> life and <strong>obesity</strong>. Obes Rev.<br />
2001;2:219-229.<br />
13. van Gemert WG, Adang EM, Greve JW, Soeters PB. Quality <strong>of</strong> life assessment<br />
<strong>of</strong> <strong>morbid</strong>ly obese patients: effect <strong>of</strong> weight-reducing surgery. Am J Clin Nutr.<br />
1998;67:197-201.<br />
14. Buchwald H. A bariatric surgery algorithm. Obes Surg. 2002;12:733-746.<br />
March 2005 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> 17
<strong>Management</strong> <strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>: <strong>The</strong> role <strong>of</strong> bariatric surgery<br />
Before and after surgery:<br />
<strong>The</strong> team approach to management<br />
Christopher D. Still, DO<br />
Director, Center for Nutrition and Weight <strong>Management</strong><br />
Geisinger Health Care System<br />
Danville, Pa<br />
Despite impressive outcomes, bariatric surgery<br />
remains the treatment <strong>of</strong> last resort for <strong>morbid</strong><br />
<strong>obesity</strong>. Among the patients who stand to benefit<br />
most are those who 1) have failed attempts at medical<br />
and lifestyle management or have been judged as unlikely<br />
to succeed at them and 2) have a body mass index<br />
(BMI) <strong>of</strong> 40 kg/m 2 or higher or a BMI <strong>of</strong> 35 to 40 kg/m 2<br />
and 1 or more <strong>of</strong> the following co<strong>morbid</strong>ities: diabetes,<br />
hypertension, obstructive sleep apnea, cardiovascular disease,<br />
gastroesophageal reflux disease, degenerative joint<br />
disease, or steatohepatitis (fatty liver) (TABLE 1). 1-3<br />
Amelioration <strong>of</strong> co<strong>morbid</strong>ities should be the primary<br />
goal when contemplating surgery. Indeed, in the severely<br />
obese patient, surgery is the only treatment that has been<br />
shown to cure or ameliorate many <strong>of</strong> these chronic medical<br />
conditions.<br />
In addition to the above criteria, potential candidates<br />
must be well-informed about bariatric surgery,<br />
motivated, and have realistic expectations. Operative<br />
risks must be acceptable, and patients should understand<br />
the ways in which their lives will change after the<br />
operation. <strong>The</strong>y also should be prepared to accept longterm<br />
postsurgical follow-up.<br />
Contraindications to bariatric surgery include<br />
untreated major depression or psychosis, certain personality<br />
disorders (eg, bipolar, schizoaffective), active<br />
alcohol or drug abuse, and noncompliance with preoperative<br />
medical, nutritional, and psychologic management.<br />
Weight-loss surgery is no longer denied to<br />
patients older than 65 years; however, surgical risks may<br />
outweigh benefits in patients over 70 years <strong>of</strong> age.<br />
Bariatric surgery in children and adolescents<br />
remains controversial. Inge et al noted that surgery in<br />
severely obese teenagers (12-18 years) with significant<br />
18 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> March 2005<br />
associated medical conditions (metabolic syndrome,<br />
diabetes, obstructive sleep apnea, reactive airway disease,<br />
steatohepatitis) is safe and has resulted in resolution<br />
<strong>of</strong> co<strong>morbid</strong>ities. 4<br />
Bariatric surgery programs and insurance carriers<br />
invariably insist that patients meet some or all <strong>of</strong> the<br />
above conditions. However, criteria vary from region to<br />
region and state to state, and it is therefore recommended<br />
that the family physician obtain specific inclusion<br />
and exclusion criteria from the patient’s insurance carrier<br />
before making a referral for bariatric surgery.<br />
Preoperative evaluation and care<br />
A comprehensive team approach to patient management<br />
is advocated by most bariatric surgeons and insurance<br />
carriers. An ideal team includes, at a minimum,<br />
representatives from 4 specialties: medicine, nutrition,<br />
psychology/psychiatry, and surgery. 5 <strong>The</strong> team evaluates<br />
the patient, treats conditions that require stabilization<br />
before surgery, and participates in postoperative education<br />
and management. In addition to providing optimal<br />
care in each area <strong>of</strong> expertise, team members should be<br />
able to communicate constructive insights to help the<br />
patient fully appreciate the lifelong lifestyle changes<br />
necessitated by bariatric surgery.<br />
Medical evaluation. To decrease perioperative<br />
<strong>morbid</strong>ity, the medical pr<strong>of</strong>essional whether a family<br />
physician, internist, endocrinologist, gastroenterologist,<br />
or cardiologist should ensure optimal preoperative control<br />
<strong>of</strong> such common co<strong>morbid</strong> conditions as hypertension,<br />
hyperglycemia, dyslipidemia, liver abnormalities,<br />
and sleep disorders. A modest preoperative weight loss<br />
<strong>of</strong> 5% to 10%, which is mandatory in many bariatric
surgery programs, is an effective intervention that can<br />
facilitate significant improvement in many co<strong>morbid</strong>ities.<br />
A thorough physical examination and disease-specific<br />
testing are also recommended. Cardiovascular<br />
assessment, via a stress imaging study such as echocardiography<br />
or nuclear imaging, should be considered in<br />
patients older than 50 years and in those whose <strong>obesity</strong>-related<br />
co<strong>morbid</strong>ities (especially diabetes, hypercholesterolemia,<br />
and hypertension) have been present for<br />
more than 10 years. Administration <strong>of</strong> dobutamine or<br />
adenosine <strong>of</strong>ten is needed to achieve target heart rates in<br />
patients with limited mobility.<br />
A 12-lead EKG should be performed to assess,<br />
among other things, for Q-Tc interval prolongation.<br />
Obese patients with acquired Q-Tc interval prolongation<br />
have increased risk for postoperative malignant<br />
arrhythmias. 6<br />
Sleep apnea is common in the severely obese, but is<br />
<strong>of</strong>ten overlooked or misdiagnosed as depression or<br />
chronic fatigue syndrome. A polysomnogram or, if it is<br />
not available, nocturnal pulse oximetry should be<br />
arranged for patients with loud snoring and documented<br />
apneic episodes, significant daytime somnolence,<br />
and/or early morning headache.<br />
A routine workup that includes complete blood<br />
count, liver function studies, and disease-specific serologies<br />
may be augmented by additional testing, such as<br />
right upper quadrant ultrasound to assess for cholelithiasis<br />
and liver size and steatosis, stool analysis for<br />
Helicobacter pylori antigen, and measurement <strong>of</strong> bone<br />
mineral density.<br />
Preoperative placement <strong>of</strong> an inferior vena cava filter<br />
may be considered in patients with a high risk for<br />
deep vein thrombosis and pulmonary embolism. 7<br />
However, prophylactic use <strong>of</strong> such filters needs to be<br />
validated by prospective, randomized trials. White et al,<br />
for example, found that a vena cava filter did not reduce<br />
the incidence <strong>of</strong> pulmonary embolism and, in patients<br />
with previous pulmonary embolism, it was associated<br />
with a higher incidence <strong>of</strong> rehospitalization for venous<br />
thrombosis. 8<br />
Nutritional evaluation. A registered dietitian or<br />
nutritionist is instrumental in preoperative weight-loss<br />
counseling and, to that end, will assess food intake and<br />
identify eating triggers such as emotional upset.<br />
TABLE 1<br />
THE JOURNAL OF<br />
FAMILY<br />
PRACTICE<br />
Indications and contraindications<br />
for bariatric surgery<br />
Indications<br />
• BMI ≥40 kg/m 2<br />
• BMI ≥35 kg/m 2 and high-risk co<strong>morbid</strong>ity*<br />
• Failed attempts at behavioral and medical therapy †<br />
• Motivated, psychologically stable, realistic<br />
expectations<br />
• Understanding <strong>of</strong> procedure, acceptance <strong>of</strong><br />
operative risks, and commitment to lifelong<br />
behavioral changes<br />
• Commitment to long-term follow-up<br />
• Supportive family environment<br />
Contraindications<br />
• Unacceptable medical risks<br />
• Unresolved alcohol or drug abuse<br />
• Depression, especially involving suicidal ideation<br />
• Hostile, uncooperative patient and/or family<br />
*Cardiopulmonary conditions (eg, sleep apnea, cardiomyopathy,<br />
pickwickian syndrome), type 2 diabetes, joint disease, and body-size<br />
problems that interfere with ambulation and employment.<br />
† Or judged as unlikely to succeed at behavioral and medical<br />
approaches to weight loss.<br />
Adapted from NIH Consensus Development Conference Panel2 and<br />
Mun et al. 3<br />
Counseling also includes repeated review <strong>of</strong> the progressive<br />
dietary stages that the patient will be expected to follow<br />
after surgery. Postoperatively, the dietitian/nutritionist<br />
will monitor the patient for adequate nutrient intake.<br />
Psychologic/psychiatric evaluation. Assessment<br />
<strong>of</strong> mental status should be done by a psychologist or<br />
psychiatrist who is familiar with the psychologic/emotional<br />
abnormalities common to the <strong>morbid</strong>ly obese, as<br />
well as the ramifications <strong>of</strong> bariatric surgery. <strong>The</strong> focus<br />
<strong>of</strong> the mental health examination is on eating disorders/behaviors<br />
(binge eating, in particular), uncontrolled<br />
major depression, and personality disorders.<br />
<strong>The</strong> mental health pr<strong>of</strong>essional also needs to confirm<br />
that the patient has realistic expectations <strong>of</strong> surgery<br />
and fully understands and accepts the postoperative<br />
lifestyle and behavioral changes that will be required.<br />
<strong>The</strong> strength <strong>of</strong> the patient’s support network is another<br />
important issue, given the high rates <strong>of</strong> marital and<br />
March 2005 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> 19
<strong>Management</strong> <strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>: <strong>The</strong> role <strong>of</strong> bariatric surgery<br />
TABLE 2<br />
Potential complications after bariatric surgery<br />
Malabsorptive* Combined † Restrictive ‡<br />
Wound infection ✔ ✔ ✔<br />
Anastomotic leak ✔ ✔ ✔<br />
Stomal stenosis ✔ ✔ ✔<br />
Marginal ulcer ✔ ✔ ✔<br />
Pouch dilation ✔ ✔<br />
Staple failure ✔ ✔<br />
Band migration/erosion ✔<br />
Access port complications ✔<br />
Thromboembolism ✔ ✔ ✔<br />
Pulmonary embolism ✔ ✔ ✔<br />
Nausea/vomiting ✔ ✔ ✔<br />
Gallstones ✔ ✔ ✔<br />
Dumping syndrome ✔<br />
Gastroesophageal reflux disease ✔<br />
Nutrient deficiency ✔ ✔<br />
(iron, vitamin B 12 , calcium, protein)<br />
* Malabsorptive: biliopancreatic diversion, biliopancreatic diversion with duodenal switch.<br />
† Combined: gastric bypass, which has features <strong>of</strong> both intestinal malabsorption and gastric<br />
restriction but relies primarily on restriction for weight loss.<br />
‡ Restrictive: vertical banded gastroplasty, gastric banding.<br />
Adapted from Buchwald et al 21 and McTigue et al. 23<br />
family discord that occur after bariatric surgery.<br />
Surgical evaluation. After the medical, nutritional,<br />
and mental health evaluations have been completed and<br />
adequate metabolic control has been achieved, the<br />
patient is referred to the bariatric surgeon who also<br />
assesses the patient’s motivation and expectations. In<br />
addition, the surgeon discusses the risks and benefits <strong>of</strong><br />
the various surgical approaches after which the most<br />
appropriate technique is selected.<br />
Support groups. Preoperative attendance <strong>of</strong> support-group<br />
meetings is mandatory in most bariatric<br />
programs. Here patients are exposed to other preoperative<br />
candidates as well as to patients who have<br />
undergone weight-loss surgery. Direct contact with<br />
postoperative patients is particularly beneficial, as it<br />
provides firsthand accounts <strong>of</strong> successful and less<br />
than successful adaptation to the behavioral and<br />
lifestyle changes. In larger bariatric programs, separate<br />
support groups <strong>of</strong>ten are created for patients<br />
20 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> March 2005<br />
undergoing malabsorptive procedures<br />
(eg, gastric bypass) and those<br />
assigned to restrictive procedures (eg,<br />
vertical banded gastroplasty,<br />
adjustable lap band) to accommodate<br />
differences in rate <strong>of</strong> weight loss and<br />
behavioral changes.<br />
Perioperative care<br />
Bariatric surgery today is a relatively<br />
safe endeavor with short hospital<br />
stays, the result by and large <strong>of</strong> specific<br />
improvements in surgical technique<br />
and general improvements in the surgical<br />
milieu, such as anesthesia and ventilation.<br />
9 A standard, comprehensive<br />
protocol that is designed to ensure<br />
early ambulation, aggressive pulmonary<br />
toilet, adequate pain control,<br />
and diligent blood glucose control will<br />
decrease perioperative <strong>morbid</strong>ity and<br />
shorten length <strong>of</strong> stay. Depending on<br />
which surgical procedure was performed,<br />
patients are usually discharged<br />
1 to 7 days after surgery.<br />
<strong>The</strong>refore, immediate and frequent<br />
postoperative follow-up by the<br />
bariatric team is essential to ensure<br />
adequate hydration and prompt detection <strong>of</strong> early postoperative<br />
complications (TABLE 2).<br />
Postoperative care<br />
As with preoperative care, postoperative care <strong>of</strong> the<br />
bariatric surgery patient is comprehensive in nature<br />
and best achieved with the team approach.<br />
Postoperative involvement <strong>of</strong> the medical, nutritional,<br />
mental health, and surgical team members maximizes<br />
the likelihood <strong>of</strong> achieving optimal weight loss and resolution<br />
<strong>of</strong> co<strong>morbid</strong>ities.<br />
Early postoperative period<br />
Anastomotic leak. During the early postoperative<br />
period (1-4 weeks), leakage from the gastrojejunal, gastroduodenal,<br />
or jejunojejunal anastomosis may develop<br />
in patients undergoing malabsorptive procedures, such as<br />
Roux-en-Y gastric bypass or biliopancreatic diversion<br />
with duodenal switch. Because it is potentially life-threat
ening, this complication has been well publicized<br />
Reported frequencies in large series (≥2,000 patients)<br />
have ranged from 3%. 10,11<br />
Anastomotic leaks most commonly occur during a<br />
surgeon’s first 75 laparoscopic bypass procedures. 12,13<br />
<strong>The</strong> leak usually manifests while the patient is hospitalized;<br />
however, signs and symptoms may not appear<br />
until 7 to 14 days after surgery. <strong>The</strong> primary care physician<br />
should, therefore, be familiar with their signs and<br />
symptoms.<br />
<strong>The</strong> most sensitive signs <strong>of</strong> anastomotic leak are sustained<br />
tachycardia <strong>of</strong> >120 bpm. 14 Additional signs and<br />
symptoms include fever, shoulder pain (usually in the<br />
left), abdominal pain, shortness <strong>of</strong> breath, and respiratory<br />
rate <strong>of</strong> >22 bpm, increased thirst, and hypotension.<br />
When an anastomotic leak is suspected, the recommended<br />
workup includes a barium swallow or CT scan<br />
with contrast, complete blood count with differential,<br />
comprehensive metabolic panel, and chest X-rays (posterior-anterior<br />
and lateral).<br />
If diagnosed early, the leak can be managed conservatively<br />
without long-term sequelae in most cases. Early<br />
management typically involves total parenteral nutrition<br />
(NPO) and antibiotic therapy. Percutaneous<br />
drainage <strong>of</strong> any collection may be warranted to prevent<br />
abscess formation. In the unstable patient, surgical reexploration<br />
with repair, drainage, and G-tube placement<br />
may be indicated.<br />
Pulmonary embolism. In contrast to the anastomotic<br />
leak, pulmonary embolism is not widely publicized<br />
as a cause <strong>of</strong> death after bariatric surgery; nevertheless,<br />
it may be the most frequent cause <strong>of</strong> operative<br />
mortality (1-30 days). All patients are at risk for deep<br />
venous thrombosis/pulmonary embolism (DVT/PE)<br />
regardless <strong>of</strong> the procedure performed. Hence, aggressive<br />
prophylaxis is warranted. 15<br />
Definitive data on the incidence <strong>of</strong> pulmonary<br />
embolism after bariatric surgery are lacking; estimates<br />
place it at 2% to 4%. In a retrospective study <strong>of</strong><br />
DVT/PE prophylaxis by Miller and Rovito, the 30-day<br />
incidence <strong>of</strong> pulmonary embolism was 1.2%. 15<br />
An effective prophylactic treatment regimen for<br />
DVT/PE consists <strong>of</strong> low-molecular-weight heparin<br />
administered intraoperatively and twice a day until discharge,<br />
lower extremity compression devices, and early<br />
ambulation. As mentioned, preoperative placement <strong>of</strong><br />
THE JOURNAL OF<br />
FAMILY<br />
PRACTICE<br />
an inferior vena cava filter is an option in high-risk<br />
patients, such as those with a history <strong>of</strong> DVT/PE, clotting<br />
disorders, or significant venous stasis. 7 As with<br />
anastomotic leak, DVT/PE can occur as late as 2 weeks<br />
after surgery, so familiarity with the signs and symptoms<br />
is important.<br />
Nausea and vomiting. Intermittent nausea and<br />
vomiting <strong>of</strong>ten occur soon after bariatric surgery. <strong>The</strong><br />
complication is by no means life-threatening but can be<br />
frustrating for the patient and primary care physician.<br />
Causes <strong>of</strong> nausea include dehydration, pain medication,<br />
administration <strong>of</strong> vitamins, pouch size, and eating too<br />
quickly, eating too much, or not chewing adequately.<br />
Patients who are unable to keep down fluids and solids<br />
for a 24-hour period should be evaluated for possible<br />
obstruction and/or dehydration.<br />
Nausea typically responds to rehydration and<br />
antiemetic medication administered orally, per rectum,<br />
or intravenously. Repeated administration <strong>of</strong> intravenous<br />
fluid may be necessary.<br />
Patients who are also vomiting need to be given<br />
thiamine/folate and a multiple vitamin in the intravenous<br />
infusion to prevent thiamine deficiency and<br />
Wernicke’s encephalopathy. <strong>The</strong> latter may occur after<br />
any gastric surgery. Often, administration <strong>of</strong> thiamine<br />
alone immediately alleviates nausea and vomiting.<br />
Repeated vomiting may cause pouch swelling and<br />
anastomotic narrowing, which, in turn, may exacerbate<br />
nausea and vomiting. In addition, pouch size and<br />
the angle <strong>of</strong> the anastomosis into the jejunum can contribute<br />
to emesis. In rare instances, total parenteral<br />
nutrition may be necessary until the patient can tolerate<br />
adequate oral feeding.<br />
Wound complications. Wound infection or cellulitis<br />
occurs in 5% to 20% <strong>of</strong> patients who undergo an<br />
open procedure. <strong>Management</strong> <strong>of</strong>ten requires no more<br />
than opening the incision and local packing. An extended<br />
course <strong>of</strong> antibiotic therapy may not be necessary.<br />
Other early complications. Diarrhea is frequent<br />
after bariatric surgery and may be caused by new onset<br />
(<strong>of</strong>ten temporary) lactose intolerance, which can be<br />
resolved with ezymatic therapy or withdrawal <strong>of</strong> dairy<br />
products. Other causes <strong>of</strong> diarrhea include occult ingestion<br />
<strong>of</strong> sugar contained in prescription and over-the-<br />
March 2005 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> 21
<strong>Management</strong> <strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>: <strong>The</strong> role <strong>of</strong> bariatric surgery<br />
TABLE 3<br />
Selected medications that should be avoided<br />
after malabsorptive procedures<br />
Nonsteroidal antiinflammatory<br />
drugs<br />
Advil (ibupr<strong>of</strong>en)<br />
Aleve (naproxen)<br />
Anaprox (naproxen)<br />
Ansaid (flurbipr<strong>of</strong>en)<br />
Azolid (phenylbutazone)<br />
Bextra (valdecoxib)<br />
Butazolidin<br />
(phenylbutazone)<br />
Celebrex (celecoxib)<br />
Clinoril (sulindac)<br />
Dolobid (diflunisal)<br />
Excedrin IB (ibupr<strong>of</strong>en)<br />
Feldene (piroxicam)<br />
Ibuprin (ibupr<strong>of</strong>en)<br />
Indocin (indomethacin)<br />
Lodine (etodolac)<br />
Meclomen<br />
(mecl<strong>of</strong>enamate)<br />
Midol IB (ibupr<strong>of</strong>en)<br />
Motrin (ibupr<strong>of</strong>en)<br />
Motrin-IB (ibupr<strong>of</strong>en)<br />
Nalfon (fenopr<strong>of</strong>en)<br />
Naprosyn (naproxen)<br />
Nuprin (ibupr<strong>of</strong>en)<br />
Orudis (ketopr<strong>of</strong>en)<br />
Oruvail (ketopr<strong>of</strong>en)<br />
Pamprin-IB (ibupr<strong>of</strong>en)<br />
Ponstel (mefenamic acid)<br />
Rexolate<br />
(sodium thiosalicylate)<br />
Tandearil<br />
(oxyphenbutazone)<br />
Tolectin (tolmetin)<br />
Voltaren (dicl<strong>of</strong>enac)<br />
Barbiturate<br />
Fiorinal (butalbital/aspirin/caffeine)<br />
Salicylates<br />
Amigesic (salsalate)<br />
Anacin (aspirin)<br />
Arthropan<br />
(choline salicylate)<br />
Ascriptin<br />
(buffered aspirin)<br />
Aspirin (aspirin)<br />
Aspirtab (aspirin)<br />
Bufferin<br />
(buffered aspirin)<br />
Disalcid (salsalate)<br />
Ecotrin (aspirin)<br />
Uracel<br />
(sodium salicylate)<br />
Analgesics<br />
Darvon (propoxyphene)<br />
Equagesic<br />
(meprobamate/aspirin)<br />
Micrainin<br />
(meprobamate/aspirin)<br />
Percodan<br />
(oxycodone/aspirin)<br />
Marcolide antibiotics<br />
Biaxin (clarithromycin)<br />
E-Mycin (erythromycin)<br />
Eryped (erythromycin)<br />
Erythrocin (erythromycin)<br />
Robimycin (erythromycin)<br />
Zithromax (azithromycin)<br />
Tetracycline antibiotics<br />
Brodspec (tetracycline)<br />
Panmycin (tetracycline)<br />
Sumycin (tetracycline)<br />
Tetracap (tetracycline)<br />
Ketolide antibiotic<br />
Ketek (telithromycin)<br />
counter drugs, malabsorption or dumping syndrome,<br />
and Clostridium difficile colitis.<br />
More common than diarrhea, however, is constipation,<br />
which results from the high protein intake,<br />
decreased fruit and vegetable intake, and administration<br />
<strong>of</strong> narcotic pain medication after surgery.<br />
Metabolic management. Aggressive metabolic and<br />
medication management is crucial in all patients during<br />
22 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> March 2005<br />
the early postoperative period. Insulin requirements fall<br />
significantly immediately after weight-loss surgery, and<br />
other medications need to be reduced in dosage or withdrawn.<br />
In patients who were receiving preoperative<br />
antidiabetic therapy, oral glycemic agents should be<br />
replaced with sliding-scale, short-acting insulin.<br />
Similarly, antihypertensive medications should be<br />
reduced in dosage or discontinued and diuretics should<br />
be withheld. Antilipid agents also should be held during<br />
the early postoperative period, given their tendency to<br />
produce nausea in some patients.<br />
Essential medications should be administered in<br />
regular-release rather than sustained-release formulations<br />
to <strong>of</strong>fset the altered gastrointestinal absorption<br />
that occurs after malabsorptive procedures.<br />
Moreover, patient tolerance <strong>of</strong> medications can be<br />
improved by crushing the tablets or giving a liquid<br />
formulation <strong>of</strong> the drug during the first 4 postoperative<br />
weeks. By the fifth week, bisecting the tablets is<br />
usually sufficient.<br />
Late postoperative period<br />
<strong>The</strong> most common late complications seen after Rouxen-Y<br />
gastric bypass are gallstones, stomal stenosis, and<br />
marginal ulcers. 16 Gallstones <strong>of</strong>ten develop after rapid<br />
weight loss, be it surgically or nonsurgically induced,<br />
For this reason, some surgeons opt for prophylactic<br />
cholecystectomy at the time <strong>of</strong> surgery. When<br />
cholelithiasis is documented on preoperative ultrasound<br />
or palpated intraoperatively, simultaneous<br />
cholecystectomy probably is warranted.<br />
Marginal ulcers and stomal stenosis occur in 10%<br />
<strong>of</strong> gastric bypass patients. Chronic use <strong>of</strong> aspirin, nonsteroidal<br />
anti-inflammatory agents, and some other<br />
medications has been associated with significantly<br />
increased risk for these complications. <strong>The</strong>refore, the<br />
agents listed in TABLE 3 should be avoided after malabsorptive<br />
procedures. Marginal ulcers respond to<br />
treatment with proton pump inhibitors and stenosis <strong>of</strong><br />
the gastrojejunostomy is readily dilated by an experienced<br />
endoscopist.<br />
Nutritional management<br />
Immediately after surgery, patients are placed on a<br />
sugar-free, clear-liquid diet, from which they progress<br />
slowly, as tolerated, to a prudent low-fat diet. Most<br />
comprehensive bariatric surgery programs have estab-
lished a series <strong>of</strong> specific diets<br />
with recommended stages <strong>of</strong><br />
progression (TABLE 4). A<br />
variety <strong>of</strong> commercial supplements<br />
designed specifically<br />
for bariatric surgery patients’<br />
postoperative needs contain<br />
the required vitamins, minerals,<br />
and protein and <strong>of</strong>fer<br />
some convenience for postoperative<br />
nutrition. <strong>The</strong>se formulations<br />
usually obviate the<br />
need for additional vitamin<br />
supplementation and its<br />
attendant risk <strong>of</strong> nausea.<br />
As mentioned, the most<br />
frequent cause <strong>of</strong> postoperative<br />
emesis is eating too quickly<br />
or too much or not chewing<br />
adequately. Patients should<br />
consume small frequent meals<br />
throughout the day and should<br />
not drink fluids for at least 1<br />
hour after eating. When fluids<br />
are permitted, carbonated beverages<br />
should be avoided.<br />
Patients with recurrent vomiting<br />
are at risk for pouch<br />
swelling and edema and<br />
should temporarily go back to<br />
clear- or full-liquid diet until<br />
symptoms abate.<br />
Dumping syndrome may<br />
occur in patients who undergo<br />
a combined restrictive/<br />
malabsorptive procedure such<br />
as the Roux-en-Y gastric<br />
bypass. Dumping is the<br />
jejunum’s response to the<br />
rapid introduction <strong>of</strong> a large<br />
amount <strong>of</strong> undigested carbohydrate.<br />
Enteroglucagon and<br />
other gastrointestinal hormones<br />
cause an influx <strong>of</strong> fluid<br />
into the lumen <strong>of</strong> the small<br />
intestine, which is usually fol-<br />
TABLE 4<br />
THE JOURNAL OF<br />
FAMILY<br />
PRACTICE<br />
Recommended dietary stages after gastric bypass surgery<br />
STAGE 1: Water and sugar-free clear liquids<br />
Begin: 1 day after surgery Duration: 1 day<br />
Diet: 3 fluid oz (90 cc) <strong>of</strong> regular bouillon or diet Jell-O ® per meal, plus 3-5 oz <strong>of</strong><br />
water or decarbonated (flat) diet ginger ale per hour between meals. Fluid intake<br />
should not exceed 8 oz/hour<br />
Fluid Goal: 32 oz/day (1 qt)<br />
STAGE 2: High-protein liquid supplements primarily<br />
Begin: 2 days after surgery or 24 hours after stage 1 was begun Duration: 4 weeks<br />
Diet: 8 oz <strong>of</strong> high-protein liquid supplement 2-3 times a day plus stage 1 beverages<br />
Fluid Goal: 48-64 oz/day Protein Goal: 60 gm/day minimum<br />
• Keep a food diary to track protein and fluid intake.<br />
STAGE 3: S<strong>of</strong>t-protein foods<br />
Begin: 4 weeks after surgery Duration: 4 weeks<br />
Diet: 3 oz <strong>of</strong> s<strong>of</strong>t foods (no fruits, vegetables, or starchy foods) 3 times a day<br />
plus stage 1 beverages<br />
Fluid Goal: 48-64 oz/day Protein Goal: 60 gm/day minimum<br />
• Eat slowly; no more than 1 oz every 10 minutes.<br />
• If you feel full, stop eating; otherwise, vomiting can occur.<br />
• Continuous overeating will stretch your new pouch.<br />
• Do not consume foods and beverages at the same time.<br />
Wait 30 minutes before eating and another 60 minutes after<br />
eating before drinking fluids.<br />
• Avoid cold or hot liquids and foods that are high in sugar or fat;<br />
they cause dumping syndrome.<br />
• Continue food diary to track protein and fluid intake.<br />
STAGE 4: Low-fat, low-sugar foods<br />
Begin: Approximately 8 weeks after surgery Duration: Lifelong<br />
Diet: Use the Food Pyramid as a guide. Every day, try to eat 6 oz <strong>of</strong> meat or<br />
high-protein foods, 2 cups <strong>of</strong> milk products, 2-3 servings <strong>of</strong> grains or starch,<br />
2 servings <strong>of</strong> vegetables, and 2-3 servings <strong>of</strong> fruit.<br />
Fluid Goal: 48-64 oz/day Protein Goal: 60 gm/day minimum<br />
• Gradually introduce new foods to your diet 1 at a time. Go slowly<br />
with fresh fruits and vegetables.<br />
• If a food is not tolerated, wait 2-4 weeks before reintroducing it.<br />
• Consume protein at each meal.<br />
• Take at least 30-60 minutes to consume a typical meal, which should<br />
fit on a dish no larger than a salad plate.<br />
• Continue to keep a food diary to ensure adequate protein and<br />
fluid intake.<br />
March 2005 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> 23
<strong>Management</strong> <strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>: <strong>The</strong> role <strong>of</strong> bariatric surgery<br />
TABLE 5<br />
Nutrient supplementation after gastric bypass surgery<br />
Recommended<br />
dosage Comments<br />
Iron 40-65 mg/day • 2 chewable multiple vitamin (with iron)<br />
tablets daily for the first month, then<br />
• 1 prenatal multiple vitamin or 2<br />
regular multiple vitamin (with iron)<br />
tablets daily<br />
Vitamin B 12 350 mcg/day • An additional 1,000 mcg IM every 1-3<br />
sublingually months, if necessary<br />
Folate 800-1,000 • Most multiple vitamin tablets contain<br />
mcg/day recommended dosage<br />
Calcium + Calcium: 1,200- • Calcium citrate preferred over calcium<br />
Vitamin D 1,500 mg/day carbonate, which is malabsorbed after<br />
Vitamin D: gastric bypass<br />
1,600 IU/day<br />
lowed by runny nose, excessive salivation, nausea,<br />
tachycardia, syncope or presyncope, vomiting, and<br />
diarrhea. 17 <strong>The</strong> small bowel gradually adapts to the<br />
anatomic changes <strong>of</strong> surgery, and dumping syndrome<br />
usually resolves in 6 to 12 months. Although uncomfortable,<br />
the syndrome provides valuable negative<br />
reinforcement for patients to avoid concentrated<br />
sweets and carbohydrates.<br />
Psychologic follow-up<br />
After surgery, patients need early and frequent contact<br />
with a psychologist or psychiatrist to address such<br />
issues as adjustment to behavioral and dietary<br />
changes, depression, marital/family discord, poor selfimage/esteem,<br />
and impaired coping mechanisms).<br />
Continued participation in support groups is beneficial<br />
and recommended. Many online support groups<br />
and chat rooms have appeared recently. Visiting such<br />
sites (eg, Association for Morbid Obesity Support at<br />
www.<strong>obesity</strong>help.com/<strong>morbid</strong> <strong>obesity</strong>/index.html)<br />
may help to reinforce goals <strong>of</strong> the bariatric program.<br />
Medical management<br />
Patients who have undergone a malabsorptive procedure<br />
require lifelong supplementation with vitamins and<br />
24 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> March 2005<br />
minerals, iron, vitamin B 12,<br />
and calcium with vitamin D<br />
(TABLE 5). 18 Gastric bypass<br />
patients should receive 40 to<br />
65 mg/day <strong>of</strong> iron, which<br />
can be obtained from most<br />
prescription prenatal vitamin<br />
supplements. Additional iron<br />
may be warranted, especially<br />
in menstruating women.<br />
Folate deficiency is rare<br />
after malabsorptive procedures.<br />
<strong>The</strong> recommended<br />
800 to 1,000 mcg/day <strong>of</strong><br />
folate is generally contained<br />
in over-the-counter multiple<br />
vitamins.<br />
Vitamin B 12 deficiency<br />
occurs in about one-third <strong>of</strong><br />
patients after malabsorptive<br />
surgery. An average dose <strong>of</strong><br />
350 mcg/day <strong>of</strong> sublingual B 12 is recommended.<br />
Intramuscular injections <strong>of</strong> 1,000 mcg <strong>of</strong> B 12 every 1<br />
to 3 months may be warranted in some patients.<br />
Calcium with vitamin D is an important supplement<br />
that is <strong>of</strong>ten overlooked in gastric bypass<br />
patients. Calcium absorption, which occurs in the<br />
duodenum, is bypassed by the procedure, placing<br />
these patients at increased risk for osteoporosis.<br />
Calcium citrate (1,200-1,500 mg/day along with<br />
1,600 IU <strong>of</strong> vitamin D) is preferred over calcium carbonate.<br />
<strong>The</strong> pouch <strong>of</strong> gastric bypass patients contains<br />
fewer than the normal number <strong>of</strong> parietal cells, resulting<br />
in decreased acid secretion and accelerated<br />
absorption <strong>of</strong> calcium carbonate.<br />
Deficiencies <strong>of</strong> these essential nutrients can cause<br />
significant neurologic and metabolic disorders; therefore,<br />
annual serologic testing and measurement <strong>of</strong><br />
bone mineral density is recommended. In patients<br />
with significant steatohepatitis or fibrosis at the time<br />
<strong>of</strong> surgery, a liver biopsy performed 12 to 24 months<br />
postoperatively will help assess progression or regression<br />
<strong>of</strong> disease. Similarly, follow-up polysomnogram<br />
should be considered to ensure resolution <strong>of</strong> obstructive<br />
sleep apnea.<br />
<strong>The</strong> ramifications <strong>of</strong> altered gut absorption for<br />
drug dosing extend well beyond the early postopera-
tive period. Adequate absorption <strong>of</strong> medication<br />
should be held in question at least until the jejunum<br />
has fully adapted surgical alterations. Measurement<br />
<strong>of</strong> blood drug levels may be necessary, particularly in<br />
patients receiving antiseizure, thyroid replacement, or<br />
antipsychotic medications, and dosages adjusted to<br />
achieve required therapeutic levels. In some cases,<br />
placement <strong>of</strong> a G-tube at the time <strong>of</strong> surgery is warranted<br />
to ensure adequate drug levels.<br />
Pregnancy should be avoided for 12 to 18 months<br />
after surgery. <strong>The</strong> altered absorption <strong>of</strong> essential nutrients<br />
and rapid weight loss confer an increased risk for<br />
neural tube defects and other perinatal complications.<br />
19,20 As with all medications, therapeutic blood levels<br />
<strong>of</strong> oral birth control pills cannot be assumed and<br />
additional birth control (eg, barrier methods, patches,<br />
or intramuscular injection) is necessary.<br />
Realistic expectations<br />
Weight loss after bariatric surgery ranges from 30% to<br />
90% <strong>of</strong> excess body-weight loss depending on the procedure<br />
performed. Even more important is amelioration<br />
<strong>of</strong> <strong>obesity</strong>-related co<strong>morbid</strong>ities. A comprehensive<br />
meta-analysis by Buchwald et al showed that HbA 1c<br />
reverted to normal in 77% <strong>of</strong> patients with preoperative<br />
diabetes, blood pressure decreased to normal in 62% <strong>of</strong><br />
patients, and obstructive sleep apnea resolved in 86%. 21<br />
A more detailed discussion <strong>of</strong> this study can be found<br />
on page 15.<br />
In a survey <strong>of</strong> 100 gastric bypass patients, some <strong>of</strong><br />
whom had been followed for 20 years, Cook and<br />
Edwards found that patients with the most successful<br />
outcomes adhered to a strict regimen. <strong>The</strong> regimen<br />
included eating 5 small meals a day to avoid hunger,<br />
avoiding fluids for the first hour after eating, a daily<br />
intake <strong>of</strong> 60 oz <strong>of</strong> noncarbonated calorie-free beverages<br />
supplemented with calcium and vitamin B 12, sleeping an<br />
average <strong>of</strong> 7 hours a night, exercising 2.5 hours a week,<br />
and weighing themselves at least once a week. 22<br />
Summary<br />
Bariatric surgery can be a major effective component <strong>of</strong><br />
comprehensive team management <strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>, pro-<br />
THE JOURNAL OF<br />
FAMILY<br />
PRACTICE<br />
vided that the family physician gives serious consideration<br />
to both the bariatric program and surgical procedure.<br />
<strong>The</strong> family physician can be an integral member <strong>of</strong><br />
the bariatric team who initiates patient selection, makes a<br />
referral to a program that includes medical, nutritional,<br />
psychologic, and surgical interventions, and participates<br />
in pre- and postoperative management. ■<br />
REFERENCES<br />
1. Steinbrook R. Surgery for severe <strong>obesity</strong>. N Engl J Med. 2004;350:1075-<br />
1079.<br />
2. NIH Consensus Development Conference Panel. Gastrointestinal surgery<br />
for severe <strong>obesity</strong>. Ann Intern Med. 1991;115:956-961.<br />
3. Mun EC, Blackburn GL, Matthews JB. Current status <strong>of</strong> medical and surgical<br />
therapy for <strong>obesity</strong>. Gastroenterology. 2001;120:669-681.<br />
4. Inge TH, Krebs NF, Garcia VF, et al. Bariatric surgery for severely overweight<br />
adolescents: concerns and recommendations. Pediatrics.<br />
2004;114:217-223.<br />
5. Kushner RF. Roadmaps for clinical practice: Case Studies in Disease<br />
Prevention and Health Promotion. Assessment and <strong>Management</strong> <strong>of</strong> Adult<br />
Obesity: A Primer for Physicians (Booklet 7: Surgical <strong>Management</strong>).<br />
Chicago, Ill: American Medical Association; 2003.<br />
6. Papaioannou A, Michaloudis D, Fraidakis O, et al. Effects <strong>of</strong> weight loss on<br />
QTc interval in <strong>morbid</strong>ly obese patients. Obes Surg. 2003;13:869-873.<br />
7. Ferrell A, Byrne T, Robison J. Placement <strong>of</strong> inferior vena cava filters in<br />
bariatric surgical patients: possible indications and technical considerations.<br />
Obes Surg. 2004;14:738-743.<br />
8. White RH, Zhou H, Kim J, Romano PS. A population-based study <strong>of</strong> the<br />
effectiveness in inferior vena cava filter use among patients with venous<br />
thromboembolism. Arch Intern Med. 2000;160:2033-2041.<br />
9. Christou N, Sampalis J, Liberman M, et al. Surgery decreases long term<br />
mortality, and health care in <strong>morbid</strong>ly obese patients. Ann Surg.<br />
2004;240:416-424.<br />
10. Torgerson JS, Sjöström L. <strong>The</strong> Swedish Obese Subjects (SOS) study—rationale<br />
and results. Int J Obes Relat Metab Disord. 2001;25(suppl 1):S2-S4.<br />
11. Fernandez AZ Jr, De Maria EJ, Tichansky DS et al. Experience with over<br />
3,000 open and laparoscopic bariatric procedures: multivariate analysis <strong>of</strong><br />
factors relalted to leak and resultant mortality. Surg Endosc. 2004;18:<br />
193-197.<br />
12. Schauer PR, Ikramuddin S, Hamad G, et al. <strong>The</strong> learning curve for laparoscopic<br />
Roux-en-Y gastric bypass in 100 cases. Surg Endosc. 2003;17:<br />
212-215.<br />
13. Nguyen N, Rivers R, Wolfe B. Factors associated with operative outcomes<br />
in laparoscopic gastric bypass. J Am Coll Surg. 2003;197:548-557.<br />
14. Hamilton EC, Sims TL, Hamilton TT, Mullican MA, Jones DB, Provost DA.<br />
Clinical predictors <strong>of</strong> leak after laparoscopic Roux-en-Y gastric bypass for<br />
<strong>morbid</strong> <strong>obesity</strong>. Surg Endosc. 2003;17:679-684.<br />
15. Miller MT, Rovito PF. An approach to venous thromboembolism prophylaxis<br />
in laparoscopic Roux-en-Y gastric bypass surgery. Obes Surg.<br />
2004;14:731-737.<br />
16. Nguyen N, Rivers R, Wolf B. Early gastrointestinal hemorrhage after<br />
laparoscopic gastric bypass surgery. Obes Surg. 2003;13:62-65.<br />
17. Kellum J, Kuemmerle J, O'Dorisio T, et al. Gastrointestinal hormone<br />
responses to meals before and after gastric bypass and vertical banded gastroplasty.<br />
Ann Surg. 1990;211:763-770.<br />
18. Elliot K. Nutritional considerations after bariatric surgery. Crit Care Nurs<br />
Q. 2003;26:133-138.<br />
19. Wittgrove A, Jester L, Wittgrove P, et al. Pregnancy following gastric bypass<br />
for <strong>morbid</strong> <strong>obesity</strong>. Obes Surg. 1998;8:461-466.<br />
20. Moore KA, Ouyang DW, Whang EE. Maternal and fetal deaths after gastric<br />
bypass surgery for <strong>obesity</strong>. N Engl J Med. 2004;351:721-722.<br />
21. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic<br />
review and meta-analysis. JAMA. 2004;292:1724-1737.<br />
22. Cook C, Edwards C. Successful habits <strong>of</strong> long-term gastric bypass patients.<br />
Obes Surg. 1999;9:80-82.<br />
23. McTigue KM, Harris R, Hemphill B, et al. Screening and interventions for<br />
<strong>obesity</strong> in adults: summary <strong>of</strong> the evidence for the U.S. Preventive Services<br />
Task Force. Ann Intern Med. 2003;139:933-949.<br />
March 2005 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> 25
<strong>Management</strong> <strong>of</strong> <strong>morbid</strong> <strong>obesity</strong>: <strong>The</strong> role <strong>of</strong> bariatric surgery<br />
CME posttest | Answer form<br />
To receive CME credit for this activity, please visit www.jfponline.com where you can take the online posttest and receive credit. If<br />
you do not have Internet access, please complete the test below by circling the correct answer to each <strong>of</strong> the questions. Send your<br />
test with the completed registration form and program evaluation (on page 27) to: Office <strong>of</strong> CME, University <strong>of</strong> Cincinnati, PO Box<br />
670567, Cincinnati, OH 45267; Fax (513) 558-1708.<br />
1. What percentage <strong>of</strong> adults in the United States<br />
are obese?<br />
a. 19%<br />
b. 31%<br />
c. 43%<br />
d. 52%<br />
2. Which <strong>of</strong> the following bariatric surgical procedures<br />
is no longer used in the United States?<br />
a. Long-limb Roux-en-Y gastric bypass<br />
b. Vertical banded gastroplasty<br />
c. Biliopancreatic diversion<br />
d. Jejunoileal bypass<br />
3. <strong>The</strong> most commonly used bariatric surgical procedure is<br />
a. Laparoscopic Roux-en-Y gastric bypass<br />
b. Open Roux-en-Y gastric bypass<br />
c. Laparoscopic gastric banding<br />
d. Open gastric banding<br />
4. Which <strong>of</strong> the following statements about nonsurgical<br />
treatments for <strong>obesity</strong> is true?<br />
a. Maximum average weight losses range<br />
from 6 to 12 kg<br />
b. Noncompliance rates are about 50%<br />
c. Relapse rates approach 75%<br />
d. All <strong>of</strong> the above<br />
5. Which <strong>of</strong> the following anti<strong>obesity</strong> agents should be<br />
administered with caution in patients with hypertension?<br />
a. Sibutramine<br />
b. Orlistat<br />
c. All <strong>of</strong> the above<br />
d. None <strong>of</strong> the above<br />
6. Which <strong>of</strong> the following is a contraindication for<br />
bariatric surgery?<br />
a. Age 68 years<br />
b. Severe hypertension<br />
c. Schizoaffective disorder<br />
d. None <strong>of</strong> the above<br />
26 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> March 2005<br />
7. Gastric banding’s beneficial effects on weight and<br />
preoperative co<strong>morbid</strong>ities have made it the best surgical<br />
solution for <strong>morbid</strong> <strong>obesity</strong>.<br />
a. True<br />
b. False<br />
8. A minimal 4-specialty team that manages bariatric<br />
surgery patients should include a<br />
a. Nutritionist<br />
b. Physical therapist<br />
c. Diabetologist<br />
d. Cardiologist<br />
9. According to the Buchwald meta-analysis, how many<br />
patients experience resolution <strong>of</strong> diabetes, hypertension,<br />
and/or hyperlipidemia after bariatric surgery?<br />
a. 50% to 60%<br />
b. 60% to 70%<br />
c. 70% to 80%<br />
d. 80% to 90%<br />
10. Nausea and vomiting after bariatric surgery may be<br />
caused by<br />
a. Dumping syndrome<br />
b. Vitamin supplements<br />
c. Inadequate mastication <strong>of</strong> food<br />
d. All <strong>of</strong> the above<br />
11. On average, how much does systolic blood pressure<br />
decrease when an obese patient loses 2 kg <strong>of</strong><br />
weight?<br />
a. 0.6 mm Hg<br />
b. 0.8 mm Hg<br />
c. 1.0 mm Hg<br />
d. 1.2 mm Hg<br />
12. Aspirin should be avoided by patients who have<br />
undergone gastric banding.<br />
a. True<br />
b. False
Registration form (please print)<br />
NAME (LAST) (FIRST)<br />
DEGREE SPECIALTY<br />
AFFILIATION<br />
STREET ADDRESS<br />
CITY STATE ZIP<br />
TELEPHONE NUMBER FAX NUMBER<br />
E-MAIL ADDRESS<br />
SIGNATURE (I CERTIFY THAT I HAVE COMPLETED THIS CME ACTIVITY AS DESIGNED)<br />
Program Evaluation<br />
Please circle the letter that best reflects your agreement with the statements below, using the following scale:<br />
a. Strongly disagree b. Disagree c. Agree d. Strongly agree e. Does not apply<br />
THE JOURNAL OF<br />
FAMILY<br />
PRACTICE<br />
1. <strong>The</strong> program objectives were fully met.<br />
2. <strong>The</strong> quality <strong>of</strong> the educational process (presentation<br />
a b c d e<br />
and information) was satisfactory and appropriate. a b c d e<br />
3. <strong>The</strong> educational activity has enhanced my pr<strong>of</strong>essional effectiveness and improved my ability to:<br />
a. Treat/manage patients a b c d e<br />
b. Communicate with patients a b c d e<br />
c. Manage my medical practice<br />
4. <strong>The</strong> information presented was without promotional or<br />
a b c d e<br />
commercial bias. a b c d e<br />
5. <strong>The</strong> program level was appropriate.<br />
6. I intend to change my clinical practice as a result <strong>of</strong><br />
a b c d e<br />
the information presented in this CME program.<br />
7. Suggestions regarding this material, or recommendations for future presentations:<br />
a b c d e<br />
For the Physician’s Recognition Award, you can claim only the time you<br />
actually spent on this educational activity. This cannot exceed the<br />
2.5 credits designated as the maximum allowable for this supplement.<br />
HOURS: MINUTES:<br />
ACTUAL TIME SPENT ON THIS ACTIVITY<br />
❚ To receive CME credit, return this page with your<br />
completed posttest (on page 26) to:<br />
Office <strong>of</strong> CME, University <strong>of</strong> Cincinnati, PO Box 670567,<br />
Cincinnati, OH 45267<br />
Fax: 513.558.1708 Tel: 513.558.7350<br />
March 2005 Supplement to <strong>The</strong> <strong>Journal</strong> <strong>of</strong> <strong>Family</strong> <strong>Practice</strong> 27
A supplement to<br />
THE JOURNAL OF<br />
FAMILY<br />
PRACTICE<br />
<strong>Management</strong><br />
<strong>of</strong> <strong>morbid</strong><br />
<strong>obesity</strong>:<br />
<strong>The</strong> role<br />
<strong>of</strong> bariatric<br />
surgery