Delayed Sudden Death in an Infant Following an Accidental Fall
Delayed Sudden Death in an Infant Following an Accidental Fall
Delayed Sudden Death in an Infant Following an Accidental Fall

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
CASE REPORT<br />
<strong>Delayed</strong> <strong>Sudden</strong> <strong>Death</strong> <strong>in</strong> <strong>an</strong> Inf<strong>an</strong>t Follow<strong>in</strong>g <strong>an</strong><br />
<strong>Accidental</strong> <strong>Fall</strong><br />
A Case Report With Review of the Literature<br />
Abstract: Several controversies exist regard<strong>in</strong>g ultimately lethal<br />
head <strong>in</strong>juries <strong>in</strong> small children. <strong>Death</strong> from short falls, tim<strong>in</strong>g of<br />
head <strong>in</strong>jury, lucid <strong>in</strong>tervals, presence of diffuse axonal <strong>in</strong>jury (DAI),<br />
<strong>an</strong>d subdural hematoma (SDH) as marker of DAI are the most recent<br />
controversial topics of debate <strong>in</strong> this evolv<strong>in</strong>g field of study. In this<br />
area of debate, we present a case of delayed death from a witnessed<br />
fall backwards off a bed <strong>in</strong> a 9-month-old black male child who<br />
struck his head on a concrete floor <strong>an</strong>d was <strong>in</strong>dependently witnessed<br />
as “healthy” postfall for 72 hours until he was discovered dead <strong>in</strong><br />
bed. Gr<strong>an</strong>dmother, babysitter, <strong>an</strong>d mother all <strong>in</strong>dependently corroborated<br />
under police <strong>in</strong>vestigation that the child “acted <strong>an</strong>d behaved<br />
normally” after the fall until death. Autopsy showed a l<strong>in</strong>ear nondisplaced<br />
parietal skull fracture, diastasis of adjacent occipital suture,<br />
subgaleal hemorrhage with evidence of ag<strong>in</strong>g, small posterior<br />
clott<strong>in</strong>g SDH, marked cerebral edema, <strong>an</strong>d a small tear of the<br />
midsuperior body of the corpus callosum consistent with focal<br />
axonal <strong>in</strong>jury (FAI). No DAI was seen, <strong>an</strong>d there were no ret<strong>in</strong>al<br />
hemorrhages. All other causes of death were excluded upon thorough<br />
police <strong>an</strong>d medical exam<strong>in</strong>er <strong>in</strong>vestigation. Although this<br />
seems to be a rare phenomenon, a delayed, seem<strong>in</strong>gly symptom-free<br />
<strong>in</strong>terval c<strong>an</strong> occur between a cl<strong>in</strong>ically apparent mild head <strong>in</strong>jury<br />
<strong>an</strong>d accidental death <strong>in</strong> a young child.<br />
(Am J Forensic Med Pathol 2003;24: 371–376)<br />
CASE REPORT<br />
A<br />
9-month-old black male child weigh<strong>in</strong>g 22 pounds (10<br />
kg) <strong>an</strong>d measur<strong>in</strong>g 28 <strong>in</strong>ches (71 cm), 80 th percentile <strong>an</strong>d<br />
50 th percentile for age, respectively, with a history of asthma<br />
M<strong>an</strong>uscript received March 19, 2003; accepted May 29, 2003.<br />
From the Cook County Office of the Medical Exam<strong>in</strong>er, <strong>an</strong>d Department of<br />
Pathology, Rush College of Medic<strong>in</strong>e, Chicago, Ill<strong>in</strong>ois (J.S.D.), <strong>an</strong>d<br />
Knox County Office of the Medical Exam<strong>in</strong>er, <strong>an</strong>d Department of<br />
Pathology, Graduate School of Medic<strong>in</strong>e, University of Tennessee,<br />
Knoxville, Tennessee (D.M.).<br />
Repr<strong>in</strong>ts: Dar<strong>in</strong>ka Mileusnic, MD, PhD, Regional Forensic Center, University<br />
of Tennessee Memorial Hospital, 1924 Alcoa Highway, Knoxville,<br />
TN 37920. E-mail: dmileusn@mc.utmck.edu<br />
Copyright © 2003 by Lipp<strong>in</strong>cott Williams & Wilk<strong>in</strong>s<br />
0195-7910/03/2404-0371<br />
DOI: 10.1097/01.paf.0000097851.18478.16<br />
Scott Denton, MD, <strong>an</strong>d Dar<strong>in</strong>ka Mileusnic, MD, PhD<br />
treated with nebulizer, was witnessed by his gr<strong>an</strong>dmother to<br />
fall backwards off the edge of a queen-sized bed, 30 <strong>in</strong>ches<br />
off the floor. The child was sitt<strong>in</strong>g on the edge of the bed as<br />
the gr<strong>an</strong>dmother dressed her 2-year-old daughter. The child<br />
fell backwards <strong>an</strong>d rotated from the sitt<strong>in</strong>g position, strik<strong>in</strong>g<br />
the midback of his head on a v<strong>in</strong>yl-covered concrete floor at<br />
8:00 AM. He immediately beg<strong>an</strong> cry<strong>in</strong>g, <strong>an</strong>d the gr<strong>an</strong>dmother<br />
placed ice on a knot on the back of his head. He stopped<br />
cry<strong>in</strong>g <strong>an</strong>d was consolable with<strong>in</strong> a few m<strong>in</strong>utes. The child<br />
was taken to the babysitter’s residence, where the babysitter<br />
was told of the fall <strong>an</strong>d to watch for <strong>an</strong>y behavioral ch<strong>an</strong>ges.<br />
The mother was at work the morn<strong>in</strong>g when the fall occurred.<br />
When the mother picked the child up at the babysitter’s <strong>in</strong> the<br />
afternoon, he appeared well. The babysitter reported no<br />
problems <strong>an</strong>d that he acted, ate, <strong>an</strong>d behaved as usual. For the<br />
next 2 days, the gr<strong>an</strong>dmother, mother, <strong>an</strong>d babysitter did not<br />
notice <strong>an</strong>y abnormalities <strong>in</strong> either behavior or appear<strong>an</strong>ce of<br />
the child.<br />
Approximately 72 hours after the fall off the bed, the<br />
child was found at the foot of the mother’s bed, where he<br />
usually slept, prone, cold, <strong>an</strong>d unresponsive. Paramedics were<br />
called, <strong>an</strong>d <strong>in</strong> spite of resuscitative efforts, he was pronounced<br />
dead upon arrival at the hospital. He was last seen<br />
alive 8 hours prior when he was fed by his mother <strong>an</strong>d given<br />
his usual albuterol breath<strong>in</strong>g treatment. No abnormalities on<br />
the child were seen <strong>in</strong> the emergency department. There was<br />
no evidence of overly<strong>in</strong>g or asphyxia.<br />
Medical <strong>an</strong>d family history revealed that the child was<br />
born full-term weigh<strong>in</strong>g 7 pounds 4 ounces. He was diagnosed<br />
with asthma after compla<strong>in</strong>ts of wheez<strong>in</strong>g episodes <strong>an</strong>d<br />
was prescribed <strong>an</strong> albuterol nebulizer twice daily. The child’s<br />
father, who does not reside <strong>in</strong> the home, has asthma. The<br />
mother <strong>an</strong>d gr<strong>an</strong>dmother reside together <strong>in</strong> a public hous<strong>in</strong>g<br />
development. Department of Child <strong>an</strong>d Family Services<br />
records revealed no prior <strong>in</strong>cidents concern<strong>in</strong>g the deceased,<br />
but the mother had 1 report of be<strong>in</strong>g a victim of prior abuse.<br />
The gr<strong>an</strong>dmother has a remote history of coca<strong>in</strong>e abuse. Her<br />
2-year-old daughter is well <strong>an</strong>d lives with her.<br />
Autopsy revealed a well-developed <strong>an</strong>d well-nourished<br />
black male child appear<strong>in</strong>g the stated age <strong>an</strong>d without exter-<br />
The Americ<strong>an</strong> Journal of Forensic Medic<strong>in</strong>e <strong>an</strong>d Pathology • Volume 24, Number 4, December 2003 371
Denton <strong>an</strong>d Mileusnic The Americ<strong>an</strong> Journal of Forensic Medic<strong>in</strong>e <strong>an</strong>d Pathology • Volume 24, Number 4, December 2003<br />
nal abnormality. There was no swell<strong>in</strong>g or contusion of the<br />
back of the head. Complete postmortem radiographs revealed<br />
a l<strong>in</strong>ear, nondisplaced, posterior right parietal skull fracture.<br />
Internal exam<strong>in</strong>ation confirmed the skull fracture, as well as<br />
a patch or right posterior subgaleal hemorrhage that was<br />
centrally red with yellow marg<strong>in</strong>s. The underly<strong>in</strong>g right<br />
posterior l<strong>in</strong>ear skull fracture was 3.0 <strong>in</strong>ches (9.0 cm) long<br />
<strong>an</strong>d extended to the right parieto-occipital suture, caus<strong>in</strong>g<br />
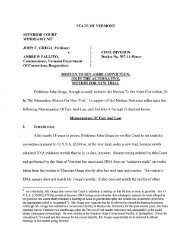
mild diastasis of the suture, 2.5 <strong>in</strong>ches (7.5 cm) long (Fig. 1).<br />
There was a th<strong>in</strong> adherent clotted SDH underly<strong>in</strong>g the fracture,<br />
2.0 2.0 0.1 cm. The bra<strong>in</strong> weighed 1035 g<br />
(expected average weight for age, 750 g) <strong>an</strong>d showed severe<br />
edema with flatten<strong>in</strong>g of the gyri, loss of sulci, <strong>an</strong>d notch<strong>in</strong>g<br />
of both unci <strong>an</strong>d cerebellar tonsils (Fig. 2). After formal<strong>in</strong><br />
fixation, serial section<strong>in</strong>g of the bra<strong>in</strong> revealed diffusely<br />
dusky white matter <strong>an</strong>d a focal tear of the midsuperior corpus<br />
FIGURE 1. View of the l<strong>in</strong>ear skull fracture <strong>in</strong>volv<strong>in</strong>g the posterior<br />
right parietal bone, after removal of the overly<strong>in</strong>g subgaleal<br />
hemorrhage.<br />
372<br />
FIGURE 2. Severely edematousbra<strong>in</strong> demonstrat<strong>in</strong>g flatten<strong>in</strong>g<br />
of the gyri <strong>an</strong>d narrow<strong>in</strong>g of the sulci.<br />
callosum, 1 mm, with surround<strong>in</strong>g hemorrhage, 2 mm. There<br />
were no other gross neuropathologic f<strong>in</strong>d<strong>in</strong>gs. The rema<strong>in</strong><strong>in</strong>g<br />
<strong>in</strong>ternal org<strong>an</strong>s were unremarkable, without other new or old<br />
fractures, petechiae, or gross asthma ch<strong>an</strong>ges. Comprehensive<br />
toxicologic screen<strong>in</strong>g us<strong>in</strong>g gas chromatography <strong>an</strong>d<br />
mass spectrometry was negative. Microscopically, the corpus<br />
callosum tear showed hemorrhage with <strong>in</strong>tact red blood cells,<br />
FAI, <strong>an</strong>d microglial activation without <strong>in</strong>flammation (Fig. 3).<br />
Extensive sections of the bra<strong>in</strong> showed only edema without<br />
evidence of DAI. Sections of the subgaleal hemorrhage<br />
showed hemorrhage of coalesc<strong>in</strong>g red blood cells with neutrophilic<br />
<strong>in</strong>flammation. Decalcified sections of the parietal<br />
fracture showed <strong>an</strong> acute fracture with early periosteal reaction<br />
at the fracture marg<strong>in</strong>. Lung sections showed mild focal<br />
peribronchial lymphocytic aggregates consistent with bronchitis<br />
without asthma ch<strong>an</strong>ges. There were neither eos<strong>in</strong>ophils<br />
nor mucus plugs. Sections of rema<strong>in</strong><strong>in</strong>g org<strong>an</strong>s were<br />
© 2003 Lipp<strong>in</strong>cott Williams & Wilk<strong>in</strong>s
The Americ<strong>an</strong> Journal of Forensic Medic<strong>in</strong>e <strong>an</strong>d Pathology • Volume 24, Number 4, December 2003 <strong>Delayed</strong> <strong>Sudden</strong> <strong>Death</strong><br />
FIGURE 3. Coronal section of the corpus callosum show<strong>in</strong>g<br />
wedge-shaped laceration (right upper corner) surrounded by a<br />
rim of hemorrhage, FAI <strong>an</strong>d activated microglia (100, hematoxyl<strong>in</strong>-eos<strong>in</strong>).<br />
without pathologic ch<strong>an</strong>ges. The eyes were exam<strong>in</strong>ed by <strong>an</strong><br />
ophthalmic pathologist consult<strong>an</strong>t <strong>an</strong>d were normal. A forensic<br />
radiologist consult<strong>an</strong>t also reviewed postmortem radiographs<br />
<strong>an</strong>d reported no additional f<strong>in</strong>d<strong>in</strong>gs.<br />
Follow-up Investigation<br />
Prior to the autopsy, Chicago police detectives were<br />
notified of the skull fracture <strong>an</strong>d attended the exam<strong>in</strong>ation.<br />
After autopsy, police rem<strong>an</strong>ded the gr<strong>an</strong>dmother <strong>an</strong>d mother<br />
to the police station, where they were <strong>in</strong>terviewed separately<br />
about the <strong>in</strong>juries. Upon extensive question<strong>in</strong>g about <strong>an</strong>y<br />
possibility of <strong>in</strong>flicted trauma <strong>an</strong>d abuse that the baby could have<br />
susta<strong>in</strong>ed, they both spont<strong>an</strong>eously gave the similar story of the<br />
fall 3 days prior. The babysitter was questioned <strong>an</strong>d confirmed<br />
the accounts <strong>an</strong>d tim<strong>in</strong>g of the reported events. Police detectives<br />
<strong>an</strong>d evidence technici<strong>an</strong>s accomp<strong>an</strong>ied the mother <strong>an</strong>d gr<strong>an</strong>dmother<br />
back to their residence <strong>an</strong>d verified the scene <strong>an</strong>d<br />
reenactment of the fall. A week later, the prosector pathologist<br />
(JSD) <strong>an</strong>d a specialist child death scene <strong>in</strong>vestigator of<br />
the Medical Exam<strong>in</strong>er’s Office went to the residence <strong>an</strong>d<br />
aga<strong>in</strong> <strong>in</strong>spected the residence, <strong>in</strong>terviewed the gr<strong>an</strong>dmother<br />
<strong>an</strong>d mother, <strong>an</strong>d reenacted the fall. As with the police detectives,<br />
all felt the gr<strong>an</strong>dmother <strong>an</strong>d mother to be truthful <strong>an</strong>d<br />
griev<strong>in</strong>g appropriately for the circumst<strong>an</strong>ces. After consideration<br />
of the autopsy, toxicologic, histologic, consultative, <strong>an</strong>d<br />
<strong>in</strong>vestigative f<strong>in</strong>d<strong>in</strong>gs, the death was certified as cr<strong>an</strong>iocerebral<br />
<strong>in</strong>juries due to a fall from the bed backwards onto a<br />
concrete floor. The m<strong>an</strong>ner was determ<strong>in</strong>ed accidental.<br />
DISCUSSION<br />
Certa<strong>in</strong> issues <strong>in</strong> pediatric head trauma, such as lethality<br />
of short falls, tim<strong>in</strong>g of head <strong>in</strong>jury, <strong>an</strong>d presence of DAI<br />
<strong>in</strong> the majority of lethal events, are still controversial. One<br />
widely held belief is that short falls are almost never fatal.<br />
Second, if a child is go<strong>in</strong>g to die follow<strong>in</strong>g head trauma,<br />
either accidental or abusive, he or she is severely impaired<br />
<strong>an</strong>d most likely immediately unconscious, without a lucid<br />
<strong>in</strong>terval. F<strong>in</strong>ally, <strong>in</strong> severe <strong>in</strong>juries where children are immediately<br />
comatose <strong>an</strong>d die shortly after the <strong>in</strong>cident from either<br />
shak<strong>in</strong>g <strong>an</strong>d/or direct impact, it is believed that DAI is the<br />
mech<strong>an</strong>ism. Certa<strong>in</strong> reviews have gone so far to identify<br />
subdural hemorrhage, frequently present <strong>in</strong> certa<strong>in</strong> forms of<br />
early childhood abusive head trauma, as a “marker” of undetectable<br />
DAI. 1 If this were true, then reports describ<strong>in</strong>g<br />
radiologically present old <strong>an</strong>d/or new subdural hemorrhages,<br />
with or without focal shear hemorrhages <strong>in</strong> the white matter,<br />
<strong>in</strong> liv<strong>in</strong>g children would be a rarity rather th<strong>an</strong> a common<br />
place. 2<br />
In this present case, we discuss the death of a 9-monthold<br />
child who died 3 days after a witnessed backward fall<br />
from a bed on a concrete floor. Ma<strong>in</strong> pathologic f<strong>in</strong>d<strong>in</strong>gs<br />
consisted of a l<strong>in</strong>ear nondisplaced skull fracture, m<strong>in</strong>imal<br />
clott<strong>in</strong>g subdural hemorrhage, severe bra<strong>in</strong> swell<strong>in</strong>g with<br />
tonsillary herniation, <strong>an</strong>d a small tear <strong>in</strong> the body of the<br />
corpus callosum, which appeared histologically as FAI. Analysis<br />
of the fall revealed a rotational component of the body<br />
<strong>an</strong>d head movement, which could account for the described<br />
<strong>in</strong>juries. The location <strong>an</strong>d appear<strong>an</strong>ce of the primary <strong>in</strong>jury<br />
was consistent with flipp<strong>in</strong>g backward <strong>an</strong>d strik<strong>in</strong>g the back<br />
of the head. There was no diffuse axonal damage or ret<strong>in</strong>al<br />
hemorrhage. Thorough workup, <strong>in</strong>clud<strong>in</strong>g scene <strong>in</strong>vestigation<br />
<strong>an</strong>d <strong>in</strong>dependent police question<strong>in</strong>g of all <strong>in</strong>dividuals <strong>in</strong>volved<br />
<strong>in</strong> the care of the <strong>in</strong>f<strong>an</strong>t, prior to, dur<strong>in</strong>g, <strong>an</strong>d after the<br />
accident, were un<strong>an</strong>imous. There were no <strong>in</strong>consistencies,<br />
<strong>an</strong>d the stories have never varied from the beg<strong>in</strong>n<strong>in</strong>g to the<br />
conclusion of the <strong>in</strong>vestigation. There were no other <strong>in</strong>st<strong>an</strong>ces<br />
of trauma to the head observed by the caretakers. Based on<br />
several <strong>in</strong>dependent accounts, the <strong>in</strong>f<strong>an</strong>t’s behavior follow<strong>in</strong>g<br />
the head trauma upto his sudden death was ord<strong>in</strong>ary <strong>an</strong>d did<br />
not require medical attention, qualify<strong>in</strong>g as a lucid or symptom-free<br />
<strong>in</strong>terval.<br />
Decid<strong>in</strong>g whether head <strong>in</strong>jury <strong>in</strong> a very young child is<br />
accidental or nonaccidental has always been problematic for<br />
cl<strong>in</strong>ici<strong>an</strong>s <strong>an</strong>d forensic pathologists alike. 3,4 We realize that a<br />
number of child abuse experts would have a problem with the<br />
accidental determ<strong>in</strong>ation of the m<strong>an</strong>ner of death <strong>in</strong> the present<br />
case. We do not argue the widely noted observation that<br />
simple falls from low heights rarely result <strong>in</strong> signific<strong>an</strong>t<br />
primary bra<strong>in</strong> <strong>in</strong>jury. 5 However, every fall is different, as well<br />
as the <strong>in</strong>dividual reaction to the primary <strong>in</strong>sult. Some experts<br />
<strong>in</strong> head trauma consider the term m<strong>in</strong>or head <strong>in</strong>jury <strong>an</strong><br />
oxymoron. 6 We believe that a series of secondary <strong>in</strong>juries,<br />
known to occur after a primary <strong>in</strong>sult, resulted <strong>in</strong> the extreme<br />
swell<strong>in</strong>g of the bra<strong>in</strong> <strong>an</strong>d death of the child. What is widely<br />
understated <strong>an</strong>d sometimes forgotten about is secondary bra<strong>in</strong><br />
© 2003 Lipp<strong>in</strong>cott Williams & Wilk<strong>in</strong>s 373
Denton <strong>an</strong>d Mileusnic The Americ<strong>an</strong> Journal of Forensic Medic<strong>in</strong>e <strong>an</strong>d Pathology • Volume 24, Number 4, December 2003<br />
<strong>in</strong>jury, which occasionally may be the pr<strong>in</strong>cipal force determ<strong>in</strong><strong>in</strong>g<br />
the outcome after a seem<strong>in</strong>gly trivial head <strong>in</strong>jury. 7–12<br />
Another frequently forgotten factor is the <strong>in</strong>fluence of age <strong>an</strong>d<br />
sex on the presentation <strong>an</strong>d the outcome of head <strong>in</strong>jury. The<br />
group<strong>in</strong>g together of different pathologies such as subdural<br />
hemorrhages, cerebral contusions, FAI, <strong>an</strong>d DAI, as well as<br />
lump<strong>in</strong>g together of <strong>in</strong>f<strong>an</strong>ts, toddlers, <strong>an</strong>d preschool children,<br />
needs to be addressed. It has been shown that <strong>in</strong>f<strong>an</strong>ts <strong>an</strong>d<br />
young toddlers lose consciousness less frequently, <strong>an</strong>d a<br />
smaller proportion of their head <strong>in</strong>juries lead to immediate<br />
coma <strong>in</strong> comparison to other children with the same grades of<br />
traumatic energy. 13 Pohl et al 9 demonstrated that evolution of<br />
posttraumatic bra<strong>in</strong> damage after head trauma <strong>in</strong> develop<strong>in</strong>g<br />
rodents is a highly dynamic process exhibit<strong>in</strong>g age-dependent<br />
excitotoxic <strong>an</strong>d dist<strong>an</strong>t apoptotic cell death.<br />
Review<strong>in</strong>g the literature on childhood head trauma, one<br />
c<strong>an</strong> clearly see that a gradual sideway drift or evolution of<br />
f<strong>in</strong>d<strong>in</strong>gs <strong>an</strong>d conclusions of the orig<strong>in</strong>al reports, research, <strong>an</strong>d<br />
data had taken place. One of them, also frequently encountered<br />
<strong>in</strong> court, is that very young children, especially <strong>in</strong>f<strong>an</strong>ts,<br />
are automatically assumed to be the victims of “shaken baby<br />
syndrome.” 14–16 However, from the literature <strong>an</strong>d from personal<br />
experience, f<strong>in</strong>d<strong>in</strong>gs of direct impact to the head prevail.<br />
The problem is not only sem<strong>an</strong>tic <strong>in</strong> nature but has major<br />
<strong>an</strong>d far-reach<strong>in</strong>g consequences s<strong>in</strong>ce the character, location,<br />
<strong>an</strong>d cl<strong>in</strong>ical presentation of the <strong>in</strong>juries are different from the<br />
rare purely shaken babies. 17,18<br />
Another encountered fallacy is that the children who<br />
die of head trauma, especially abusive head trauma, susta<strong>in</strong><br />
DAI. Go<strong>in</strong>g back to some of the orig<strong>in</strong>al research, it is clear<br />
that the authors explicitly stated that the 2 worst types of head<br />
<strong>in</strong>jury are SDH <strong>an</strong>d DAI. These 2 have different mech<strong>an</strong>isms<br />
of causation: SDH occurs much more commonly <strong>in</strong> nonvehicular<br />
<strong>in</strong>juries, such as falls <strong>an</strong>d abusive head trauma, while<br />
DAI is caused almost exclusively by vehicular mech<strong>an</strong>isms.<br />
19–22 Although both <strong>in</strong>juries frequently share a common<br />
mech<strong>an</strong>ical cause such as <strong>an</strong>gular acceleration, they<br />
differ <strong>in</strong> degree. SDH usually occurs with a rotational <strong>in</strong>jury<br />
of short duration <strong>an</strong>d a high rate of acceleration. Conversely,<br />
motor vehicle accidents tend to cause longer-duration, loweracceleration-rate<br />
<strong>in</strong>juries lead<strong>in</strong>g to DAI rather th<strong>an</strong> SDH. 8,21<br />
SDHs occur <strong>in</strong> a greater number <strong>in</strong> children with <strong>in</strong>flicted<br />
versus non<strong>in</strong>flicted traumatic bra<strong>in</strong> <strong>in</strong>jury, whereas shear<br />
<strong>in</strong>juries are commonly visualized <strong>in</strong> the non<strong>in</strong>flicted <strong>in</strong>jury<br />
group. 22 Therefore, current supposition that the presence of<br />
SDH is a marker of DAI is likely <strong>in</strong>accurate.<br />
A frequently asked question is whether delayed mental<br />
status deterioration c<strong>an</strong> occur follow<strong>in</strong>g head <strong>in</strong>jury <strong>in</strong> children.<br />
This is critically import<strong>an</strong>t <strong>in</strong> unwitnessed circumst<strong>an</strong>ces<br />
such as child abuse. A widely held dogma is that if a<br />
child becomes unresponsive while <strong>in</strong> the care of <strong>an</strong> <strong>in</strong>dividual<br />
who is report<strong>in</strong>g the onset of unconsciousness, that same<br />
<strong>in</strong>dividual must be the perpetrator. Currently, some special-<br />
374<br />
ists <strong>in</strong>volved <strong>in</strong> the care of abused children accept as true that<br />
all children who eventually die, regardless of the type of the<br />
head <strong>in</strong>jury, must be severely disabled, usually comatose<br />
from the very moment the <strong>in</strong>jury occurred. 23 From personal<br />
experience <strong>an</strong>d based on the literature review, this tenet is not<br />
necessarily true. 24,25 Although there are clearly scenarios <strong>in</strong><br />
which this pr<strong>in</strong>ciple could be applicable, there is undoubtedly<br />
a subpopulation of <strong>in</strong>f<strong>an</strong>ts <strong>an</strong>d especially toddlers with a<br />
completely different constellation of <strong>in</strong>juries <strong>an</strong>d a dissimilar<br />
presentation. Occasionally, these children have nonspecific<br />
symptoms for several hours to a day prior to the onset of<br />
either coma or seizure followed by coma. Common observations<br />
<strong>in</strong>clude reduced physical activity, lethargy, drows<strong>in</strong>ess,<br />
irritability, temperature irregularities, poor feed<strong>in</strong>g, <strong>an</strong>d gastro<strong>in</strong>test<strong>in</strong>al<br />
symptoms. 23,26,27 Careful <strong>an</strong>alysis of the history<br />
<strong>an</strong>d the events lead<strong>in</strong>g to the critical symptoms <strong>in</strong>dicate that<br />
there was a certa<strong>in</strong> progression of symptomatology.<br />
Occult <strong>in</strong>tracr<strong>an</strong>ial <strong>in</strong>jury <strong>in</strong> <strong>in</strong>f<strong>an</strong>ts younger th<strong>an</strong> 12<br />
months of age is not uncommon. 28 Cl<strong>in</strong>ical symptoms <strong>an</strong>d<br />
signs are <strong>in</strong>sensitive <strong>in</strong>dicators of <strong>in</strong>tracr<strong>an</strong>ial <strong>in</strong>jury <strong>in</strong> <strong>in</strong>f<strong>an</strong>ts.<br />
29 Radiologic observations c<strong>an</strong> sometimes be of limited<br />
value as well. 30 Also, slow deterioration follow<strong>in</strong>g mild head<br />
<strong>in</strong>juries <strong>in</strong> children have been reported. 31 Furthermore, 1 of<br />
the most frequently cited articles on restrict<strong>in</strong>g the time of<br />
<strong>in</strong>jury <strong>in</strong> fatal <strong>in</strong>flicted head <strong>in</strong>juries draws its pediatric<br />
population ma<strong>in</strong>ly from motor vehicle accidents, with the<br />
average age of the study grouppatients be<strong>in</strong>g 8.5 years, with<br />
a SD of 4.0 years. 32<br />
Although m<strong>an</strong>y studies have offered guidel<strong>in</strong>es for<br />
determ<strong>in</strong><strong>in</strong>g the age of cerebral <strong>in</strong>juries, various factors limit<br />
the reliability of these methods; for example, reduced cerebral<br />
blood flow may impede the cellular response. Not <strong>in</strong>frequently,<br />
<strong>in</strong>jured children survive <strong>in</strong> the hospital for additional<br />
2 to 3 days or even longer, sometimes undergo<strong>in</strong>g cr<strong>an</strong>iotomy,<br />
render<strong>in</strong>g tim<strong>in</strong>g of the <strong>in</strong>juries based on the autopsy<br />
f<strong>in</strong>d<strong>in</strong>gs, <strong>in</strong>clud<strong>in</strong>g histologic exam<strong>in</strong>ation of the cerebral<br />
<strong>in</strong>juries, extremely difficult. 8,23,33–35<br />
DAI is most likely a rarity <strong>in</strong> nonaccidental head<br />
trauma, <strong>an</strong>d the term is mislead<strong>in</strong>g. 17,18,36 Coma may be more<br />
of a reflection of the severity of axonal damage <strong>in</strong> particular<br />
regions of the bra<strong>in</strong>, most notably the bra<strong>in</strong>stem, rather th<strong>an</strong><br />
the total sum of axonal <strong>in</strong>jury distributed throughout the<br />
bra<strong>in</strong>. Furthermore, the pl<strong>an</strong>e of head rotational acceleration<br />
plays <strong>an</strong> import<strong>an</strong>t role <strong>in</strong> determ<strong>in</strong><strong>in</strong>g both the distribution of<br />
axonal damage <strong>an</strong>d the production of coma. 36 The localized<br />
axonal damage demonstrated <strong>in</strong> corticosp<strong>in</strong>al tracts <strong>in</strong> the<br />
lower bra<strong>in</strong>stem <strong>an</strong>d rostral cervical cord, presumably caused<br />
by stretch to the neuroaxis produced by cervical hyperextension,<br />
may be more signific<strong>an</strong>t. This f<strong>in</strong>d<strong>in</strong>g also provides <strong>an</strong><br />
expl<strong>an</strong>ation for the frequent occurrence of apnea at presentation.<br />
In m<strong>an</strong>y of the cases reported by Geddes et al, 18 the<br />
axonal damage at the cr<strong>an</strong>iocervical junction was survivable;<br />
what was life-threaten<strong>in</strong>g was the subsequent hypoxic <strong>in</strong>jury<br />
© 2003 Lipp<strong>in</strong>cott Williams & Wilk<strong>in</strong>s
The Americ<strong>an</strong> Journal of Forensic Medic<strong>in</strong>e <strong>an</strong>d Pathology • Volume 24, Number 4, December 2003 <strong>Delayed</strong> <strong>Sudden</strong> <strong>Death</strong><br />
<strong>an</strong>d bra<strong>in</strong> swell<strong>in</strong>g. In addition, true contusional tears, which<br />
are peculiar to the bra<strong>in</strong>s of young <strong>in</strong>f<strong>an</strong>ts, represent localized<br />
“shear<strong>in</strong>g” between gray <strong>an</strong>d white matter after <strong>an</strong> impact <strong>an</strong>d<br />
should not automatically imply DAI. 17<br />
Cerebral hypoperfusion, followed by hypoxia/ischemia<br />
<strong>an</strong>d diffuse bra<strong>in</strong> swell<strong>in</strong>g, characteristic <strong>in</strong> <strong>in</strong>jured children<br />
younger th<strong>an</strong> 24 months of age, are key pathophysiological<br />
f<strong>in</strong>d<strong>in</strong>gs associated with poor outcome follow<strong>in</strong>g severe traumatic<br />
bra<strong>in</strong> <strong>in</strong>jury. 8,37–39 Primary bra<strong>in</strong> damage occurs at<br />
impact <strong>an</strong>d appears immediately or shortly after <strong>in</strong>jury. Secondary<br />
bra<strong>in</strong> <strong>in</strong>jury may be more import<strong>an</strong>t, particularly <strong>in</strong><br />
delayed fatalities, <strong>an</strong>d occurs dist<strong>an</strong>t to the impact. Secondary<br />
events may not become apparent until several hours after<br />
<strong>in</strong>jury. The largest controlled neuropathological study of<br />
nonaccidental <strong>in</strong>f<strong>an</strong>t head <strong>in</strong>jury showed that axonal damage<br />
occurred <strong>in</strong> the bra<strong>in</strong> of both head-<strong>in</strong>jured subjects <strong>an</strong>d <strong>in</strong><br />
controls <strong>in</strong> the same distribution. This is not DAI but rather<br />
diffuse vascular or hypoxic-ischemic <strong>in</strong>jury due to bra<strong>in</strong><br />
swell<strong>in</strong>g <strong>an</strong>d raised <strong>in</strong>tracr<strong>an</strong>ial pressure. The study demonstrated<br />
that the diffuse bra<strong>in</strong> damage responsible for loss of<br />
consciousness is a hypoxic secondary reaction <strong>an</strong>d argues<br />
aga<strong>in</strong>st DAI. One of the ma<strong>in</strong> conclusions of the study was<br />
that focal, localized axonal <strong>in</strong>jury <strong>an</strong>d secondary vascularhypoxic<br />
ch<strong>an</strong>ges characterize the mech<strong>an</strong>ism of bra<strong>in</strong><br />
death. 18<br />
In conclusion, we present a case of a seem<strong>in</strong>gly m<strong>in</strong>or<br />
bra<strong>in</strong> <strong>in</strong>jury <strong>in</strong> <strong>an</strong> <strong>in</strong>f<strong>an</strong>t with a symptom-free <strong>in</strong>terval, which<br />
resulted <strong>in</strong> delayed, sudden death. The import<strong>an</strong>ce of the<br />
mech<strong>an</strong>ism of <strong>in</strong>jury, location of <strong>in</strong>jury, age of the child,<br />
<strong>an</strong>d secondary bra<strong>in</strong> <strong>in</strong>jury with special reference to nonaccidental<br />
head trauma of childhood, as well as need for<br />
further research, are discussed. Although this is a rare<br />
presentation of a traumatic bra<strong>in</strong> <strong>in</strong>jury, based on recent<br />
adv<strong>an</strong>ces <strong>in</strong> traumatic neuropathology, it is conceivable, as<br />
<strong>in</strong> this case, that a delayed asymptomatic deterioration to<br />
death c<strong>an</strong> occur.<br />
REFERENCES<br />
1. Case ME, Graham MA, Corey H<strong>an</strong>dy T, et al. Position paper on fatal<br />
abusive head <strong>in</strong>juries <strong>in</strong> <strong>in</strong>f<strong>an</strong>ts <strong>an</strong>d young children. Am J Forensic Med<br />
Pathol. 2001;22:112–122.<br />
2. Demaerel P, Casteels I, Wilms G. Cr<strong>an</strong>ial imag<strong>in</strong>g <strong>in</strong> child abuse. Eur<br />
Radiol. 2002;12:849–857.<br />
3. Maxe<strong>in</strong>er H. Lethal subdural bleed<strong>in</strong>gs of babies: accident or abuse?<br />
Med Law. 2001;20:463–482.<br />
4. Fung ELW, Sung RYT, Severn Nelson EA, Poon WS. Unexpla<strong>in</strong>ed<br />
subdural hematoma <strong>in</strong> young children: is it always child abuse? Pediatr<br />
Internat. 2002;44:37–42.<br />
5. Duhaime AC, Alario AJ, Lew<strong>an</strong>der WJ, et al. Head <strong>in</strong>jury <strong>in</strong> very young<br />
children: mech<strong>an</strong>isms, <strong>in</strong>jury types, <strong>an</strong>d ophthalmologic f<strong>in</strong>d<strong>in</strong>gs <strong>in</strong> 100<br />
hospitalized patients younger th<strong>an</strong> 2 years of age. Pediatrics. 1992;90:<br />
179–185.<br />
6. Schutzm<strong>an</strong> SA, Greenes DS. Pediatric m<strong>in</strong>or head trauma. Ann Emerg<br />
Med. 2001;37:65–74.<br />
7. Bruce DA. Head <strong>in</strong>juries <strong>in</strong> the pediatric population. Curr Probl Pediatr.<br />
1990;20:61–107.<br />
8. Pearl GS. Traumatic neuropathology. Cl<strong>in</strong> Lab Med. 1998;18:39–64.<br />
9. Pohl D, Bittigau P, Ishimaru MJ, et al. N-methyl-D-aspartate <strong>an</strong>tagonists<br />
<strong>an</strong>d apoptotic cell death by head trauma <strong>in</strong> develop<strong>in</strong>g rat bra<strong>in</strong>. Proc<br />
Natl Acad Sci. USA. 1999;96:2508–2513.<br />
10. Gilles EE, Nelson MD. Cerebral complications of nonaccidental head<br />
<strong>in</strong>jury <strong>in</strong> childhood. Pediatr Neurol. 1998;19:119–128.<br />
11. Bergsneider M, Hovda D, Lee SM, et al. Dissociation of cerebral<br />
glucose metabolism <strong>an</strong>d level of consciousness dur<strong>in</strong>g the period of<br />
metabolic depression follow<strong>in</strong>g hum<strong>an</strong> traumatic bra<strong>in</strong> <strong>in</strong>jury. J Neurotrauma.<br />
2000;17:389–401.<br />
12. Ruppel RA, Clark RS, Bayir H, et al. Critical mech<strong>an</strong>isms of secondary<br />
damage after <strong>in</strong>flicted head <strong>in</strong>jury <strong>in</strong> <strong>in</strong>f<strong>an</strong>ts <strong>an</strong>d children. Neurosurg<br />
Cl<strong>in</strong> North Am. 2002;13:169–182.<br />
13. Barney J, Froidevaux A-C, Favier J. Paediatric head trauma: <strong>in</strong>fluence of<br />
age <strong>an</strong>d sex, II: biomech<strong>an</strong>ical <strong>an</strong>d <strong>an</strong>atomo-cl<strong>in</strong>ical correlations. Child<br />
Nerv Syst. 1994;10:517–523.<br />
14. Caffey J. On the theory <strong>an</strong>d practice of shak<strong>in</strong>g <strong>in</strong>f<strong>an</strong>ts: its potential<br />
residual effects of perm<strong>an</strong>ent bra<strong>in</strong> damage <strong>an</strong>d mental retardation. Am J<br />
Dis Child. 1972;124:161–169.<br />
15. Caffey J. The whiplash shaken <strong>in</strong>f<strong>an</strong>t syndrome: m<strong>an</strong>ual shak<strong>in</strong>g by the<br />
extremities with whiplash-<strong>in</strong>duced <strong>in</strong>tracr<strong>an</strong>ial <strong>an</strong>d <strong>in</strong>traocular bleed<strong>in</strong>gs,<br />
l<strong>in</strong>ked with residual perm<strong>an</strong>ent bra<strong>in</strong> damage <strong>an</strong>d mental retardation.<br />
Pediatrics. 1974;54:396–403.<br />
16. Lev<strong>in</strong> AV. Ret<strong>in</strong>al haemorrhages <strong>an</strong>d child abuse. Rec Adv Paediatr.<br />
2000;18:151–219.<br />
17. Geddes JF, Hackshaw AK, Vowles GH, et al. Neuropathology of<br />
<strong>in</strong>flicted head <strong>in</strong>jury <strong>in</strong> children, I: patterns of bra<strong>in</strong> damage. Bra<strong>in</strong>.<br />
2001;124:1290–1298.<br />
18. Geddes JF, Vowles GH, Hackshaw AK, et al. Neuropathology of<br />
<strong>in</strong>flicted head <strong>in</strong>jury <strong>in</strong> children, II: microscopic bra<strong>in</strong> <strong>in</strong>jury <strong>in</strong> <strong>in</strong>f<strong>an</strong>ts.<br />
Bra<strong>in</strong>. 2001;124:1299–1306.<br />
19. Gennarelli TA, Thibault LE. Biomech<strong>an</strong>ics of acute subdural hematoma.<br />
J Trauma. 1982;22:680–686.<br />
20. Gennarelli TA, Thibault LE, Adams JH, et al. Diffuse axonal <strong>in</strong>jury <strong>an</strong>d<br />
traumatic coma <strong>in</strong> the primate. Ann Neurol. 1982;12:564–574.<br />
21. Gennarelli TA. Head <strong>in</strong>jury <strong>in</strong> m<strong>an</strong> <strong>an</strong>d experimental <strong>an</strong>imals: cl<strong>in</strong>ical<br />
aspects. Acta Neurochir. 1983;32(suppl):1–13.<br />
22. Ew<strong>in</strong>g-Cobbs L, Kramer L, Prasad M, et al. Neuroimag<strong>in</strong>g, physical,<br />
<strong>an</strong>d developmental f<strong>in</strong>d<strong>in</strong>gs after <strong>in</strong>flicted <strong>an</strong>d non<strong>in</strong>flicted traumatic<br />
bra<strong>in</strong> <strong>in</strong>jury <strong>in</strong> young children. Pediatrics. 1998;102:300–307.<br />
23. Duhaime A-C, Christi<strong>an</strong> CW, Bali<strong>an</strong> Rorke L, Zimmerm<strong>an</strong> RA.<br />
Nonaccidental head <strong>in</strong>jury <strong>in</strong> <strong>in</strong>f<strong>an</strong>ts-the “shaken-baby syndrome.”<br />
N Engl J Med. 1998;338:1822–1829.<br />
24. Nashelsky MB, Dix JD. The time <strong>in</strong>terval between lethal <strong>in</strong>f<strong>an</strong>t shak<strong>in</strong>g<br />
<strong>an</strong>d onset of symptoms: a review of the shaken baby syndrome literature.<br />
Am J Forensic Med Pathol. 1995;16:154–157.<br />
25. Hunt<strong>in</strong>gton RW III. Symptoms follow<strong>in</strong>g head <strong>in</strong>jury. Am J Forensic<br />
Med Pathol. 2002;23:105.<br />
26. Ward JD. Pediatric issues <strong>in</strong> head trauma. New Horiz. 1995;3:539–545.<br />
27. Havil<strong>an</strong>d J, Ross Russell RI. Outcome after severe non-accidental head<br />
<strong>in</strong>jury. Arch Dis Child. 1997;77:504–507.<br />
28. Greenes DS, Schutzm<strong>an</strong> SA. Occult <strong>in</strong>tracr<strong>an</strong>ial <strong>in</strong>jury <strong>in</strong> <strong>in</strong>f<strong>an</strong>ts. Ann<br />
Emerg Med. 1998;32:680–686.<br />
29. Greenes DS, Schutzm<strong>an</strong> SA. Cl<strong>in</strong>ical <strong>in</strong>dicators of <strong>in</strong>tracr<strong>an</strong>ial <strong>in</strong>jury <strong>in</strong><br />
head-<strong>in</strong>jured <strong>in</strong>f<strong>an</strong>ts. Pediatrics. 1999;104:861–867.<br />
30. Dias MS, Backstrom J, Falk M, Veetai L. Serial radiography <strong>in</strong> the<br />
<strong>in</strong>f<strong>an</strong>t shaken impact syndrome. Pediatr Neurosurg. 1998;29:77–85.<br />
31. Snoek JW, M<strong>in</strong>derhoud JM, Wilm<strong>in</strong>k JT. <strong>Delayed</strong> deterioration follow<strong>in</strong>g<br />
mild head <strong>in</strong>jury <strong>in</strong> children. Bra<strong>in</strong>. 1984;107:15–36.<br />
32. Willm<strong>an</strong> KY, B<strong>an</strong>k DE, Senac M, Chadwick DL. Restrict<strong>in</strong>g the time of<br />
<strong>in</strong>jury <strong>in</strong> fatal <strong>in</strong>flicted head <strong>in</strong>juries. Child Abuse Negl. 1997;21:929–<br />
940.<br />
33. McD. Anderson R, Opesk<strong>in</strong> K. Tim<strong>in</strong>g of early ch<strong>an</strong>ges <strong>in</strong> bra<strong>in</strong> trauma.<br />
Am J Forensic Med Pathol. 1998;19:1–9.<br />
34. Wilk<strong>in</strong>son AE, Bridges LR, Sivalog<strong>an</strong>ath<strong>an</strong> S. Correlation of survival<br />
time with size of axonal swell<strong>in</strong>gs <strong>in</strong> diffuse axonal <strong>in</strong>jury. Acta<br />
Neuropathol. 1999;98:197–202.<br />
35. Oehmichen M, Theuerkauf I, Meissner C. Is traumatic axonal <strong>in</strong>jury (AI)<br />
associated with <strong>an</strong> early microglial activation? Application of a doublelabel<strong>in</strong>g<br />
technique for simult<strong>an</strong>eous detection of microglial <strong>an</strong>d AI. Acta<br />
Neuropathol. 1999;97:491–494.<br />
© 2003 Lipp<strong>in</strong>cott Williams & Wilk<strong>in</strong>s 375
Denton <strong>an</strong>d Mileusnic The Americ<strong>an</strong> Journal of Forensic Medic<strong>in</strong>e <strong>an</strong>d Pathology • Volume 24, Number 4, December 2003<br />
36. Smith DH, Nonaka M, Miller R, et al. Immediate coma follow<strong>in</strong>g<br />
<strong>in</strong>ertial bra<strong>in</strong> <strong>in</strong>jury dependent on axonal damage <strong>in</strong> the bra<strong>in</strong>stem.<br />
J Neurosurg. 2000;93:315–322.<br />
37. Adelson PD, Clyde B, Koch<strong>an</strong>ek PM, et al. Cerebrovascular response <strong>in</strong><br />
<strong>in</strong>f<strong>an</strong>ts <strong>an</strong>d young children follow<strong>in</strong>g severe traumatic bra<strong>in</strong> <strong>in</strong>jury: a<br />
prelim<strong>in</strong>ary report. Pediatr Neurosurg. 1997;26:200–207.<br />
376<br />
38. Ew<strong>in</strong>g-Cobbs L, Prasad M, Kramer L, L<strong>an</strong>dry S. Inflicted traumatic<br />
bra<strong>in</strong> <strong>in</strong>jury: relationshipof developmental outcome to severity of <strong>in</strong>jury.<br />
Pediatr Neurosurg. 1999;31:251–258.<br />
39. Tabori U, Kornecki A, Sofer S, et al. Repeat computed tomographic sc<strong>an</strong><br />
with<strong>in</strong> 24–48 hours of admission <strong>in</strong> children with moderate <strong>an</strong>d severe<br />
head trauma. Crit Care Med. 2000;28:840–844.<br />
© 2003 Lipp<strong>in</strong>cott Williams & Wilk<strong>in</strong>s
Diagnosis of Traumatic<br />
Diffuse Axonal Injury<br />
To the Editor:<br />
In the December 2003 issue of the<br />
Americ<strong>an</strong> Journal of Forensic Medic<strong>in</strong>e<br />
<strong>an</strong>d Pathology, there was a case report<br />
written by Drs. Scott Denton <strong>an</strong>d<br />
Dar<strong>in</strong>ka Mileusnic titled “<strong>Delayed</strong> <strong>Sudden</strong><br />
<strong>Death</strong> <strong>in</strong> <strong>an</strong> Inf<strong>an</strong>t Follow<strong>in</strong>g <strong>an</strong><br />
<strong>Accidental</strong> <strong>Fall</strong>: A Case Report With<br />
Review of the Literature.” This article<br />
presented a case of delayed death <strong>in</strong> a<br />
9-month-old <strong>in</strong>f<strong>an</strong>t as a result of severe<br />
cr<strong>an</strong>iocerebral <strong>in</strong>juries, which were susta<strong>in</strong>ed<br />
from <strong>an</strong> accidental fall <strong>in</strong> the<br />
domestic environment. The authors had<br />
affirmed that there was no evidentiary<br />
f<strong>in</strong>d<strong>in</strong>g of diffuse axonal <strong>in</strong>jury (DAI).<br />
The scientific validity of this assertion<br />
rema<strong>in</strong>s <strong>in</strong> doubt s<strong>in</strong>ce the authors neither<br />
mentioned nor performed <strong>an</strong>y tissue<br />
-amyloid precursor prote<strong>in</strong> (-APP)<br />
immunohistochemical <strong>an</strong>alyses, given<br />
our current level of knowledge <strong>in</strong> the<br />
diagnosis of severe traumatic bra<strong>in</strong> <strong>in</strong>jury,<br />
<strong>in</strong>clud<strong>in</strong>g DAI. 1–6 S<strong>in</strong>ce the 1980s,<br />
tissue immunohistochemistry for -APP<br />
has emerged as the most sensitive methodology<br />
<strong>an</strong>d gold st<strong>an</strong>dard for the detection,<br />
confirmation, <strong>an</strong>d diagnosis of diffuse<br />
<strong>an</strong>d focal axonal <strong>in</strong>jury. With the<br />
absence of <strong>an</strong>y -APP immunohistochemical<br />
confirmation of DAI, what the<br />
authors had referred to as a “laceration”<br />
of the splenium of the corpus callosum<br />
may actually represent Adam’s grade II<br />
DAI 7,8 s<strong>in</strong>ce DAI is accentuated <strong>in</strong> the<br />
splenium of the corpus callosum. 9 In<br />
Adam’s grade I DAI, there is no gross<br />
evidence of axonal <strong>in</strong>jury; however,<br />
there is diffuse -APP immunopositivity<br />
for axonal <strong>in</strong>jury. In Adam’s grade II<br />
DAI, there are gross lesions (parenchymal<br />
hemorrhages) of the corpus callosum,<br />
<strong>in</strong> addition to -APP tissue immunopositivity.<br />
In Adam’s grade III DAI,<br />
there are gross lesions (parenchymal<br />
hemorrhages) of the corpus callosum<br />
<strong>an</strong>d dorsolateral midbra<strong>in</strong>/pons, <strong>in</strong> addition<br />
to diffuse -APP tissue immunopositivity.<br />
7,8<br />
270<br />
LETTERS TO THE EDITOR<br />
-APP is a s<strong>in</strong>gle membr<strong>an</strong>e–<br />
sp<strong>an</strong>n<strong>in</strong>g prote<strong>in</strong>, which is present <strong>in</strong><br />
membr<strong>an</strong>ous structures of the cell such<br />
as the endoplasmic reticulum, Golgi<br />
compartment, <strong>an</strong>d the cell membr<strong>an</strong>e,<br />
encoded by the APP gene localized to<br />
chromosome 21, <strong>an</strong>d is ubiquitously expressed<br />
<strong>in</strong> m<strong>an</strong>y cell <strong>an</strong>d tissue types,<br />
<strong>in</strong>clud<strong>in</strong>g endothelia, glia, <strong>an</strong>d neurons<br />
of the bra<strong>in</strong>. -APP is a resource-rich<br />
molecule that is <strong>in</strong>volved <strong>in</strong> diverse normal<br />
cell functions, be<strong>in</strong>g the center of<br />
m<strong>an</strong>y converg<strong>in</strong>g metabolic <strong>an</strong>d regulatory<br />
pathways, <strong>in</strong>clud<strong>in</strong>g cell adhesion,<br />
<strong>in</strong>tercellular signal<strong>in</strong>g, membr<strong>an</strong>e-to-nucleus<br />
signal<strong>in</strong>g, cholesterol metabolism,<br />
gene tr<strong>an</strong>scription, axonal tr<strong>an</strong>sport, <strong>an</strong>d<br />
neurotrophic <strong>an</strong>d neuroproliferative activity.<br />
1<br />
In the neuron, -APP is synthesized<br />
<strong>in</strong> the perikaryon <strong>an</strong>d tr<strong>an</strong>sported<br />
<strong>an</strong>terogradely <strong>an</strong>d retrogradely <strong>in</strong> the<br />
axon by fast/rapid axonal tr<strong>an</strong>sport (100<br />
to 400 mm/day). In normal, structurally<br />
<strong>in</strong>tact axons, -APP does not accumulate<br />
to a level that allows its detection <strong>in</strong><br />
tissue sections. However, once structural<br />
axonal <strong>in</strong>jury <strong>an</strong>d damage occur<br />
<strong>an</strong>d the fast axonal tr<strong>an</strong>sport is impaired,<br />
-APP accumulates <strong>in</strong> the proximal <strong>an</strong>d<br />
distal axonal segment to a level that<br />
allows its detection by tissue immunohistochemistry<br />
with<strong>in</strong> 1.75 to 3 hours<br />
follow<strong>in</strong>g <strong>in</strong>jury. -APP has been reported<br />
to rema<strong>in</strong> detectable by tissue<br />
immunohistochemistry for up to 99 days<br />
follow<strong>in</strong>g axonal <strong>in</strong>jury. 1,6<br />
For this specified case report by<br />
Scott Denton <strong>an</strong>d Dar<strong>in</strong>ka Mileusnic,<br />
-APP tissue immunohistochemistry<br />
that is performed accord<strong>in</strong>g to the recommended<br />
medicolegal protocol 10 may<br />
reveal grades I or II DAI. This f<strong>in</strong>d<strong>in</strong>g<br />
may additionally <strong>an</strong>d more <strong>in</strong>terest<strong>in</strong>gly<br />
reaffirm that children who susta<strong>in</strong> low<br />
grades of DAI may m<strong>an</strong>ifest a delayed,<br />
symptomatic, or fatal presentation.<br />
Bennet I. Omalu, MD<br />
Division of Forensic Neuropathology<br />
Allegheny County Coroner’s Office<br />
Pittsburgh, Pennsylv<strong>an</strong>ia<br />
REFERENCES<br />
1. Turner PR, O’Connor K, Tate WP, et al. Roles<br />
of amyloid precursor prote<strong>in</strong> <strong>an</strong>d its fragments<br />
<strong>in</strong> regulat<strong>in</strong>g neural activity, plasticity <strong>an</strong>d<br />
memory. Prog Neurobiol. 2003;10:1–32.<br />
2. Smith C, Graham DI, Geddes JF, et al. The<br />
<strong>in</strong>terpretation of Beta-APP immunoreactivity:<br />
a response to C. Neiss et al., Acta Neuropathol<br />
(2002) 104:79. Acta Neuropathol. 2003;106:<br />
97–98.<br />
3. Smith DH, Me<strong>an</strong>ey DF, Shull WH. Diffuse<br />
axonal <strong>in</strong>jury <strong>in</strong> head trauma. J Head Trauma<br />
Rehabil. 2003;18:307–316.<br />
4. Med<strong>an</strong>a IM, Esiri MM. Axonal damage: a key<br />
predictor of outcome <strong>in</strong> hum<strong>an</strong> CNS diseases.<br />
Bra<strong>in</strong>. 2003;126:515–530.<br />
5. Blumbergs PC, Scott G, M<strong>an</strong>avis J, et al.<br />
Topography of axonal <strong>in</strong>jury as def<strong>in</strong>ed by<br />
amyloid precursor prote<strong>in</strong> <strong>an</strong>d the sector scor<strong>in</strong>g<br />
method <strong>in</strong> mild <strong>an</strong>d severe closed head<br />
<strong>in</strong>jury. J Neurotrauma. 1995;12:565–572.<br />
6. McKenzie KJ, McLell<strong>an</strong> DR, Gentlem<strong>an</strong> SM,<br />
et al. Is -APP a marker of axonal damage <strong>in</strong><br />
short-surviv<strong>in</strong>g head <strong>in</strong>jury? Acta Neuropathol.<br />
1996;92:608–613.<br />
7. Adams JH, Doyle D, Ford I, et al. Diffuse<br />
axonal <strong>in</strong>jury <strong>in</strong> head <strong>in</strong>jury: def<strong>in</strong>ition, diagnosis<br />
<strong>an</strong>d grad<strong>in</strong>g. Histopathology. 1989;15:<br />
49–59.<br />
8. Ellison D, Love S, Chimelli L, et al.<br />
Neuropathology: A Reference Text of CNS<br />
Pathology. Philadelphia, PA: Harcourt Publishers<br />
Limited; 2000.<br />
9. Leclercq PD, McKenzie JE, Graham DI, et al.<br />
Axonal <strong>in</strong>jury is accentuated <strong>in</strong> the caudal<br />
corpus callosum of head-<strong>in</strong>jured patients.<br />
J Neurotrauma. 2001;18:1–9.<br />
10. Geddes JF, Whitwell HL, Graham DI.<br />
Traumatic axonal <strong>in</strong>jury: practical issues for<br />
diagnosis <strong>in</strong> medicolegal cases. Neuropathol<br />
Appl Neurobiol. 2000;26:105–116.<br />
Response to Letter<br />
From Dr. Omalu<br />
We th<strong>an</strong>k Dr. Omalu for his comments<br />
regard<strong>in</strong>g our recent case report. 1<br />
Dr. Omalu certa<strong>in</strong>ly seems knowledgeable<br />
<strong>in</strong> his review of amyloid precursor<br />
prote<strong>in</strong> (-APP) <strong>an</strong>d is apparently a<br />
strong advocate for -APP immunohistochemistry<br />
<strong>in</strong> cases of head <strong>in</strong>jury. Dr.<br />
Omalu stated that there was no scientific<br />
validity that diffuse axonal <strong>in</strong>jury (DAI)<br />
was not there <strong>in</strong> our case. Dr. Omalu<br />
also asserted that the tear <strong>in</strong> the corpus<br />
callosum was <strong>an</strong> adv<strong>an</strong>ced stage of DAI.<br />
We would have expected to see microscopic<br />
evidence of DAI on the numer-<br />
The Americ<strong>an</strong> Journal of Forensic Medic<strong>in</strong>e <strong>an</strong>d Pathology Volume 25, Number 3, September 2004
ous hematoxyl<strong>in</strong> <strong>an</strong>d eos<strong>in</strong> sections,<br />
given the time <strong>in</strong>terval from the witnessed<br />
fall to the child’s death. The tear<br />
of the corpus callosum was from the<br />
impact from the fall as the corpus callosum<br />
struck the falx cerebri. We would<br />
argue the assertion that -APP is accepted<br />
as the most sensitive methodology<br />
<strong>an</strong>d gold st<strong>an</strong>dard for detection of<br />
DAI <strong>an</strong>d the medicolegal protocol referenced<br />
<strong>in</strong> Dr. Omalu’s letter above is not<br />
accepted as such <strong>in</strong> our practices. We do<br />
not perform rout<strong>in</strong>e -APP test<strong>in</strong>g <strong>in</strong><br />
our offices.<br />
We respect Dr. Omalu’s advocacy<br />
for -APP test<strong>in</strong>g, although we do not<br />
feel -APP would have ch<strong>an</strong>ged our<br />
conclusions or shown hidden DAI. We<br />
do note that we have received advertisements<br />
from Dr. Omalu <strong>an</strong>d his Forensic<br />
Neuropathology Consultation Service<br />
for perform<strong>in</strong>g -APP test<strong>in</strong>g. As of<br />
note, <strong>in</strong> his advertisement Dr. Omalu<br />
states that <strong>in</strong> head <strong>in</strong>jury deaths it “has<br />
been established <strong>an</strong>d highly recommended<br />
that -APP immunosta<strong>in</strong><strong>in</strong>g be<br />
performed <strong>in</strong> multiple topographically<br />
targeted regions of the bra<strong>in</strong>” <strong>an</strong>d that<br />
applications <strong>in</strong>clude “tim<strong>in</strong>g of <strong>in</strong>jury<br />
susten<strong>an</strong>ce <strong>an</strong>d determ<strong>in</strong>ation of time of<br />
death.” We are unaware of this tim<strong>in</strong>g of<br />
<strong>in</strong>jury <strong>an</strong>d death data that would surely<br />
solve the major critical problems <strong>in</strong> pediatric<br />
head <strong>in</strong>jury deaths. We s<strong>in</strong>cerely<br />
wish Dr. Omalu well <strong>in</strong> adv<strong>an</strong>c<strong>in</strong>g his<br />
-APP research <strong>an</strong>d enterprise.<br />
S<strong>in</strong>cerely,<br />
Scott Denton, MD<br />
Deputy Medical Exam<strong>in</strong>er<br />
Cook County Medical Exam<strong>in</strong>ers Office<br />
Assist<strong>an</strong>t Professor of Pathology<br />
Rush University Medical Center<br />
Chicago, IL<br />
Dar<strong>in</strong>ka Miluesnic, MD, PhD<br />
Assist<strong>an</strong>t Chief Medical Exam<strong>in</strong>er<br />
Knox County Medical Exam<strong>in</strong>ers Office<br />
University of Tennessee Medical Center<br />
Knoxville, Tennessee<br />
REFERENCES<br />
1. Denton S, Mileusnic D. <strong>Delayed</strong> sudden death<br />
<strong>in</strong> <strong>an</strong> <strong>in</strong>f<strong>an</strong>t follow<strong>in</strong>g <strong>an</strong> accidental fall: a case<br />
report with review of the literature. Am J Forensic<br />
Med Pathol. 2003;24:371–376.<br />
The Americ<strong>an</strong> Journal of Forensic Medic<strong>in</strong>e <strong>an</strong>d Pathology Volume 25, Number 3, September 2004 271