

Nontuberculous Mycobacterial Meningitis - Clinical Infectious ...
Nontuberculous Mycobacterial Meningitis - Clinical Infectious ...
Nontuberculous Mycobacterial Meningitis - Clinical Infectious ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
cm 1996;23 (December) <strong>Nontuberculous</strong> <strong>Mycobacterial</strong> <strong>Meningitis</strong> 1271<br />
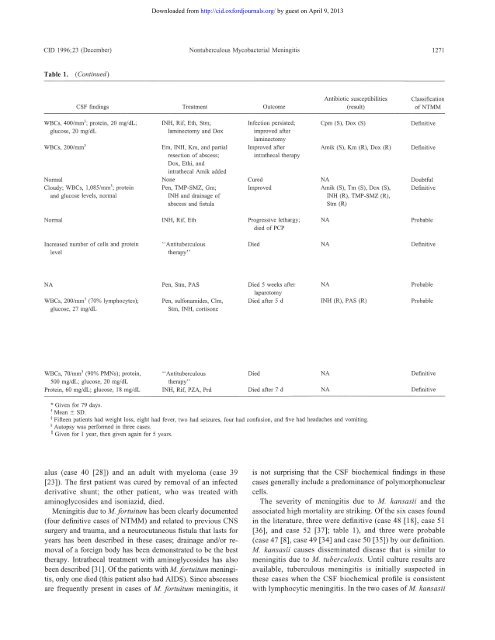
Table 1. (Continued)<br />
CSF findings<br />
WBCs, 400/mm'; protein, 20 mg/dL;<br />
glucose, 20 mg/dL<br />
WBCs, 200/mm'<br />
Normal<br />
Cloudy; WBCs, 1,085/mm'; protein<br />
and glucose levels, normal<br />
Normal<br />
Increased number of cells and protein<br />
level<br />
NA<br />
WBCs, 200/mm' (70% lymphocytes);<br />
glucose, 27 mg/dL<br />
WBCs, 70/mm' (90% PMNs); protein,<br />
500 mg/dL; glucose, 20 mg/dL<br />
Protein, 60 mg/dL; glucose, 18 mg/dL<br />
Treatment<br />
INH, Rif, Eth, Stm;<br />
laminectomy and Dox<br />
Em, INH, Km, and partial<br />
resection of abscess;<br />
Dox, Ethi, and<br />
intrathecal Amik added<br />
None<br />
Pen, TMP-SMZ, Gm;<br />
INH and drainage of<br />
abscess and fistula<br />
INH, Rif, Eth<br />
" Antituberculous<br />
therapy"<br />
Pen, Strn, PAS<br />
Pen, sulfonamides, Clm,<br />
Strn, INH, cortisone<br />
"Antituberculous<br />
therapy"<br />
INH, Rif, PZA, Prd<br />
Outcome<br />
Infection persisted;<br />
improved after<br />
laminectomy<br />
Improved after<br />
intrathecal therapy<br />
Cured<br />
Improved<br />
Progressive lethargy;<br />
died of PCP<br />
* Given for 79 days.<br />
tMean ± SD.<br />
I Fifteen patients had weight loss, eight had fever, two had seizures, four had confusion, and five had headaches and vomiting.<br />
§ Autopsy was performed in three cases.<br />
II Given for 1 year, then given again for 5 years.<br />
alus (case 40 [28]) and an adult with myeloma (case 39<br />
[23]). The first patient was cured by removal of an infected<br />
derivative shunt; the other patient, who was treated with<br />
aminoglycosides and isoniazid, died.<br />
<strong>Meningitis</strong> due to M. fortuitum has been clearly documented<br />
(four definitive cases ofNTMM) and related to previous CNS<br />
surgery and trauma, and a neurocutaneous fistula that lasts for<br />
years has been described in these cases; drainage and/or removal<br />
of a foreign body has been demonstrated to be the best<br />
therapy. Intrathecal treatment with aminoglycosides has also<br />
been described [31]. Of the patients with M. fortuitum meningitis,<br />
only one died (this patient also had AIDS). Since abscesses<br />
are frequently present in cases of M. fortuitum meningitis, it<br />
Downloaded from<br />
http://cid.oxfordjournals.org/ by guest on April 9, 2013<br />
Died<br />
Died 5 weeks after<br />
laparotomy<br />
Died after 5 d<br />
Died<br />
Died after 7 d<br />
Antibiotic susceptibilities<br />
(result)<br />
Cpm (S), Dox (S)<br />
Amik (S), Km (R), Dox (R)<br />
NA<br />
Amik (S), Tm (S), Dox (S),<br />
INH (R), TMP-SMZ (R),<br />
Strn (R)<br />
NA<br />
NA<br />
NA<br />
INH (R), PAS (R)<br />
NA<br />
NA<br />
Classification<br />
ofNTMM<br />
Definitive<br />
Definitive<br />
Doubtful<br />
Definitive<br />
Probable<br />
Definitive<br />
Probable<br />
Probable<br />
Definitive<br />
Definitive<br />
is not surprising that the CSF biochemical findings in these<br />
cases generally include a predominance of polymorphonuclear<br />
cells.<br />
The severity of meningitis due to M. kansasii and the<br />
associated high mortality are striking. Of the six cases found<br />
in the literature, three were definitive (case 48 [18], case 51<br />
[36], and case 52 [37]; table 1), and three were probable<br />
(case 47 [8], case 49 [34] and case 50 [35]) by our definition.<br />
M. kansasii causes disseminated disease that is similar to<br />
meningitis due to M. tuberculosis. Until culture results are<br />
available, tuberculous meningitis is initially suspected in<br />
these cases when the CSF biochemical profile is consistent<br />
with lymphocytic meningitis. In the two cases of M. kansasii













