AHF-fixing-labor-market-leakages-getting-more-bang-for-your-buck-on-human-resources-for-health
AHF-fixing-labor-market-leakages-getting-more-bang-for-your-buck-on-human-resources-for-health
AHF-fixing-labor-market-leakages-getting-more-bang-for-your-buck-on-human-resources-for-health

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Fixing Labor Market Leakages: Getting More Bang<br />
<str<strong>on</strong>g>for</str<strong>on</strong>g> Your Buck <strong>on</strong> Human Resources <str<strong>on</strong>g>for</str<strong>on</strong>g> Health<br />
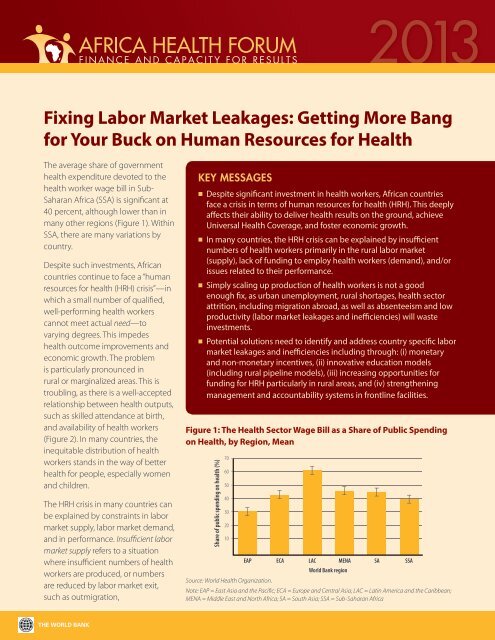
The average share of government<br />
<strong>health</strong> expenditure devoted to the<br />
<strong>health</strong> worker wage bill in Sub-<br />
Saharan Africa (SSA) is significant at<br />
40 percent, although lower than in<br />
many other regi<strong>on</strong>s (Figure 1). Within<br />
SSA, there are many variati<strong>on</strong>s by<br />
country.<br />
Despite such investments, African<br />
countries c<strong>on</strong>tinue to face a “<strong>human</strong><br />
<strong>resources</strong> <str<strong>on</strong>g>for</str<strong>on</strong>g> <strong>health</strong> (HRH) crisis”—in<br />
which a small number of qualified,<br />
well-per<str<strong>on</strong>g>for</str<strong>on</strong>g>ming <strong>health</strong> workers<br />
cannot meet actual need—to<br />
varying degrees. This impedes<br />
<strong>health</strong> outcome improvements and<br />
ec<strong>on</strong>omic growth. The problem<br />
is particularly pr<strong>on</strong>ounced in<br />
rural or marginalized areas. This is<br />
troubling, as there is a well-accepted<br />
relati<strong>on</strong>ship between <strong>health</strong> outputs,<br />
such as skilled attendance at birth,<br />
and availability of <strong>health</strong> workers<br />
(Figure 2). In many countries, the<br />
inequitable distributi<strong>on</strong> of <strong>health</strong><br />
workers stands in the way of better<br />
<strong>health</strong> <str<strong>on</strong>g>for</str<strong>on</strong>g> people, especially women<br />
and children.<br />
The HRH crisis in many countries can<br />
be explained by c<strong>on</strong>straints in <str<strong>on</strong>g>labor</str<strong>on</strong>g><br />
<str<strong>on</strong>g>market</str<strong>on</strong>g> supply, <str<strong>on</strong>g>labor</str<strong>on</strong>g> <str<strong>on</strong>g>market</str<strong>on</strong>g> demand,<br />
and in per<str<strong>on</strong>g>for</str<strong>on</strong>g>mance. Insufficient <str<strong>on</strong>g>labor</str<strong>on</strong>g><br />
<str<strong>on</strong>g>market</str<strong>on</strong>g> supply refers to a situati<strong>on</strong><br />
where insufficient numbers of <strong>health</strong><br />
workers are produced, or numbers<br />
are reduced by <str<strong>on</strong>g>labor</str<strong>on</strong>g> <str<strong>on</strong>g>market</str<strong>on</strong>g> exit,<br />
such as outmigrati<strong>on</strong>,<br />
KEY MESSAGES<br />
n Despite significant investment in <strong>health</strong> workers, African countries<br />
face a crisis in terms of <strong>human</strong> <strong>resources</strong> <str<strong>on</strong>g>for</str<strong>on</strong>g> <strong>health</strong> (HRH). This deeply<br />
affects their ability to deliver <strong>health</strong> results <strong>on</strong> the ground, achieve<br />
Universal Health Coverage, and foster ec<strong>on</strong>omic growth.<br />
n In many countries, the HRH crisis can be explained by insufficient<br />
numbers of <strong>health</strong> workers primarily in the rural <str<strong>on</strong>g>labor</str<strong>on</strong>g> <str<strong>on</strong>g>market</str<strong>on</strong>g><br />
(supply), lack of funding to employ <strong>health</strong> workers (demand), and/or<br />
issues related to their per<str<strong>on</strong>g>for</str<strong>on</strong>g>mance.<br />
n Simply scaling up producti<strong>on</strong> of <strong>health</strong> workers is not a good<br />
enough fix, as urban unemployment, rural shortages, <strong>health</strong> sector<br />
attriti<strong>on</strong>, including migrati<strong>on</strong> abroad, as well as absenteeism and low<br />
productivity (<str<strong>on</strong>g>labor</str<strong>on</strong>g> <str<strong>on</strong>g>market</str<strong>on</strong>g> <str<strong>on</strong>g>leakages</str<strong>on</strong>g> and inefficiencies) will waste<br />
investments.<br />
n Potential soluti<strong>on</strong>s need to identify and address country specific <str<strong>on</strong>g>labor</str<strong>on</strong>g><br />
<str<strong>on</strong>g>market</str<strong>on</strong>g> <str<strong>on</strong>g>leakages</str<strong>on</strong>g> and inefficiencies including through: (i) m<strong>on</strong>etary<br />
and n<strong>on</strong>-m<strong>on</strong>etary incentives, (ii) innovative educati<strong>on</strong> models<br />
(including rural pipeline models), (iii) increasing opportunities <str<strong>on</strong>g>for</str<strong>on</strong>g><br />
funding <str<strong>on</strong>g>for</str<strong>on</strong>g> HRH particularly in rural areas, and (iv) strengthening<br />
management and accountability systems in fr<strong>on</strong>tline facilities.<br />
Figure 1: The Health Sector Wage Bill as a Share of Public Spending<br />
<strong>on</strong> Health, by Regi<strong>on</strong>, Mean<br />
Share of public spending <strong>on</strong> <strong>health</strong> (%)<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
Source: World Health Organizati<strong>on</strong>.<br />
a. By regi<strong>on</strong><br />
EAP ECA LAC MENA SA SSA<br />
World Bank regi<strong>on</strong><br />
2013<br />
Note: EAP = East Asia and the Pacific; ECA = Europe and Central Asia; LAC = Latin America and the Caribbean;<br />
MENA = Middle East and North Africa; SA = South Asia; SSA = Sub-Saharan Africa
2<br />
or disproporti<strong>on</strong>ate job uptake in<br />
urban over rural areas. Insufficient<br />
<str<strong>on</strong>g>labor</str<strong>on</strong>g> <str<strong>on</strong>g>market</str<strong>on</strong>g> demand refers to a<br />
situati<strong>on</strong> where there are insufficient<br />
<strong>resources</strong> (public or private)<br />
available to hire <strong>health</strong> workers.<br />
AFRICA HEALTH FORUM 2013<br />
Finally, problems with <strong>health</strong> worker<br />
per<str<strong>on</strong>g>for</str<strong>on</strong>g>mance include insufficient<br />
skills to carry out services, lack of<br />
equipment and supplies to apply<br />
skills, or low attendance, motivati<strong>on</strong>,<br />
and productivity.<br />
Figure 2: Health worker density is correlated with skilled attendance<br />
at birth, Africa, 2005–09<br />
Skilled attendance at birth (%)<br />
100<br />
90<br />
80<br />
70<br />
DRC<br />
Benin<br />
Health worker density (per 1,000 populati<strong>on</strong>)<br />
Source: WHO/Global Atlas (2005–2009) and UNICEF (latest year available).<br />
Figure 3: Findings from a Discrete Choice Experiment: Share of<br />
nurses in Ethiopia willing to accept a rural job, as a functi<strong>on</strong> of<br />
the rural wage b<strong>on</strong>us (horiz<strong>on</strong>tal axis), with alternative in-kind<br />
attribute incentives<br />
Source: Jack and others in Berhanu Feysia and others, 2012<br />
Botswana<br />
Namibia<br />
Mauritius<br />
South Africa<br />
Gab<strong>on</strong><br />
60<br />
50<br />
40<br />
30<br />
Sierra Le<strong>on</strong>e<br />
Burundi<br />
Eritrea<br />
Zambia<br />
R<br />
20<br />
10<br />
0<br />
Chad<br />
Ethiopia<br />
0 1 2 3 4 5 6<br />
2 = 0.475<br />
Probability of landing rural job<br />
-0.5<br />
0.6<br />
0.5<br />
0.4<br />
0.2<br />
Basic housing<br />
and equipment<br />
Time<br />
Basic housing<br />
Supervisi<strong>on</strong>s<br />
Equipment<br />
Superior housing<br />
Baseline<br />
0<br />
0 0.5 0 1.5 2 2.5 3<br />
Wage b<strong>on</strong>us (as a multiple of base salary)<br />
COMMON<br />
CONSTRAINTS TO<br />
LABOR MARKET<br />
SUPPLY<br />
Low Labor Producti<strong>on</strong>: Health<br />
training instituti<strong>on</strong>s often lack<br />
the physical, technical and<br />
organizati<strong>on</strong>al capacity to produce<br />
larger numbers of <strong>health</strong> workers.<br />
Capacity varies between countries,<br />
with Sudan producing <str<strong>on</strong>g>more</str<strong>on</strong>g> than<br />
3,000 doctors a year, while Zambia<br />
produces fewer than a hundred.<br />
Health training instituti<strong>on</strong>s in most<br />
African countries lack teachers,<br />
teaching supplies, infrastructure,<br />
and sufficient management<br />
capacity.<br />
Preferences <str<strong>on</strong>g>for</str<strong>on</strong>g> Urban and Outof-Country<br />
Employment: Given<br />
comparatively lower salaries and<br />
fewer opportunities at home <str<strong>on</strong>g>for</str<strong>on</strong>g><br />
post-graduate educati<strong>on</strong>, <strong>health</strong><br />
workers often migrate abroad. If<br />
they remain in their own countries,<br />
they tend to prefer urban over<br />
rural jobs, as the <str<strong>on</strong>g>for</str<strong>on</strong>g>mer offer better<br />
income, better educati<strong>on</strong> <str<strong>on</strong>g>for</str<strong>on</strong>g> their<br />
children, and better working/living<br />
c<strong>on</strong>diti<strong>on</strong>s. Figure 3 shows how<br />
the probability of rural job uptake<br />
(in this case <str<strong>on</strong>g>for</str<strong>on</strong>g> nurses in Ethiopia)<br />
is closely linked to the provisi<strong>on</strong><br />
of different types of m<strong>on</strong>etary and<br />
n<strong>on</strong>-m<strong>on</strong>etary incentives. There<br />
are also str<strong>on</strong>g links between the<br />
socioec<strong>on</strong>omic and/or geographic<br />
background of <strong>health</strong> workers<br />
(as well as exposure to rural areas<br />
during training, <str<strong>on</strong>g>for</str<strong>on</strong>g> example) and<br />
their willingness to remain in the<br />
country or work in rural areas<br />
(Lemiere and Herbst et al, 2013).
COMMON<br />
CONSTRAINTS TO<br />
LABOR MARKET<br />
DEMAND<br />
Insufficient Funding <str<strong>on</strong>g>for</str<strong>on</strong>g> Wages:<br />
Wage bill funding is c<strong>on</strong>sidered<br />
insufficient if neither the public<br />
nor private sectors can adequately<br />
absorb <strong>health</strong> workers. This<br />
can occur when there is rapid<br />
scale-up in producti<strong>on</strong>, urban<br />
oversupply (a comm<strong>on</strong> issue), or<br />
reducti<strong>on</strong> in outmigrati<strong>on</strong>, without<br />
c<strong>on</strong>comitant expansi<strong>on</strong> of wage<br />
bill allocati<strong>on</strong>s or private sector<br />
employment opportunities. Rural<br />
areas comm<strong>on</strong>ly suffer from wage<br />
funding insufficiency. Public sector<br />
funding is often disproporti<strong>on</strong>ately<br />
allocated towards urban areas,<br />
where most of the higher-paid<br />
<strong>health</strong> workers are employed and<br />
most of the larger sec<strong>on</strong>dary and<br />
tertiary level hospitals located.<br />
The private <str<strong>on</strong>g>for</str<strong>on</strong>g>-profit sector is<br />
also disproporti<strong>on</strong>ately found in<br />
urban areas.<br />
Fiscal Re-centralizati<strong>on</strong>: In many<br />
countries, n<strong>on</strong>-functi<strong>on</strong>ing or<br />
reversed decentralizati<strong>on</strong> policies<br />
have curtailed local <strong>health</strong><br />
providers’ income and ability to<br />
hire and retain <strong>health</strong> workers. This<br />
is sometimes made worse by rural<br />
<strong>health</strong> facilities being unable to<br />
mobilize discreti<strong>on</strong>ary <strong>resources</strong><br />
of their own, sometimes because<br />
of the limited number of patients<br />
willing or able to purchase services.<br />
In Sudan <str<strong>on</strong>g>for</str<strong>on</strong>g> example, the <str<strong>on</strong>g>more</str<strong>on</strong>g><br />
rural states such as North Kordofan,<br />
Kassala, or Red Sea receive much<br />
less revenue from federal transfers<br />
and own sources than <str<strong>on</strong>g>more</str<strong>on</strong>g> urban<br />
or centrally located states.<br />
Limited Patient Ability to Pay:<br />
Limited revenues particularly from<br />
rural populati<strong>on</strong>s c<strong>on</strong>strain privatesector<br />
demand <str<strong>on</strong>g>for</str<strong>on</strong>g> <strong>health</strong> workers,<br />
and/or public sector income<br />
augmentati<strong>on</strong> opportunities.<br />
Assessments in SSA overwhelmingly<br />
show that rural populati<strong>on</strong>s are<br />
poorer than urban <strong>on</strong>es. Lack<br />
of <strong>health</strong> insurance <str<strong>on</strong>g>for</str<strong>on</strong>g> rural<br />
populati<strong>on</strong>s also prevents them from<br />
buying adequate <strong>health</strong> services and<br />
thus generating rural revenue and<br />
demand <str<strong>on</strong>g>for</str<strong>on</strong>g> HRH (including from the<br />
private sector).<br />
COMMON<br />
PERFORMANCE<br />
ISSUES<br />
Limited Health Worker<br />
Competencies: A critical challenge<br />
many countries face is underdeveloped<br />
competencies of<br />
<strong>health</strong> workers (knowledge<br />
and skills), often because of the<br />
limited physical, technical and<br />
organizati<strong>on</strong>al capacity of <strong>health</strong><br />
training organizati<strong>on</strong>s. Moreover,<br />
in-service training<br />
and c<strong>on</strong>tinuing<br />
development<br />
opportunities are<br />
often lacking or<br />
unevenly available.<br />
Specialist skill<br />
sets, especially<br />
in critical areas<br />
such as obstetrics,<br />
pediatrics, internal<br />
medicine and<br />
infectious diseases<br />
are also often<br />
highly limited<br />
by meager<br />
postgraduate<br />
medical training<br />
opportunities. Where they exist,<br />
such opportunities are often<br />
c<strong>on</strong>centrated <strong>on</strong>ly in urban areas<br />
(with little linkage to the realities<br />
found in many rural areas).<br />
Challenging Working C<strong>on</strong>diti<strong>on</strong>s:<br />
Equipment and supplies shortages<br />
frequently prevent <strong>health</strong> workers<br />
from delivering services adequately,<br />
especially in rural areas, where<br />
inefficient supply chain mechanisms<br />
have <strong>on</strong>ly limited reach. This is<br />
complicated by additi<strong>on</strong>al systems<br />
challenges including poor flow of<br />
in<str<strong>on</strong>g>for</str<strong>on</strong>g>mati<strong>on</strong>, and capacity issues<br />
such as excessive workload, limited<br />
staff and support services, and<br />
infrastructure challenges.<br />
Sub-par Applicati<strong>on</strong> of Ef<str<strong>on</strong>g>for</str<strong>on</strong>g>t: A<br />
comm<strong>on</strong> per<str<strong>on</strong>g>for</str<strong>on</strong>g>mance limitati<strong>on</strong><br />
in many countries is the gap<br />
between what <strong>health</strong> workers know<br />
how to do, and actually do (Figure<br />
4). This “know-do” gap is often<br />
a reflecti<strong>on</strong> of low productivity<br />
levels, <strong>health</strong> worker absenteeism,<br />
and inadequate resp<strong>on</strong>siveness.<br />
The gap is often linked to two<br />
main challenges 1) inadequate or<br />
Figure 4: The Know-do Gap: The gap<br />
between what <strong>health</strong> workers know how<br />
to do, and actually do<br />
Health worker per<str<strong>on</strong>g>for</str<strong>on</strong>g>mance<br />
(process quality)<br />
KNOW-DO GAP<br />
Potential per<str<strong>on</strong>g>for</str<strong>on</strong>g>mance<br />
(knowledge, equipment)<br />
Actual per<str<strong>on</strong>g>for</str<strong>on</strong>g>mance<br />
Le<strong>on</strong>ard at al, (2007)<br />
J of Human Resources<br />
FINANCE AND CAPACITY FOR RESULTS 3
n<strong>on</strong>-functi<strong>on</strong>ing accountability<br />
and supervisi<strong>on</strong> mechanisms<br />
(particularly <str<strong>on</strong>g>for</str<strong>on</strong>g> facility managers<br />
over <strong>health</strong> workers), 2) low<br />
motivati<strong>on</strong> of <strong>health</strong> workers, due<br />
to challenging working and living<br />
c<strong>on</strong>diti<strong>on</strong>s, few opportunities <str<strong>on</strong>g>for</str<strong>on</strong>g><br />
professi<strong>on</strong>al advancement, and few<br />
per<str<strong>on</strong>g>for</str<strong>on</strong>g>mance-linked m<strong>on</strong>etary or<br />
n<strong>on</strong>-m<strong>on</strong>etary incentives.<br />
POLICY IMPLICATIONS<br />
Identify and Address HRH<br />
Leakages. Traditi<strong>on</strong>al approaches<br />
to address the HRH crisis have<br />
focused mainly <strong>on</strong> increasing<br />
producti<strong>on</strong> of <strong>health</strong> workers,<br />
without first paying attenti<strong>on</strong><br />
to <str<strong>on</strong>g>labor</str<strong>on</strong>g> <str<strong>on</strong>g>market</str<strong>on</strong>g> leaks and<br />
inefficiencies. Figure 5 shows<br />
comm<strong>on</strong> <str<strong>on</strong>g>leakages</str<strong>on</strong>g> in Togo because<br />
of outmigrati<strong>on</strong>, unemployment,<br />
and a large rural/urban imbalance.<br />
Only 150 out of 890 doctors trained<br />
actually end up serving 80 percent<br />
of the populati<strong>on</strong>. Of them,<br />
many are absent, unresp<strong>on</strong>sive,<br />
unproductive and unmotivated.<br />
Fixing these inefficiencies and<br />
<str<strong>on</strong>g>leakages</str<strong>on</strong>g> will require identifying<br />
country-specific, cost-effective<br />
strategies and mechanisms that<br />
focus <strong>on</strong> changing <strong>health</strong> worker<br />
behavior through incentives,<br />
QUESTIONS TO AFRICAN MINISTERS<br />
HRH is a critical issue <str<strong>on</strong>g>for</str<strong>on</strong>g> low and<br />
middle income countries aiming to<br />
achieve Universal Health Coverage,<br />
achieve critical <strong>health</strong> outcome<br />
improvements, and foster ec<strong>on</strong>omic<br />
growth.<br />
n What is needed to scale up ef<str<strong>on</strong>g>for</str<strong>on</strong>g>ts to<br />
identify and fix existing inefficiencies<br />
and <str<strong>on</strong>g>leakages</str<strong>on</strong>g> in the <strong>health</strong> <str<strong>on</strong>g>labor</str<strong>on</strong>g><br />
<str<strong>on</strong>g>market</str<strong>on</strong>g>, which will be unique <strong>on</strong> a<br />
country to country basis?<br />
n What would it take to redistribute<br />
funding <str<strong>on</strong>g>for</str<strong>on</strong>g> <strong>health</strong> and other<br />
Figure 5: Loss of Investment in Producti<strong>on</strong> from Leakages -<br />
Example of Togo<br />
Producti<strong>on</strong><br />
890 doctors<br />
trained<br />
Migrati<strong>on</strong>:<br />
250<br />
Source: World Bank, Country Status Report, Togo, 2011<br />
sectors <str<strong>on</strong>g>more</str<strong>on</strong>g> equitably between<br />
urban and rural areas, to improve<br />
rural working and living c<strong>on</strong>diti<strong>on</strong>s<br />
<str<strong>on</strong>g>for</str<strong>on</strong>g> <strong>health</strong> workers and ensure<br />
<strong>resources</strong> exist to hire them?<br />
n What would it take to better<br />
decentralize <strong>health</strong> worker training<br />
to rural areas, and to adopt<br />
educati<strong>on</strong> strategies linked to<br />
reducing outmigrati<strong>on</strong>, better skill<br />
sets to address local challenges,<br />
and increasing rural job uptake?<br />
adopting innovative educati<strong>on</strong><br />
models (including rural pipeline<br />
policies), increasing opportunities<br />
<str<strong>on</strong>g>for</str<strong>on</strong>g> funding <str<strong>on</strong>g>for</str<strong>on</strong>g> HRH (including<br />
<str<strong>on</strong>g>labor</str<strong>on</strong>g> <str<strong>on</strong>g>market</str<strong>on</strong>g> demand) especially in<br />
rural and marginalized areas, and<br />
strengthening management and<br />
accountability systems (particularly<br />
at the facility level).<br />
n How can facility managers be<br />
empowered with better skills,<br />
incentives, decisi<strong>on</strong> making<br />
authority, and tools to raise funding,<br />
so that they can <str<strong>on</strong>g>more</str<strong>on</strong>g> effectively<br />
manage their <strong>health</strong> workers?<br />
n How can the private sector play a<br />
larger role in addressing the HRH<br />
crisis (and shoulder some of the<br />
public sector funding c<strong>on</strong>straints),<br />
and how can its reach and access be<br />
expanded to reach the rural poor?<br />
This brief is a product of the staff of the Internati<strong>on</strong>al Bank <str<strong>on</strong>g>for</str<strong>on</strong>g> Rec<strong>on</strong>structi<strong>on</strong> and Development/The World Bank, prepared ahead of Africa Health Forum 2013: Finance and Capacity <str<strong>on</strong>g>for</str<strong>on</strong>g> Results, an event co-hosted by the World Bank<br />
and the U.S. State Department Office of Global Health Diplomacy, in col<str<strong>on</strong>g>labor</str<strong>on</strong>g>ati<strong>on</strong> with Harm<strong>on</strong>izati<strong>on</strong> <str<strong>on</strong>g>for</str<strong>on</strong>g> Health in Africa. The findings, interpretati<strong>on</strong>s, and c<strong>on</strong>clusi<strong>on</strong>s expressed in this brief do not necessarily reflect the views of the<br />
Executive Directors of the World Bank or the governments they represent, or of any of the hosting entities and partners.<br />
Retired: 20<br />
Unemployed: 20<br />
Employed<br />
full-time in<br />
private <str<strong>on</strong>g>for</str<strong>on</strong>g> profit<br />
sector: 200<br />
Employed<br />
full time in<br />
Government<br />
sector:<br />
400<br />
C<strong>on</strong>centrated in the<br />
capital city (20% of<br />
populati<strong>on</strong>) 75% of<br />
employed doctors<br />
Service 80%<br />
of the populati<strong>on</strong>:<br />
150 doctors