1 national rural health mission pip: 2012-13 mission flexipool
1 national rural health mission pip: 2012-13 mission flexipool
1 national rural health mission pip: 2012-13 mission flexipool

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
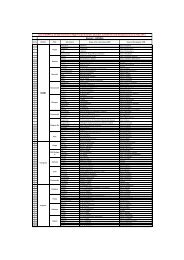
Sr Act. No. Initiative<br />
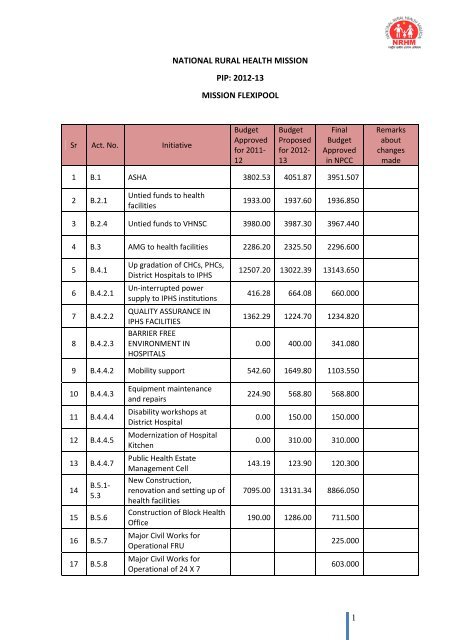
NATIONAL RURAL HEALTH MISSION<br />
PIP: <strong>2012</strong>-<strong>13</strong><br />
MISSION FLEXIPOOL<br />
Budget<br />
Approved<br />
for 2011-<br />
12<br />
Budget<br />
Proposed<br />
for <strong>2012</strong>-<br />
<strong>13</strong><br />
Final<br />
Budget<br />
Approved<br />
in NPCC<br />
1 B.1 ASHA 3802.53 4051.87 3951.507<br />
2 B.2.1<br />
Untied funds to <strong>health</strong><br />
facilities<br />
1933.00 1937.60 1936.850<br />
3 B.2.4 Untied funds to VHNSC 3980.00 3987.30 3967.440<br />
4 B.3 AMG to <strong>health</strong> facilities 2286.20 2325.50 2296.600<br />
5 B.4.1<br />
6 B.4.2.1<br />
7 B.4.2.2<br />
8 B.4.2.3<br />
Up gradation of CHCs, PHCs,<br />
District Hospitals to IPHS<br />
Un-interrupted power<br />
supply to IPHS institutions<br />
QUALITY ASSURANCE IN<br />
IPHS FACILITIES<br />
BARRIER FREE<br />
ENVIRONMENT IN<br />
HOSPITALS<br />
12507.20 <strong>13</strong>022.39 <strong>13</strong>143.650<br />
416.28 664.08 660.000<br />
<strong>13</strong>62.29 1224.70 1234.820<br />
0.00 400.00 341.080<br />
9 B.4.4.2 Mobility support 542.60 1649.80 1103.550<br />
10 B.4.4.3<br />
11 B.4.4.4<br />
12 B.4.4.5<br />
<strong>13</strong> B.4.4.7<br />
14<br />
B.5.1-<br />
5.3<br />
15 B.5.6<br />
16 B.5.7<br />
17 B.5.8<br />
Equipment maintenance<br />
and repairs<br />
Disability workshops at<br />
District Hospital<br />
Modernization of Hospital<br />
Kitchen<br />
Public Health Estate<br />
Management Cell<br />
New Construction,<br />
renovation and setting up of<br />
<strong>health</strong> facilities<br />
Construction of Block Health<br />
Office<br />
Major Civil Works for<br />
Operational FRU<br />
Major Civil Works for<br />
Operational of 24 X 7<br />
224.90 568.80 568.800<br />
0.00 150.00 150.000<br />
0.00 310.00 310.000<br />
143.19 123.90 120.300<br />
7095.00 <strong>13</strong><strong>13</strong>1.34 8866.050<br />
190.00 1286.00 711.500<br />
225.000<br />
603.000<br />
1<br />
Remarks<br />
about<br />
changes<br />
made
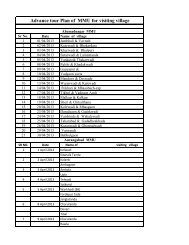
Sr Act. No. Initiative<br />
18 B.5.9<br />
19 B.5.10<br />
20 B.5.11<br />
Civil Works to operationalise<br />
Infection Management and<br />
Environment Protection<br />
Plan (IMEP) at <strong>health</strong><br />
facilities<br />
Strengthening of Training<br />
Infrastructure<br />
Third Party Evaluation of<br />
Civil Works<br />
Budget<br />
Approved<br />
for 2011-<br />
12<br />
Budget<br />
Proposed<br />
for <strong>2012</strong>-<br />
<strong>13</strong><br />
Final<br />
Budget<br />
Approved<br />
in NPCC<br />
123.55 104.70 104.700<br />
1481.60 2459.00 1696.500<br />
0.00 262.00 194.000<br />
21 B.6 Corpus grant to HMS/RKS 2449.00 2457.00 2458.000<br />
22 B.7.1 District Health Action Plans 292.80 370.75 370.750<br />
23<br />
B.8.1 -<br />
B.8.2<br />
24 B.8.4<br />
Constitution and Orientation<br />
of Community leaders and<br />
of VHSC, SHC, PHC, CHC, etc.<br />
Guided tours of MLAs/MLCs<br />
and office bearers of ZPs<br />
<strong>13</strong>7.81 317.70 176.500<br />
56.80 102.60 68.400<br />
25 B.9 Mainstreaming of AYUSH <strong>13</strong>94.82 1240.53 <strong>13</strong>58.<strong>13</strong>0<br />
26 B.10.1 Strengthening of IEC Bureau 83.60 129.00 111.000<br />
27 B.10.3<br />
Implementation of IEC/BCC<br />
Stretagies<br />
1167.81 1088.40 764.400<br />
28 B.10.4 Health Mela 0.00 200.00 64.000<br />
29 B.10.5<br />
Creating awareness on<br />
declining sex ratio<br />
0.00 161.00 161.000<br />
30 B.10.6 Other activities 0.00 274.63 210.630<br />
31 B.11.1 Mobile Medical Units 608.02 932.92 932.920<br />
32<br />
B.12.1 -<br />
B.12.2<br />
33 B.14.3.2<br />
34 B.14.3.4<br />
Emergency and Referral<br />
Services<br />
Organization of epilepsy<br />
camps with the help of<br />
Epilepsy Foundation<br />
Mumbai<br />
Capacity Building and<br />
organization of Epilepsy Day<br />
3076.28 10785.40 1<strong>13</strong>01.400<br />
15.90 68.20 53.900<br />
0.00 25.60 21.600<br />
35 B.14.3.5 Health Advise Call Center 143.00 184.60 86.690<br />
36 B.14.4 NGO Program 516.50 284.40 247.800<br />
2<br />
Remarks<br />
about<br />
changes<br />
made
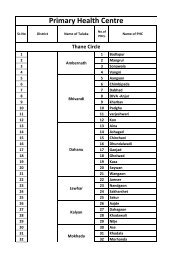
Sr Act. No. Initiative<br />
37 B.15.1<br />
Community based planning<br />
and monitoring (CBM)<br />
Budget<br />
Approved<br />
for 2011-<br />
12<br />
Budget<br />
Proposed<br />
for <strong>2012</strong>-<br />
<strong>13</strong><br />
Final<br />
Budget<br />
Approved<br />
in NPCC<br />
292.10 241.10 234.320<br />
38 B.15.2 Quality Assurance 171.700<br />
39 B.15.3.1 Monitoring and Evaluation 761.57 834.09 765.968<br />
40 B.15.3.2<br />
COMPUTERIZATION OF<br />
HMIS, E-GOVERNANCE & E-<br />
HEALTH<br />
220.00 11<strong>13</strong>.68 11<strong>13</strong>.680<br />
41 B.15.3.3 MCTS 0.00 1963.40 632.354<br />
42 B.15.3.4<br />
43 B.15.3.5<br />
Strengthening of<br />
Supervision and Monitoring<br />
System<br />
Establishment of grievance<br />
Cell<br />
0.00 484.40 484.140<br />
38.40 42.84 42.840<br />
44 B.16 Procurement 2767.82 11180.03 7005.970<br />
45 B.18.1<br />
46 B.19.2<br />
47 B.19.3<br />
State Procurement<br />
Management<br />
Biometric attendance for<br />
<strong>health</strong> staff<br />
Prevention of Sickle cell<br />
Disease<br />
599.60 783.12 783.720<br />
632.52 550.12 397.120<br />
1914.33 1815.26 1815.250<br />
48 B.19.4 Telemedicine 340.02 328.72 328.720<br />
49 B.21.1<br />
Package of Neonatal Care by<br />
ASHA (PNC BY ASHA)<br />
0.00 12.89 12.898<br />
50 B.21.2 Multi centric Birth Cohort 0.00 39.00 39.000<br />
51 B.22 SHSRC 100.00 100.00 100.000<br />
52 B.23.1.1<br />
53 B.23.1.2<br />
54 B.23.1.3<br />
Operationalization of<br />
Superspeciality Hospital for<br />
Child Eye Care<br />
Provision of Hired Vehicle<br />
for Opthalmic Surgeons for<br />
Cataract Operation<br />
Procurement of Ophthalmic<br />
Equipment for Cataract<br />
Operation<br />
0.00 29.88 29.880<br />
0.00 12.90 12.900<br />
0.00 4<strong>13</strong>.05 4<strong>13</strong>.050<br />
55 B.23.3 Support to NVBDCP 0.00 306.99 169.470<br />
3<br />
Remarks<br />
about<br />
changes<br />
made
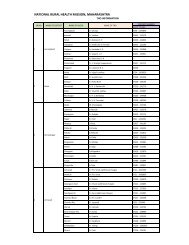
Sr Act. No. Initiative<br />
56 B.23.4<br />
57 B.23.6.1<br />
58 B.23.6.2<br />
Support strengthening<br />
RNTCP<br />
Renovation of Occupational<br />
Therapy and Kitchen<br />
Department in 4 Regional<br />
Mental HOSPITALS – 2 nd<br />
PHASE<br />
Leptospirosis Prevention<br />
And Control<br />
Budget<br />
Approved<br />
for 2011-<br />
12<br />
Budget<br />
Proposed<br />
for <strong>2012</strong>-<br />
<strong>13</strong><br />
Final<br />
Budget<br />
Approved<br />
in NPCC<br />
800.00 810.000<br />
500.00 153.00 153.000<br />
0.00 124.90 124.900<br />
59 B.23.6.3 Support to HIVS 0 249.63 102.500<br />
60 B.23.6.4 Additional Budget for IDSP 0.00 28.32 40.400<br />
61 B.23.6.6 Support to RI 200.00 1466.91 180.330<br />
62 B.23.7 Hematology Program 0.00 486.59 497.760<br />
63 B.23.8<br />
Short term certificate course<br />
for Medical Officers in PHD<br />
0.00 0.00 40.200<br />
64 B.24.2 Maher scheme 66.00 76.00 76.000<br />
65 B.24.4<br />
66 B.24.5<br />
67 B.24.6<br />
68 B.24.8<br />
69 B.24.9<br />
70 B.24.10<br />
71 B.24.11<br />
72 B.24.12<br />
73 B.24.<strong>13</strong><br />
Volunteers to tribal and LEA<br />
PHCs<br />
Mobility support to tribal<br />
institutes<br />
Solar backup in tribal and<br />
LEA <strong>health</strong> institutions<br />
Organization of Specialist<br />
Medical and Dental camps<br />
through Medical Colleges in<br />
tribal areas<br />
Pilot project to Reduce the<br />
IMR in Melghat Region<br />
Co-ordination Cell for tribes<br />
in selected Tribal District<br />
Hospital<br />
Integration of palliative care<br />
in Jawhar tribal block of<br />
Thane district<br />
Establishment of Nutritional<br />
Rehabilitation Center in<br />
tribal areas<br />
Establishment of Medicine<br />
warehouse<br />
24.60 24.60 12.240<br />
496.60 670.30 670.300<br />
595.50 595.50 192.000<br />
231.00 250.20 250.200<br />
96.72 81.92 81.920<br />
28.80 29.52 24.600<br />
<strong>13</strong>.50 <strong>13</strong>.50 <strong>13</strong>.500<br />
41.40 92.16 92.160<br />
1742.23 150.00 150.000<br />
4<br />
Remarks<br />
about<br />
changes<br />
made
Sr Act. No. Initiative<br />
Budget<br />
Approved<br />
for 2011-<br />
12<br />
Budget<br />
Proposed<br />
for <strong>2012</strong>-<br />
<strong>13</strong><br />
Final<br />
Budget<br />
Approved<br />
in NPCC<br />
74 B.24.14 Telemedicine in Tribal areas 0.00 32.45 32.450<br />
75 B.25<br />
Special PIP for Backward<br />
districts<br />
1742.23 4251.34 4251.340<br />
Total 59475.62 96110.01 82921.240<br />
5<br />
Remarks<br />
about<br />
changes<br />
made
SECTION - B.1: ACCREDITED SOCIAL HEALTH ACTIVIST (ASHA)<br />
A trained female community <strong>health</strong> worker called as Accredited Social Health Activist (ASHA)<br />
is being provided to tribal as well as non-tribal areas in the approximate ratio of one per 1000<br />
population.<br />
Year of starting<br />
the scheme<br />
2007-08<br />
(old scheme)<br />
SUMMARY INFORMATION OF THE SCHEME / INITIATIVE<br />
Budget sanctioned<br />
for year 2011-12<br />
Budget proposed<br />
for year <strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed in<br />
NPCC<br />
6<br />
Remarks<br />
3802.53 4051.87 3951.507 -<br />
SUB SECTION – B.1.1 SELECTION AND TRAINING OF ASHA<br />
Selection of ASHA<br />
Sir Area Target Appointed<br />
%<br />
Appointed<br />
1 Tribal areas 9523 9523 100<br />
2 Non-tribal areas 49861 49766 99.80<br />
Total 59384 59289 99.28<br />
As mentioned above total 59289 ASHA are appointed in Maharashtra by December <strong>2012</strong>.<br />
Training<br />
Training of ASHA has been initiated as per GOI guidelines through a cascade model. In Tribal<br />
areas of Maharashtra, first two phases of the training of ASHA under HBNC VI & VII Module is<br />
almost completed and State is planning to undergo training of HBNC in Non –tribal areas of<br />
Maharashtra from <strong>2012</strong>-<strong>13</strong>.<br />
Module wise status of training in tribal and non-tribal areas is mentioned below:
Module<br />
Table -: ASHA training status of Maharashtra state as on December 2011<br />
Tribal areas<br />
%<br />
Non-tribal areas<br />
%<br />
Total (Tribal+<br />
Nontribal)<br />
Target Achiev e Target Achiev e Target Achiev e %<br />
Module – I 9523 9523 100 49766 49405 99 59289 58928 99<br />
Module – II 9523 9501 100 49766 48024 96 59289 57525 97<br />
Module – III 9523 9388 99 49766 45712 92 59289 55100 93<br />
Module – VI 9523 9098 96 49766 26502 53 59289 35600 60<br />
Module – V 9523 8812 93 49766 1289 0 59289 10101 17<br />
Module – VI &<br />
VII (First Phase)<br />
Module – VI &<br />
VII (Second<br />
Phase)<br />
9523 7776 82<br />
9523 1588 17<br />
9523 7776 82<br />
9523 1588 17<br />
Budget requirement for training of ASHA and support staff<br />
ASHA training will require budget for Training of Trainers (ToT) and actual training of ASHA.<br />
Total budget required will be as follows:<br />
Sir Module<br />
Table -: Budget required for ToT – <strong>2012</strong>-<strong>13</strong><br />
No. of ASHA trainers to be trained in<br />
<strong>2012</strong>-<strong>13</strong><br />
Tribal Non-tribal Total<br />
Budget<br />
required<br />
/ASHA<br />
7<br />
Rs. In Lakhs<br />
Total<br />
budget<br />
required<br />
1 Module – I 0 0 0 0.017 0<br />
2 Module – II 0 0 0 0.017 0<br />
3 Module – III 0 0 0 0.017 0<br />
4 Module – IV 0 0 0 0.017 0<br />
5 Module – V 0 0 0 0.017 0<br />
6 Module – VI 330 664 994 0.077 76.538<br />
Total<br />
Budget required for training of ASHA is mentioned in table below:<br />
76.538
Sir<br />
Module<br />
Table -: Budget required for training of ASHA – <strong>2012</strong>-<strong>13</strong><br />
8<br />
Rs. In Lakhs<br />
No. of ASHA to be trained in<br />
<strong>2012</strong>-<strong>13</strong> Total<br />
Tribal Non-tribal Total<br />
Budget<br />
required<br />
/trainee<br />
budget<br />
required<br />
1 Module – I 50 100 150 0.02 3<br />
2 Module – II 50 100 150 0.014 2.1<br />
3 Module – III 50 100 150 0.014 2.1<br />
4 Module – IV 50 2000 2050 0.014 28.7<br />
5 Module – V 300 5000 5300 0.014 74.2<br />
6<br />
7<br />
8<br />
9<br />
Module – VI & VII<br />
(1st Phase)<br />
Module – VI & VII<br />
(2nd Phase)<br />
Module – VI & VII<br />
(3rd Phase)<br />
Module – VI & VII<br />
(4th Phase)<br />
Total<br />
Training of Block Facilitators and Block Community Mobilizes<br />
100 25000 25100 0.021 527.1<br />
500 5000 5500 0.021 115.5<br />
5000 0 5000 0.021 105<br />
3000 0 3000 0.021 63<br />
920.7<br />
Training of Block Facilitators and Block Community Mobilizes is to be conducted for 6 th and 7 th<br />
Module. Budget required for this training is as follows:<br />
Sir Category<br />
Table – Training of Block Facilitator<br />
No. of ASHA to be trained<br />
for Module VI & VII<br />
Tribal Non-<br />
Total<br />
tribal<br />
Budget<br />
required<br />
/trainee<br />
Rs. In Lakhs<br />
Total<br />
budget<br />
required<br />
1<br />
Block Community Mobiliser (First<br />
Phase)<br />
10 100 110 0.025 2.75<br />
2<br />
Block Community Mobiliser (Second<br />
Phase)<br />
50 50 100 0.025 2.5<br />
3<br />
Block Community Mobiliser (Third<br />
Phase)<br />
50 0 50 0.025 1.25<br />
4 Block Facilitator (First Phase) 100 800 900 0.025 22.5<br />
5 Block Facilitator (Second Phase) 600 800 1400 0.025 35
6 Block Facilitator (Third Phase) 500 0 500 0.025 12.5<br />
Total 76.5<br />
Total budget required for training of ASHA<br />
Total budget required for ASHA training include budget for ToT and budget for actual training<br />
of ASHA. Total budget required is mentioned in table below:<br />
Table -: Budget required for training of ASHA (Tribal and Non-tribal areas)<br />
Sir<br />
In Lakhs<br />
Particulars Budget<br />
1 ToT for ASHA 76.538<br />
2 ASHA training – tribal and non-tribal all modules 920.7<br />
3 Training of Block Community Mobiliser and Block Facilitator 76.5<br />
Total 1073.74<br />
The budget requested is on the assumption about per batch expenditure as mentioned in<br />
table above. However, the actual budget requirement may vary. If additional budget is<br />
required, that will be managed from savings of ASHA or other schemes.<br />
SUBSECTION - B.1.2 : MEDICINE FOR ASHA<br />
The medicines in the ASHA kits are revised as per GOI guidelines. Following list of medicines<br />
are proposed for ASHA kits. The quantity will be decided by the state level committee keeping<br />
in view the prices of the this medicines and limiting the price of the ASHA medicine kit to<br />
Rs.600 per kit-<br />
List of Drugs provided in ASHA Kit<br />
Sr. Medicines<br />
1 DDK for Clean deliveries at home<br />
2 Tab. Iron Folic Acid (L)<br />
3 Tab Punarvadu Mandur (ISM Preparation of Iron)<br />
4 ORS Packets<br />
5 Tab. Paracetamol<br />
6 Tab. Dicyclomine<br />
7 Povidine Ointment Tube<br />
8 Thermometers<br />
9 Cotton Absorbent Roll<br />
9<br />
Rs.
10 Bandages, 4cm X 4 meters<br />
11 Tab.Chloroquine<br />
12 Condoms<br />
<strong>13</strong> Oral Pills (In cycles)<br />
Number of kits and budget required for year <strong>2012</strong>-<strong>13</strong> is as follows:<br />
Table -: Budget required for ASHA medicine kit<br />
Rs.<br />
In Lakhs<br />
Total budget<br />
Sr. Area Unit price No. of kits required required<br />
1 Tribal areas 0.006 9523 57.<strong>13</strong>8<br />
2 Non-tribal areas 0.006 49483 296.898<br />
Total 59289 354.036<br />
SUBSECTION - B.1.3 TO B.1.6: INCENTIVE TO ASHA UNDER JSY, FW SERVICES, CHILD HEALTH<br />
AND OTHER INCENTIVES<br />
It is proposed to provide performance based incentive to ASHA through PHCs during monthly<br />
orientation meetings. The incentive is being provided by Cheque. Rates of ASHA incentive and<br />
budget source are as follows:<br />
Table: Performance incentives to ASHA<br />
No Activity Incentive rate<br />
1 a<br />
1 b<br />
2<br />
3<br />
JSY delivery in PHC or any recognized<br />
hospital<br />
( Tribal area)<br />
JSY delivery in PHC or any recognized<br />
hospital<br />
(Non-Tribal Areas)<br />
Motivation of BPL/SC/ST beneficiary<br />
for tubectomy<br />
Motivation of any beneficiary for<br />
vasectomy<br />
Rs. 350/- per delivery (with<br />
conditions of JSY for Tribal<br />
areas<br />
Rs. 200/- per delivery (with<br />
conditions of JSY for Non-<br />
Tribal areas.<br />
Budget<br />
Resource<br />
10<br />
RCH<br />
RCH<br />
Rs. 150/- per operation RCH<br />
Rs. 200/- per operation RCH<br />
4 Completion of DOTS (RNTCP) Rs. 250/-Case completed RNTCP<br />
5<br />
Radical treatment of malaria Positive<br />
case<br />
Per slide Rs.5/- for<br />
preparation of Blood Slide<br />
Malaria<br />
Per case Rs.20/ for treating Malaria
No Activity Incentive rate<br />
6 Leprosy treatment<br />
7 Control of epidemic (outbreak)<br />
8 Control of epidemic (dehydrated)<br />
Bringing pregnant women for HIV<br />
9<br />
testing in PPTCT centers<br />
Registration of positive pregnant<br />
10 mother at Anti Retro-Virus Treatment<br />
center<br />
11 Ad<strong>mission</strong> of HIV +ve mother for<br />
delivery in PPTCT center<br />
Follow up of HIV positive mothers at 6<br />
12 week, 6 th Month and 18 th month (or as<br />
recommended by MSACS)<br />
Referring for RTI (Reproductive Tract<br />
<strong>13</strong> Infection) / STI (Sexually Transmitted<br />
Infection) to SC/PHC/RH/SDH/DH<br />
Referring for Clubfoot Newborn to<br />
14<br />
SC/PHC/RH/SDH/DH level<br />
Referring for Clubfoot Newborn to<br />
15 further treatment at District Hospital.<br />
(after PHC MO Diagnosis)<br />
Per month Immunization at Village<br />
16<br />
Level<br />
Quarterly Meeting of ASHA on<br />
17<br />
Immunization (Yearly 4)<br />
Informed AEFI ( Adverse Event<br />
18<br />
Following Immunization) case to<br />
PF positive case<br />
Per case Rs.50/- for treating<br />
PV positive case<br />
Rs. 100/ - for newly<br />
detected case<br />
Rs. 400 – MB case<br />
completing treatment<br />
Rs. 200 – PB case<br />
completing treatment<br />
Rs. 100/- for giving first<br />
hand information of<br />
outbreak<br />
Rs. 50/- per case for timely<br />
referral of dehydrated<br />
patient to PHC/RH/DH<br />
Rs.50/- per mother<br />
Rs.200/- per mother<br />
Rs. 1000/- to ASHA<br />
Rs. 750/- per follow up<br />
Rs. 200/-<br />
Rs. 100/-<br />
Rs. 500/-<br />
Budget<br />
Resource<br />
11<br />
Malaria<br />
NLEP<br />
NLEP<br />
NLEP<br />
Mission-<br />
Flexipool<br />
Mission-<br />
Flexipool<br />
Mission-<br />
Flexipool<br />
Mission-<br />
Flexipool<br />
Mission-<br />
Flexipool<br />
Mission-<br />
Flexipool<br />
Mission-<br />
Flexipool<br />
Mission-<br />
Flexipool<br />
Mission-<br />
Flexipool<br />
Rs.75/- RI Fund<br />
Rs.75/- RI Fund<br />
Rs.50/-<br />
Mission<br />
Flexipool
No Activity Incentive rate<br />
19<br />
SC/PHC<br />
Motivation of community for toilet<br />
construction<br />
20 Birth Information (SC/PHC)<br />
21<br />
22<br />
23<br />
24<br />
25<br />
Registration of Birth including issuing<br />
birth certificate (with or without child<br />
name)<br />
Death Information (SC/PHC) of Age<br />
group 0 to 5 child<br />
Incentive to ASHA for Death certificate<br />
(Age group 0 to 5 child)<br />
Incentive to ASHA for information of<br />
women death for the age group<br />
between 15 to 49 years<br />
Incentive to ASHA for recording of<br />
Maternal death for the age group<br />
between 15 to 49 years<br />
26 Yearly Immunization<br />
27<br />
28<br />
29A<br />
29B<br />
Bringing critically ill child to hospital<br />
(for tribal areas only)<br />
Sickle Cell control program (<br />
Amaravati, Dhule, Nanded, Akola,<br />
Washim, Buldhana, Aurangabad,<br />
Jalgaon, Raigad)<br />
To give information about sickle cell<br />
Disease in Gram sabha (Two<br />
gramsabha in a year )<br />
To motivates Self help groups,<br />
adolescent girls and boys<br />
Rs. 50/-toilet construct<br />
Rs.20/- per Birth<br />
information<br />
Rs.30/- per Birth<br />
Registration<br />
Rs.75/- per information<br />
Rs.50/- per certificate<br />
Rs.100/-<br />
Rs.500/-<br />
For fully immunized<br />
children: Rs. 1000/-for<br />
100% immunization<br />
Rs. 750 if 90%<br />
immunization<br />
Rs. 50/- per child<br />
Rs. 50/- per ASHA per<br />
Gramsabha<br />
Budget<br />
Resource<br />
Total<br />
Sanitation<br />
Campaign<br />
Mission -<br />
Flexipool<br />
Mission -<br />
Flexipool<br />
Mission -<br />
Flexipool<br />
Mission -<br />
Flexipool<br />
Mission -<br />
Flexipool<br />
Mission -<br />
Flexipool<br />
Mission -<br />
Flexipool<br />
Mission -<br />
Flexipool<br />
Mission -<br />
Flexipool<br />
12<br />
Sickle Cell Fund<br />
Rs.40/- per meeting Sickle Cell Fund<br />
29C Solubility test Rs. 5/- per test Sickle Cell Fund<br />
29D Red & Yellow card distribution Rs.20/- per card Sickle Cell Fund<br />
29E Follow up to sufferer patient’s Rs.15/- per visit Sickle Cell Fund<br />
29F Incentives for successful marriage Rs.1000/- per marriage Sickle Cell Fund
No Activity Incentive rate<br />
prevention prevented<br />
Budget<br />
Resource<br />
30 Cataract operations<br />
Rs. 100/- per patient for<br />
transport<br />
NPCB<br />
Rs. 75/- per patient for IEC NPCB<br />
31 HBNC (As per GOI guidelines) Rs.250/- per New born<br />
Mission<br />
Flexipool<br />
32<br />
33<br />
Follow Up of Discharge Children From<br />
NRC<br />
Promotion of menstrual hygiene<br />
scheme<br />
Rs.50 /- per follow up (Total<br />
4 follow up)<br />
Mission<br />
Flexipool<br />
a Number of sanitary napkin soled Rs.1/- per napkin Sale of Napkin<br />
b<br />
34<br />
a<br />
35<br />
Number of meeting of adolances girl<br />
organized (one per month)<br />
Hemophilia and Thalassemia disease<br />
Program (Nagpur, Nashik, Amravati,<br />
Pune)<br />
ASHAs provided IEC about Hemophilia<br />
and Thalassemia disease to Gram<br />
Sabha, 4 sessions per year<br />
Plus Polio Immunization Campaign<br />
(IPPI)<br />
Rs.50/- per meeting<br />
Rs. 50/- per session/<br />
GramSabha<br />
Rs. 75/- per day (4days) for<br />
Home visits & Polio booth<br />
activities<br />
Rs. 20/- per day (4days) TA<br />
(As per Central Government<br />
Guideline)<br />
Untied Fund of<br />
Sub Centre<br />
Mission-<br />
Flexipool<br />
<strong>13</strong><br />
Plus Polio<br />
Total performance of ASHA during month is recorded in one register and ASHA is paid based<br />
on this record.<br />
Budget required for performance based incentive<br />
Budget required for ASHA incentive as per the activities, rates and source through NRHM<br />
Mission Flexi-pool is as follows:<br />
Table -: Budget requirement for performance based incentives to ASHA<br />
Rs. In Lakhs<br />
Area incentive/ASHA No of ASHA<br />
Total budget<br />
required<br />
Tribal areas 0.01 9523 95.23
Area incentive/ASHA No of ASHA<br />
Non-tribal<br />
areas<br />
Total budget<br />
required<br />
0.005 49766 248.83<br />
Total 59289 344.06<br />
Table -: Budget requirement for HBNC<br />
Sr. Area Incentive /ASHA No of ASHA<br />
Rs. In Lakhs<br />
Total budget<br />
required<br />
1 Tribal areas 0.01 9523 95.23<br />
2 Non-tribal areas 0.005 20000 100<br />
Total 29523 195.23<br />
Table -: Total Budget requirement for performance based incentives to ASHA<br />
Rs. In Lakhs<br />
Sr. Area Incentive /ASHA<br />
1 Tribal areas 190.46<br />
2 Non-tribal areas 348.83<br />
Total 539.29<br />
Each ASHA is provided one register for entering the work done during month. Performance<br />
based incentive is paid to ASHA during monthly meeting along with meeting stipend. During<br />
<strong>2012</strong>-<strong>13</strong>, it is proposed to pay the incentive to ASHA by account payee cheques by the PHCs.<br />
SUBSECTION – B.1.7: AWARDS TO ASHA<br />
ASHA are increasingly taking part in majority of the <strong>health</strong> services provided to patients,<br />
particularly in tribal and inaccessible areas. It is proposed to give awards to good functioning<br />
ASHAs.<br />
For provision of awards, the criteria will be: ASHA with good record keeping, consistent<br />
performance and higher compensation. In one district 3 ASHA at district level and 2 ASHA per<br />
block,<br />
Considering there are 33 districts, 353 blocks budget required for this activity will be as<br />
follows:<br />
Sir<br />
No<br />
Type of Award<br />
Award<br />
Amount<br />
No. of units<br />
14<br />
Total Budget<br />
Required<br />
1 District Level (3ASHA ×33 dist= 99) 0.26 33 Districts 8.58<br />
2 Block Level (2ASHA×353 Block=706) 0.14 353 Blocks 49.42<br />
4 Function at District Level 0.25 33 Districts 8.25<br />
Total 66.25
SUBSECTION - B.1.8 : SUPPORT MECHANISM FOR ASHA<br />
Considering the services expected to be delivered, ASHA needs to get support from village,<br />
various <strong>health</strong> functionaries, <strong>health</strong> institutions, PRI, RKS, local self help groups, etc.<br />
Therefore a strong network has been developed amongst all the stakeholders. NRHM has<br />
published guidelines regarding support mechanism for ASHA. Maharashtra has developed<br />
support mechanism as per the guidelines. Salient features of support mechanism are as<br />
follows:<br />
• Appointment of Program Managers (ASHA) and at all District HQ<br />
• Appointment of Block Facilitator @ one per 10 ASHA in tribal and one per PHC in nontribal<br />
areas.<br />
• Quality improvement in monthly reorientation meeting at all PHCs.<br />
Budget Requirement<br />
Budget required for support mechanism is as follows:<br />
Table -: Budget required for ASHA support mechanism<br />
Sir Particulars<br />
Budget<br />
/ unit<br />
Total<br />
Units<br />
15<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
A State level<br />
1 Salary/TA of Program Manager 3.6 1 3.6<br />
2 Salary of Data Assistant 1.32 1 1.32<br />
3 Salary of Statistical Investigator 1.15 1 1.15<br />
State total 6.07<br />
B District Level<br />
1<br />
Salary TA/DA of Community Mobiliser (Rs.<br />
12500/PM)<br />
1.7 33 56.1<br />
3 Contingency 0.2 33 6.6<br />
4<br />
Block Community Mobiliser Bi-monthly Meeting at<br />
District Level<br />
0.06 33 1.98<br />
District Total 64.68<br />
C Block Level<br />
1 Block level contingency 0.02 353 7.06<br />
2 Block Community Mobiliser (salary + TA/DA) - Tribal 1 50 50<br />
Block Community Mobiliser (salary + TA/DA) - Non-<br />
Tribal<br />
1 50 50<br />
Block total 107.06<br />
D PHC Level<br />
1 Block Facilitator (1/PHC) 25 visits/PM Rs. 150/visit 0.45 1500 675<br />
2 Block Facilitator Monthly meeting (12), Rs. 0.018 1500 27
Sir Particulars<br />
3<br />
150/meeting<br />
ASHA Software contingency to Block Facilitator ( 315<br />
Tribal PHC & 1494 Non-Tribal PHC) Outsourcing of<br />
data entry<br />
Budget<br />
/ unit<br />
Total<br />
Units<br />
16<br />
Budget<br />
required<br />
0.005 1809 9.045<br />
4 ASHA meeting (Rs.150/-) 0.018 47500 855<br />
5 Honorarium to MO for reorientation 0.024 1809 43.416<br />
6 LHV Honorarium 0.06 1809 108.54<br />
7 Contingency 0.01 1809 18.09<br />
PHC Total 1736.091<br />
Grand Total 19<strong>13</strong>.901<br />
SUBSECTION - B.1.9 : ASHA MENTORING GROUP<br />
NRHM has instructed to establish ASHA mentoring groups at state, districts and block level.<br />
State level mentoring group is responsible for policy decisions regarding ASHA. District level<br />
group is involved in planning, implementation and monitoring of the ASHA program. Block<br />
level group is mainly responsible for implementation and monitoring of the program.<br />
Budget requirement for ASHA mentoring group is as mentioned in table below:<br />
Table :- Budget required for ASHA Monitoring group <strong>2012</strong>-<strong>13</strong><br />
Rs. In Lakhs<br />
Sir Level<br />
Unit<br />
cost<br />
State Level<br />
No.<br />
of Budget<br />
units required<br />
Tribal areas<br />
No. of Budget<br />
units required<br />
Non-tribal areas<br />
No.<br />
of Budget<br />
units required<br />
Total<br />
Budget<br />
required<br />
1 State level 0.05 2 0.1 0 0 0 0 0.1<br />
2 District<br />
Level 0.02 0 0 15 0.3 18 0.36 0.66<br />
3 Block level 0.01 0 0 70 0.7 283 2.83 3.53<br />
Total 0.1 1 3.19 4.29<br />
SUMMARY OF ASHA BUDGET REQUIREMENT<br />
Total budget required for ASHA scheme for year <strong>2012</strong>-<strong>13</strong> is mentioned in table below:
Table -: Total budget requirement for ASHA scheme<br />
17<br />
Rs. In Lakhs<br />
Sir Particulars<br />
Budget proposed<br />
for <strong>2012</strong>-<strong>13</strong><br />
1 Selection and Training of ASHA 1073.74<br />
2 Medicine Kit 354.036<br />
3 Performance Incentive 539.29<br />
4 ASHA Award 66.25<br />
5 Support Mechanism 19<strong>13</strong>.901<br />
6 ASHA Mentoring Group 4.29<br />
Total 3951.507<br />
SECTION - B.2 : UNTIED FUNDS<br />
SUB-SECTION - B.2.1 TO B.2.3 : UNTIED FUNDS TO HEALTH FACILITIES (CHC/PHC/APHC/SC)<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2006-07 1935.35 1933.00 1937.60 1936.850<br />
Rs. in Lakhs<br />
Remarks<br />
Health Sector reforms under NRHM aim to increase functional, administrative and financial<br />
resources and autonomy to the field units under which every <strong>health</strong> institution from Subcentre<br />
to SDH will get untied grants for any additional activities.<br />
Necessity of untied funds has been felt mainly due to unavailability of funds for undertaking<br />
innovative centre-specific need based activity as allotment of funds to institutions has<br />
traditionally been of the nature of untied funds for implementation of particular activity /<br />
scheme and this hardly left any fund with the public <strong>health</strong> facility.<br />
Regarding addition of SDH/GH/WH for untied funds, explanation is as follows:<br />
CHC scheme was introduced in Maharashtra in 1980s. That time CHCs were established in the<br />
State as per GoI norms but renamed as Rural Hospitals. No. of beds, Staffing pattern,<br />
infrastructure, service delivery system, everything is as per GoI norms of CHC, only the name<br />
is changed to Rural Hospital. Maharashtra Health Systems Development Project was<br />
introduced in the State in 1998. Some of the CHCs (RH) were upgraded to 200 beds, 100 beds<br />
and 50 beds with addition of specialities. To differentiate them from Rural Hospital, names<br />
were changed to General Hospital (200 beds) and Sub-District Hospital (50 and 100 beds).<br />
Catchment area and basic structure of these hospitals is same as Rural Hospital or CHC. All
these hospitals have functional RKS. As these hospitals are considered in CHC group it is<br />
requested to sanction Untied funds to all the Hospitals. For convenience, all these hospials<br />
are separately shown in grant distribution in table below.<br />
Regarding addition of APHC, explanation is as follows:<br />
In Maharashtra there are 795 <strong>health</strong> facilities which are between Sub-Center and PHCs. One<br />
doctor, one nurse, one Pharmacist and one attendant is posted in these <strong>health</strong> facilities which<br />
are called either dispensaries or APHC. Normally these centers are situated in medium size<br />
villages. These centers do not provide emergency services and FW operation services. Except<br />
this all the services including immunization, delivery, IUD, RNTCP and other Disease Control<br />
Program Services beside curative services are provided by APHC. Considering this, it is<br />
requested to sanction Untied funds to APHCs.<br />
One more hospital is started at Bhivandi District Thane. Therefore number of CHCs is now<br />
458. Budget is requested for 458 CHC level hospitals.<br />
List of all the <strong>health</strong> facilities for UF is submitted in Annexure.<br />
Grant distribution<br />
During year 2011-12, untied grants have been distributed to all the Sub-Centers, Primary<br />
Health Centers, Rural Hospitals & Sub District Hospitals in the state. Untied grant to Sub-<br />
Centers have been released to the account jointly operated by Sarpanch of SHC village and<br />
ANM. Untied grants of other <strong>health</strong> institutions are released to RKS. Similarly, for year <strong>2012</strong>-<br />
<strong>13</strong>, untied funds are to be released to all <strong>health</strong> facilities as follows:<br />
Table – : Budget required for untied grants <strong>2012</strong>-<strong>13</strong><br />
Rs. In Lakhs<br />
Budget required<br />
No. of<br />
Total<br />
Sir Type of hospital institutions<br />
Unit rate budget<br />
eligible<br />
required<br />
1 Sub-Centre 10566 0.1 1056.6<br />
2 APHC 795 0.25 198.75<br />
3 PHC 1810 0.25 452.5<br />
4 RH (30 beds) 366 0.5 183<br />
5 SDH (50 beds) 56 0.5 28<br />
6 SDH (100 beds) 23 0.5 11.5<br />
7 WH (60-335 beds) 9 0.5 4.5<br />
8 GH (200 beds) 4 0.5 2<br />
Total <strong>13</strong>629 1936.85<br />
18
SUB-SECTION - B.2.4 : VILLAGE HEALTH SANITATION WATER SUPPLY AND NUTRITION<br />
COMMITTEE<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2006-07 4070.8 3980 3987.30 3967.440<br />
19<br />
Rs. in Lakhs<br />
Remarks<br />
VHNSC are established in every revenue village. VHC is provided with untied fund which has<br />
to be utilized for IEC, household survey, preparation of <strong>health</strong> register, organization of<br />
meetings at village level, etc. Untied fund is made available through NRHM Flexible Pool<br />
Fund.<br />
Norm of GoI for Untied fund to VHNSC is Rs. 10000/village. Same amount of fund is<br />
distributed all revenue villages irrespective of the population. Thus, revenue villages with<br />
population less than 500 or more than 10000 gets same amount of fund. Therefore it is<br />
proposed that, Maharashtra will request the funds from GoI based on population criteria.<br />
Out of total villages available in the state, VHNSC is established in 39872 villages in the State<br />
as on 31.3.<strong>2012</strong>. Number is increased from last sub<strong>mission</strong> due to addition of new villages.<br />
Budget is requested for all these 39872 villages. In addition to this, there are 73 forest<br />
villages. Forest village function as normal revenue village. They have Village Panchayat, they<br />
vote for PRI members and are included for all the development work. Only difference of these<br />
villages is that they are situated on forest land so are not declared as revenue villages. These<br />
villages are in maximum need of VHNSC funds but are deprived of that. Therefore, it is<br />
requested to add these villages in VHNSC list.<br />
Budget requirement of untied fund for VHNSC as follows:<br />
Sr.No.<br />
Table - Budget requirement to Village Health Committee<br />
VHNSC<br />
committees<br />
established in<br />
Revenue<br />
Villages<br />
1 39945<br />
Population<br />
wise Norms<br />
Population<br />
wise No. Of<br />
Villages<br />
Budget<br />
proposed per<br />
village<br />
Rs. In Lakhs<br />
Total PIP<br />
0-500 8122 0.05 406.10<br />
501-1500 19673 0.08 1573.84<br />
1501-5000 10548 0.15 1582.20
Sr.No.<br />
VHNSC<br />
committees<br />
established in<br />
Revenue<br />
Villages<br />
Population<br />
wise Norms<br />
Population<br />
wise No. Of<br />
Villages<br />
Budget<br />
proposed per<br />
village<br />
20<br />
Total PIP<br />
5001-10000 1255 0.24 301.20<br />
10000+ 347 0.30 104.10<br />
Total 39945 0.82 3967.44
SECTION - B.3 : ANNUAL MAINTENANCE GRANTS (AMG)<br />
SUBSECTION - B.3.1 TO B.3.4 : ANNUAL MAINTENANCE GRANTS TO HEALTH FACILITIES<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2006-07 2497.2 2286.2 2325.5 2296.600<br />
21<br />
Rs. in Lakhs<br />
Remarks<br />
Annual Maintenance Grants are distributed for maintenance of physical infrastructure of<br />
<strong>health</strong> institutions. GOI has directed to use the grant for regular maintenance of physical<br />
structures of <strong>health</strong> institutions including provision of water, toilets, their use and their<br />
maintenance.<br />
As mentioned in GOI guidelines, distribution of AMG is proposed in Sub-Centers, PHUs,<br />
Primary Health Centers and Rural Hospitals of the state functioning in own building.<br />
Regarding addition of SDH/GH/WH for AMG, explanation is as follows:<br />
CHC scheme was introduced in Maharashtra in 1980s. That time CHCs were established in the<br />
State as per GoI norms but renamed as Rural Hospitals. No. of beds, Staffing pattern,<br />
infrastructure, service delivery system, everything is as per GoI norms of CHC, only the name<br />
is changed to Rural Hospital. Maharashtra Health Systems Development Project was<br />
introduced in the State in 1998. Some of the CHCs (RH) were upgraded to 200 beds, 100 beds<br />
and 50 beds with addition of specialities. To differentiate them from Rural Hospital, names<br />
were changed to General Hospital (200 beds) and Sub-District Hospital (50 and 100 beds).<br />
Catchment area and basic structure of these hospitals is same as Rural Hospital or CHC. All<br />
these hospitals have functional RKS. As these hospitals are considered in CHC group it is<br />
requested to sanction AMG to all the Hospitals.<br />
List of Hospials submitted in Annexure<br />
List of PHCs is submitted in Annexure.<br />
In Maharashtra there are 795 <strong>health</strong> facilities which are between Sub-Center and PHCs. One<br />
doctor, one nurse, one Pharmacist and one attendant is posted in these <strong>health</strong> facilities which<br />
are called either dispensaries or APHC. Normally these centers are situated in medium size<br />
villages. These center do not provide emergency services and FW operation services. Except<br />
this all the services including immunization, delivery, IUD, RNTCP and other Disease Control<br />
Program Services beside curative services are provided by APHC. Considering this, it is<br />
requested to sanction AMG to APHCs.
List of APHC is submitted in Annexure.<br />
List of Sub-Centers submitted in Annexure.<br />
Budget requirement for AMG for year <strong>2012</strong>-<strong>13</strong> is given in table below.<br />
Table – : Budget required for Annual Maintenance Grants – <strong>2012</strong>-<strong>13</strong><br />
22<br />
Rs. In Lakh<br />
Sir Type of <strong>health</strong> institution<br />
No. of<br />
institutions<br />
No. in<br />
own<br />
building<br />
AMG<br />
Budget<br />
Unit rate<br />
required<br />
1 Sub-Centre 10566 8286 0.1 828.60<br />
2 APHC (PHU) 795 480 0.5 240.00<br />
2 PHC 1810 1614 0.5 807.00<br />
3 CHC 458 421 1.00 421.00<br />
Total <strong>13</strong>629 10801 2296.60
SECTION - B.4 : HOSPITAL STRENGTHNING<br />
SUBSECTION - B.4.1.1 TO B.4.1.4 : UPGRADING HEALTH FACILITIES TO IPHS<br />
Year of<br />
starting the<br />
scheme/<br />
initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year 2011-<br />
12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed in<br />
NPCC<br />
2008-09 12960.8 12507.20 <strong>13</strong>022.39 <strong>13</strong>143.650<br />
23<br />
Rs. in Lakhs<br />
Remarks<br />
Maharashtra has started upgrading the <strong>health</strong> institutions to IPHS since last three years. As<br />
per GoI timeline, all the facilities are to be upgraded to IPHS by 2010-11. However, because of<br />
want of manpower and infrastructure, it is becoming difficult to upgrade the <strong>health</strong> facilities<br />
in large scale. Therefore selected facilities fulfilling basic criteria are considered for up<br />
gradation. Once these facilities are upgraded, new facilities will be taken up.<br />
Scheme of up gradation<br />
IPHS up gradation is being carried out in Phases. Health Facilities willing for upgradation are<br />
screened for following criteria :<br />
Table : Criteria for designating <strong>health</strong> facility for IPHS Upgradation<br />
Sub Center PHC Hospitals excluding<br />
DH<br />
Own building Own building Own building Own Building<br />
Post of ANM filled in At least one MO<br />
MBBS<br />
Post of MPW (M)<br />
filled in<br />
At least 3 deliveries<br />
per month<br />
OT, labour room and<br />
Laboratory functional<br />
At least 10 deliveries<br />
per month in building<br />
Availability of at least<br />
three specialists<br />
(OBGY, Pediatrics &<br />
Anesthesia) on<br />
regular or contract<br />
basis<br />
Blood Storage Unit<br />
functional<br />
At least 30 deliveries<br />
/month. Cesarean<br />
Section and neonatal<br />
DH<br />
Availability of at least<br />
five specialities<br />
(Medicine, Surgery,<br />
OBGY, Pediatrics &<br />
Anesthesia) on<br />
regular or contractual<br />
basis<br />
Blood Bank<br />
Functional<br />
At least 50 deliveries<br />
per month. Cesarean<br />
Section and neonatal
Sub Center PHC Hospitals excluding<br />
DH<br />
IPD (excluding<br />
delivery) minimum<br />
30/month<br />
OPD – minimum<br />
1000/month<br />
24<br />
DH<br />
care facility available care facility available<br />
IPD (excluding<br />
delivery) minimum<br />
60/month<br />
OPD – minimum<br />
3000/month<br />
IPD (excluding<br />
delivery) minimum<br />
100/month<br />
OPD – minimum<br />
5000/month<br />
Once facilities are designated for upgradation, actual upgradaton is carried out in following<br />
steps<br />
Sir Step Activity<br />
1 Step -1 Identification of <strong>health</strong> facilities. Health facility is identified<br />
considering the criteria mentioned in table above. Delivery point<br />
criteria is applied since 2011-12.<br />
(Completed)<br />
Step -2 Improvement in basic amenities required to patients – drinking<br />
water, toilets, mattresses, linen, patient furniture, sitting<br />
arrangement, signages, etc.<br />
(Completed)<br />
Step -3 Upgrading PHC to 24×7 status (9 criteria to be fulfilled) and<br />
Hospitals to FRU status (10 criteria to be fulfilled). Deficit of<br />
Training, equipment procurement, civil works, medicine, etc are<br />
identified and fulfilled through IPHS funds.<br />
(Completed for 80% facilities<br />
Step -4 Health Facility is upgradated to IPHS standards. Services to be<br />
provided by that facility are enlisted. Gaps in providing these<br />
services are identified and fulfilled through IPHS Funds.<br />
Step -5 There is no provision of inspection of facilities to award IPHS<br />
status in IPHS guidelines of GoI. Maharashtra has decided to<br />
establish committees at district, circle and state level to inspect
Sir Step Activity<br />
the facility and award IPHS status if it fulfills IPHS criteria.<br />
(Proposed in <strong>2012</strong>-<strong>13</strong>)<br />
Step - 6 IPHS designated facilities with good utilization are identified<br />
functioning improved by strengthening 28 procedures related<br />
quality care.<br />
Criteria for selection of <strong>health</strong> facility<br />
Main aim of the IPHS up gradation is to provide quality services. For this, good functioning<br />
<strong>health</strong> facilities and facilities with potential to get improved are being considered for up<br />
gradation. GoI has provided guidelines for number of deliveries to be conducted for inclusion<br />
of PHCs as 24×7 PHC and hospitals as FRUs which are being called as delivery points.<br />
Considering this, criteria applied for selection of <strong>health</strong> facility for up gradation are as follows:<br />
Table : Criteria for selection of <strong>health</strong> facility for IPHS Up gradation<br />
Sir Criteria SC PHC Hospitals (CHC<br />
to Dist<br />
Hospitals)<br />
1 Infrastructure Should be<br />
functioning in<br />
own building.<br />
2 Water supply Adequate or<br />
source should be<br />
available<br />
3 Manpower Two ANM and<br />
one MPW<br />
should be<br />
available<br />
Should be<br />
functioning in<br />
own building<br />
Adequate or<br />
source should be<br />
available<br />
At least one MO<br />
MBBS<br />
Should be<br />
functioning in<br />
own building<br />
Adequate or<br />
source should be<br />
available<br />
At least three<br />
specialists :<br />
Obstratician,<br />
Pediatrician and<br />
Anesthetist<br />
4 OPD >1000/month >3000/month<br />
5 IPD (excluding delivery) >30/month >90/month<br />
6 Deliveries >3/month >10/month >20/month for<br />
25
Number of institutes upgraded<br />
RH/SDH<br />
>50/month for<br />
DH<br />
IPHS has not specified method for declaration of facility as upgraded to IPHS. Therefore in<br />
year 2011-12, achievement of upgradation was decided by self declaration of the facility that<br />
they have achieved IPHS. Latest figures of upgradation are as follows:<br />
Sir<br />
Table - : Status of up gradation of Health Institutions as per IPHS standard<br />
Type of<br />
Institution<br />
Total no.<br />
in state<br />
No. of<br />
<strong>health</strong><br />
facilities<br />
designated<br />
for upgradation<br />
24×7<br />
PHCs/ FRU<br />
upgraded<br />
IPHS<br />
Upgraded<br />
26<br />
Fulfilling<br />
criteria of<br />
delivery<br />
point<br />
1 Sub-Centre 10580 2997 1755 1521<br />
2 PHC 1810 1067 594 242 658<br />
3 RH/SDH/GH 447 224 <strong>13</strong>2 73 188<br />
4 WH 9 9 9 6 9<br />
4 DH 23 23 23 18 23<br />
Total 12874 4319 757 2094 2299<br />
For year <strong>2012</strong>-<strong>13</strong>, we are establishing committees at District, Regional and State level and<br />
developing evaluation formats for each type of facility. Once the facility approaches District<br />
Health Society to inform about achievement of IPHS status, the committee will visit this<br />
facility for certification.<br />
Sir Type of facility Head of<br />
Committee<br />
Table – IPHS Evaluation Committees<br />
Other members Certificate<br />
issuing<br />
authority<br />
1 Sub-Center RCH Officer One THO, MO DTT,<br />
Representative of CEO, One<br />
IMA representative, One senior<br />
reporter, One NGO<br />
representative<br />
2 PHC DHO DTO, MLCD, RCH Officer,<br />
Representative of CEO, One<br />
DHO &CEO ZP<br />
Deputy Director<br />
i/c Circle and
3 Rural Hospital<br />
Sub District<br />
Hospital, WH<br />
of up to 100<br />
beds.<br />
4 DH, GH and<br />
WH more than<br />
100 beds<br />
Deputy Director<br />
of Health<br />
Services<br />
Joint Director<br />
(Hospitals)<br />
Activities included and Gap filling under IPHS<br />
IMA representative, One senior<br />
reporter, One NGO<br />
representative<br />
Asst. Director (Cl), Principal<br />
HFWTC, Representative of<br />
District Collector, One IMA<br />
representative, One senior<br />
reporter, One NGO<br />
representative<br />
Joint Director (FW), Joint<br />
Director (T), One Deputy<br />
Director, One Dy Secretary<br />
from PHD, One IMA<br />
representative, One senior<br />
reporter, One NGO<br />
representative<br />
District Collector<br />
Joint Director<br />
(Hospitals) and<br />
Com<strong>mission</strong>er<br />
(FW)<br />
Director of<br />
Health Services<br />
and ACS PHD<br />
GoI has specified standards for each type of <strong>health</strong> facility. These standards are for services to<br />
be provided and human resources, medicine, equipment, instrument, infrastructure,<br />
diagnostic facilities, medicine storage system and support services required to provide these<br />
services. External Facility Survey of designated <strong>health</strong> facilities was carried out three years<br />
back. Accordingly plans for upgradation of all the desittanted services were prepared.<br />
Accordingly the facilities are being upgraded.<br />
Since last year (2011-12), Maharashtra has developed one Set of Formats to record the gaps<br />
of one year. This set contains eight forms related to human resources, medicines, equipment<br />
(purchase and maintenance), civil works, support services, etc. In each form information of<br />
total need of the hospital is recorded, supply from Government, donations, user fees charges<br />
and any other local resources (e.g. Cess funds) is recorded and substracted and final gap is<br />
identified. This gap is converted into budget and submitted to District and State. Each of the<br />
Plan Format is checked at district and state level and approval is given on facility basis to each<br />
facility separately.<br />
One such format of DH and PHC is submitted in Annexure to get idea of this detailed and<br />
extensive exercise.<br />
Increase in cost of the upgradation.<br />
Budget requested under this scheme is for upgradation of the facility and maintenance of<br />
facility to IPHS standards. Initially cost of construction and equipment procurement is very<br />
high (last year) and afterwards, cost of human resources, medicine, consumables and<br />
27
maintenance of equipment increases. Thus, in first phase, budget requirement is for<br />
upgrading the facility and in second phase it is for maintaining the IPHS. In Maharashtra we<br />
have observed improvement in OPD, IPD and delivery services by 56% above the non-IPHS<br />
facilities. This increases the cost of second phase hospitals.<br />
Budget requirement of upgradation was calculated on average basis till 2010-11. In 2011-12,<br />
individual planning formats were introduced and budget requirement was calculated based<br />
on gaps. It could not be completed till the time of sub<strong>mission</strong> of PIP so in PIP, the calculations<br />
were partially based on plans and partially on averages. However, for planning of <strong>2012</strong>-<strong>13</strong>,<br />
IPHS planning workshops were conducted in each districts with the help of IPHS Coordinators<br />
and submitted in PIP. Thus, this year planning is individual center based except for Sub-<br />
Center, where plans are still on average basis. Facility wise gaps identified and budget<br />
requirement is submitted for information. As these plans were prepared in February,<br />
additional grants received after plans were prepared (Rs. 51.30 Crores + Rs. 53.8 Crores =<br />
105.1 Crores). Some of the budget although mentioned in Plan is not completely utilized in<br />
planned year as it takes some time to get specialist and equipment required for services.<br />
List of facilities selected for upgradation<br />
List of facilities designated for Upgradation in <strong>2012</strong>-<strong>13</strong> is submitted in Annexure.<br />
Utilization of IPHS facilities<br />
Additional resources are made available to selected <strong>health</strong> facilities to upgrade infrastructure<br />
and manpower to IPHS. After going through the data of last three years it is observed that<br />
utilization of <strong>health</strong> facilities have increased remarkably. Although this increase is slow for<br />
deliveries, improvement in IPD cases indicate this will also catch up by next year.<br />
Utilization of services of IPHS PHCs as compared to non-IPHS PHCs is as follows:<br />
Table – Utilization of IPHS PHCs over non-IPHS PHCs<br />
Sir Indicator IPHS PHC<br />
Non IPHS<br />
PHC<br />
Difference<br />
28<br />
%<br />
Increase<br />
1 OPD/month/PHC 975 731 244 33%<br />
2 IPD/month/PHC 81 48 33 68%<br />
3 Deliveries/month/PHC 9 4 5 125%<br />
Table above indicate that utilization of IPHS PHCs over non-IPHS PHCs is very high. Even in<br />
IPHS PHCs the utilization has increased by 34%, for deliveries, 57 for new OPD and 47% for<br />
IPD. Although number of deliveries per PHC is lower than expected, efforts will be made in<br />
<strong>2012</strong>-<strong>13</strong> to increase the average deliveries in IPHS PHCs to increase to 25 deliveries/month. It<br />
seems to be quite possible after introduction of JSSK in the State.<br />
Similarly for hospitals also there is increase in utilization of services as mentioned in table<br />
below:
Table – Utilization of IPHS CHCs over non-IPHS CHCs<br />
Sir Indicator IPHS RH<br />
Non-IPHS<br />
RH<br />
Difference % increase<br />
1 BOR 59.4 14.1 45.3 23.7<br />
2 New OPD 2638 1516 1122 57.5<br />
3 New IPD 290 <strong>13</strong>8 152 47.6<br />
5 Deliveries 26 9 17 34.6<br />
6 LSCS 2 1 1 50.0<br />
In hospitals, all the indicators have shown remarkable increase in IPHS hospitals. This will<br />
further strengthen during <strong>2012</strong>-<strong>13</strong>.<br />
Plan for year <strong>2012</strong>-<strong>13</strong><br />
Following actions will be taken for up gradation of <strong>health</strong> facilities during <strong>2012</strong>-<strong>13</strong>:<br />
• Systematic plans are prepared based on external facility survey to upgrade the <strong>health</strong><br />
facilities to IPHS. Facilities having less than desired level of deliveries have been<br />
examined on case by case basis. In the places where there deliveries are not as per<br />
desired and where there is no possibility of further improvement, such facilities have<br />
been discontinued for up-gradation for year <strong>2012</strong>-<strong>13</strong>. There are few non-IPHS facilities<br />
where the deliveries have substantially increased. These facilities have been included<br />
in the plan.<br />
• JSSK have been introduced in the State with very good response from community. It<br />
has been observed that this is increasing the overall demand for services in the<br />
PHC/Hospitals. Thus, for better implementation of JSSK, the PHC/Hospital need to<br />
have well equipped laboratory, good quality labour room and Operation Theater and<br />
medicines required for mother as well as other patients also. Medicines included in<br />
JSSK will be procured through JSSK. But other medicines and requirements of hospital<br />
strengthening will be taken from IPHS up-gradation funds to avoid duplication.<br />
• During the visit of Joint Secretary (GoI) to Maharashtra, some of the issues were<br />
discussed with Com<strong>mission</strong>er (FW) and MD. These are : Establishing Dialysis Units in<br />
district Hospitals, Upgrading Burn Wards in District Hospitals and improvement in OPD<br />
services. Provision for these activities is also made in IPHS Up gradation Plans of<br />
Hospitals.<br />
• MCTS has enabled us to track every mother and child. We have introduced recording<br />
of Expected Place of Delivery for these mothers. Now district officials can tell us in<br />
advance how many deliveries will take place at home, in SC, in PHC or hospitals on<br />
particular day based on this data. With the help of this data Scheme called ‘Book your<br />
Bed (BYB)’ have been introduced in all the <strong>health</strong> facilities designated for upgradation<br />
to IPHS standards. In this scheme, all the mothers in areas will be shown the<br />
<strong>health</strong> facility. Bed will be booked in name of mother in advance willing for delivery in<br />
hospital and will be displayed at the entrance of female ward.<br />
29
• First step towards IPHS up gradation for hospitals is compliance of FRU status.<br />
Therefore, hospitals where three basic specialties OBGY, Pediatrics and Anesthesia are<br />
available and hospital is functioning in own buildings are only being included for IPHS<br />
up gradation. Efforts will be made to increase the availability of other specialists and<br />
nurses to provide maximum possible specialty services mentioned in IPHS as per bed<br />
strength.<br />
• Similarly, all the SDH and District Hospitals in state will be included for IPHS up<br />
gradation. Five specialties are being provided to all the hospitals – Medicine, Surgery,<br />
Gynecology, Pediatrics and Anesthesia will be provided on priority considering the<br />
goal of NRHM. In addition to this, maximum efforts will be made to get available<br />
additional 9 specialties as per bed strength of District Hospitals.<br />
• One government RH is run by NGO under PPP mode catering around 1.2 Lakh<br />
populations at Sastur Dist. Osmanabad. As this hospital has started specialty services<br />
and undergoing delivery, cesarean section operation, this hospital will also be<br />
included for IPHS up-gradation.<br />
• There are three areas in the state which are most backward and do not have facilities<br />
nearby. These areas have very high (3 times the state average) MMR and almost<br />
double IMR. Considering this, it has been decided by state to provide special package<br />
to specialists and nurses in these areas. Also these areas will require good residential<br />
accommodation. Considering this, special package for upgradation of these hospitals<br />
is being implemented from October 2011. Details of these areas is as follows:<br />
Sir District Names of RH/SDH Total<br />
No.<br />
1 Gadchiroli SDH Aheri, RH Sironcha, RH<br />
Bhamragad, RH Dhanora, RH<br />
Etapalli<br />
2 Amravati<br />
(Melghat area<br />
only)<br />
SDH Dharani, RH<br />
Chikhaldara, RH Churni<br />
3 Nandurbar RH Akkalkuwa, RH<br />
Dhadgaon, RH Molgi<br />
Remarks<br />
5 Very remote and LEA<br />
affected areas. Except<br />
Dhanora, all other more<br />
than 100 KM away from<br />
DH. No specialist facility<br />
available since<br />
establishment.<br />
3 Very remote reserve<br />
forest area. Very high<br />
IMR and MMR. No<br />
speciality services<br />
available.<br />
3 Very remote area within<br />
Satpuda mountain<br />
range and Narmada<br />
30
iver. No specialities<br />
available since<br />
establishment. High IMR<br />
and MMR.<br />
• Facility survey of hospitals included in up gradation will be carried out by External<br />
Expert agency.<br />
Budget requirement<br />
Considering above factors and based on the IPHS guidelines, one Planning Format was<br />
prepared by SHS and distributed to all the districts. Plans received from the districts are<br />
analysed and only the <strong>health</strong> facilities fulfilling Delivery Point criteria or with potential of<br />
improvement in delivery services have been included in the upgradation list. We have ready<br />
plans for each of the facility in the state. SC plans are kept at the level of District Society and<br />
all the plans for PHC and higher <strong>health</strong> facilities are scruitinised by Quality Assurance wing of<br />
the SHS. Although we have detailed plans of each facility, the budget required is mentioned<br />
as average of these facilities. List of facilities is also attached in annex.<br />
i) Budget for upgradation of facilities except special focus hospitals<br />
Budget required for up gradation is as follows:<br />
Table -: Budget required for up-gradation of <strong>health</strong> institutions as per external facility<br />
survey<br />
Rs. In Lakhs<br />
Sir Type of facility<br />
No. of<br />
facilities<br />
fulfiling<br />
criteria of<br />
delivery point<br />
No. of faciities<br />
included for<br />
IPHS<br />
Upgradation<br />
Average<br />
Budget<br />
required<br />
per unit<br />
31<br />
Total budget<br />
required<br />
1 SC 1521 1521 0.25 380.25<br />
2 PHC 658 658 6 3948<br />
3 RH 110 110 20.15 2216.5<br />
4 SDH – 50 51 51 24.3 1239.3<br />
5 SDH – 100 23 23 41.7 959.1<br />
6 GH – 200 4 4 72.5 290<br />
7 WH - (300 +) 2 2 72.6 145.2<br />
8 WH - (200-299) 2 2 54.9 109.8<br />
9 WH - (
ii) Budget required for special focus Hospitals<br />
Total 11 hospitals have been included as special focus hospitals in the state. These are very<br />
remote hospitals, without availability of specialists, far away from District Hospitals and with<br />
very high IMR and MMR. As per plan, Budget required for upgrading hospitals except human<br />
resources is as follows. Human resources budget is requested in RCH Component under<br />
Infrastructure and Human Resources.<br />
List of special focus hospitals submitted in annexure<br />
Table : Budget required to extremely difficult Hospitals for up gradation<br />
Rs. In Lakhs<br />
Sr Activity<br />
1<br />
2<br />
3<br />
No. of<br />
facilities<br />
Average<br />
Budget<br />
required per<br />
unit<br />
32<br />
Total budget<br />
required<br />
Provision of Laboratory and Blood<br />
Bank Equipment<br />
Repairs and new construction of<br />
6 9.5 57<br />
Operation theatre, Labour room and<br />
Blood Storage Unit<br />
11 16.5 181.5<br />
Repairs and New Construction of<br />
Quarters<br />
11 88 968<br />
Total 1206.5<br />
iii) Establishment of SNCU<br />
This part of SNCU added in IPHS as per remarks on RCH Flexipool.<br />
IMR of Maharashtra as per SRS is 28/1000 live births. About 70% part of this IMR is<br />
contributed by early neonatal deaths. Therefore unless neonatal care is improved, the IMR<br />
will not go down effectively. Considering this, special emphasis is being given to establish<br />
SNCU. NBSU and NBCC. GoI has published IPHS standards for these units and provided<br />
financial guidelines. Based on these guidelines, total 34 SNCUs are being established in the<br />
State as per GOI Norms. In the 34 units a detailed facility assessment with respect to Human<br />
resources, equipment & operationlization was carried out, using GOI facility assessment<br />
checklist.<br />
The restructuring of the 33 units is under process, except for Daga Womens Hospital, Nagpur<br />
which is complete, and the remaining units will be completed by December <strong>2012</strong>. Other units<br />
are being redeveloped as per IPHS and budget is handed over to PWD. It is expected that civil<br />
works of all the 34 SNCU will be complete by December <strong>2012</strong>. However till December <strong>2012</strong><br />
SNCUs are temporarily shifted in other premises and the service to the sick newborns and<br />
LBWs will be continued. The calculation of Human resources for first nine months is as per the<br />
beds currently available which are 250 beds in the State, and for the last two months, once
the SNCUs are as fully operationlized as per GOI norms human resources is calculated for<br />
every 12 beds (1 Pediatrician, 3 Medical Officers, 10 Staff Nurses). Also in the organizational<br />
cost for printing of Neonatal Case record sheets, Ad<strong>mission</strong> registers, Follow-up registers,<br />
Protocols related to Housekeeping, asepsis, Hand washing as well as IEC material for publicity<br />
of SNCUs will be included. As per remarks on RCH division, human resource and related issues<br />
are included in RCH PIP. Component wise inclusion in PIP is submitted below:<br />
Sir Activity Component Remarks<br />
1 Construction of SNCU MFP Budget handed over to PWD. Works<br />
started. Completion of Daga Hospital.<br />
Others will be completed by<br />
December <strong>2012</strong>.<br />
2 Medicine and consumables RCH FP GoI has provided list of medicines for<br />
SNCU. These medicines will be<br />
3 Manpower (Pediatrician<br />
MBBS doctors and Nurses)<br />
4 Larger equipment as per GoI<br />
list<br />
5 Minor equipment as per GoI<br />
list<br />
procured as per need of SNCU.<br />
RCH FP Proposal approved. Appointment<br />
process will start in May <strong>2012</strong>. Actual<br />
appointments as and when required.<br />
MFP Only deficit equipment to be<br />
procured. Specifications finalized.<br />
Process will start once 50% civil work<br />
is complete. Procurement at state<br />
level.<br />
MFP Only deficit equipment to be<br />
procured. Specifications finalized.<br />
Process will start once 50% civil work<br />
is complete. Procurement at District<br />
level.<br />
6 Equipment maintenance MFP It is extremely important to keep the<br />
equipment fully functional and<br />
maintained to avoid accidents.<br />
7 Support services MFP Cleaning and other services round<br />
the clock to maintain cleanliness<br />
which is crucial for prevention of<br />
infections.<br />
8 Contingency MFP Procurement of one computer<br />
system, maintenance of records,<br />
internet, furniture, etc.<br />
Considering the services above, budget required for SNCU under MFP is as follows:<br />
Sir Type of institute<br />
Cost per<br />
unit<br />
No. of units Total cost<br />
1 Larger equipment as per GoI list 11.5 34 391<br />
2<br />
Minor equipment and instrument as per<br />
GoI List<br />
9.2 34 312.8<br />
2 Maintenance of Equipment 3 34 102<br />
33
Sir Type of institute<br />
Cost per<br />
unit<br />
No. of units Total cost<br />
3 Support services 3.6 34 122.4<br />
4 Contingency 1.2 34 40.8<br />
Total 969<br />
List of SNCU is attached in Annexure<br />
Total budget required for IPHS up gradation<br />
Considering the budget requirement of <strong>health</strong> facilities in all the areas of the state and special<br />
inputs required for very remote hospitals, total budget requirement for IPHS Up gradation is<br />
as follows:<br />
Table : Budget required for IPHS Up gradation<br />
34<br />
Rs. In Lakhs<br />
Sr Particulars Budget requested<br />
1<br />
IPHS upgradation of <strong>health</strong> facilities except hospitals in very remote and<br />
difficult areas<br />
10968.15<br />
2 IPHS upgradation of <strong>health</strong> facilities in very remote and difficult areas 1206.5<br />
3 Operational expenses of SNCU in IPHS Hospitals 969<br />
Total <strong>13</strong>143.65
SUBSECTION – B.4.2 : STRENGTHENING OF DISTRICT, SUB-DISTRICT HOSPITALS, CHCs AND<br />
PHCs<br />
SCHEME - B.4.2.1 : UN-INTERRUPTED POWER SUPPLY TO IPHS INSTITUTIONS<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2007-08 605.75 416.28 664.08 660.000<br />
35<br />
Rs. in Lakhs<br />
Remarks<br />
In the remarks about this activity, it was mentioned that this should be part of activity B.4.1.<br />
It is submitted that budget requested under B.4.1 is related to IPHS Upgradation based on<br />
gaps identified in upgradation and also for maintenance of upgradation. As Solar Power<br />
System is not mentioned in IPHS guidelines of GoI, this activity is separately requested.<br />
There is severe electricity problem in state. Presently electricity is available only for a period<br />
of about 12 hours in 24 hours. IPHS <strong>health</strong> institutions require continuous power supply.<br />
Therefore following options are being implemented in state for un- interrupted power supply.<br />
Table :- Various equipment used for un-interrupted power supply in <strong>health</strong> institutions<br />
Sir Type of institute Equipment used for un-interrupted power<br />
supply<br />
1 Sub-Center Inverter<br />
2 PHC Inverter, Solar back up<br />
3 Hospitals up to 50 beds Inverter, Solar Back up<br />
4 Hospitals beyond 50 beds Inverter, Express Feeder<br />
Inverters are procured from Untied funds or RKS funds. Budget for express feeder is provided<br />
through User Fees collection and only deficit budget is paid through IPHS funds.<br />
It has been observed that solar power system is very helpful at PHC level. One Solar<br />
Photovoltaic System has been developed by College of Engineering Pune. Presently we have<br />
provided Solar Photovoltaic System to320PHCs of state. This covers almost all the tribal PHCs<br />
in the state. During year <strong>2012</strong>-<strong>13</strong>, it is proposed to provide solar back up to non-tribal PHCs<br />
with high number of deliveries. Two highest number of deliveries PHCs per district will be<br />
taken up for this scheme. Solar systems which are more than 2 year old also require<br />
maintenance. Budget is also proposed for maintenance of old system.
Monitoring of the solar back up system<br />
All the solar systems are in remote places of State. For the solar photovoltaic system of last<br />
year, one arrangement is made for condition of the system. The system sends one SMS daily<br />
to District HQ and State HQ regarding working condition of the system. If there is any<br />
problem in the working, the SMS informs that. This is reviewed daily by software and system<br />
out of order is checked and maintained. It is proposed to install this system to all the old<br />
systems also. Cost of each system including Sim Card is about Rs. 9000 to 9500/system.<br />
Budget required for solar power backup<br />
Budget required for solar power backup and maintenance is mentioned below:<br />
Table – :Budget required for solar power backup<br />
Sir Type of institute<br />
Cost per<br />
unit<br />
No. of units<br />
Rs. In Lakhs<br />
Total cost<br />
1 Solar Power Backup – PHC 9.2 63 579.6<br />
2<br />
Adding monitoring<br />
systems<br />
system to old<br />
0.092 300 27.6<br />
2 Maintenance of solar back up in PHCs 0.24 220 52.8<br />
Total 660<br />
SCHEME - B.4.2.2 : QUALITY ASSURANCE IN IPHS FACILITIES<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2010-11 1150.24 <strong>13</strong>62.29 1224.70 1234.820<br />
36<br />
Rs. in Lakhs<br />
Remarks<br />
The activity of Quality Assurance was mentioned in PIP guidelines of GoI in 2010-11. That<br />
time this activity was submitted and got approval also. However, activity could not be<br />
implemented as Technical Support Partners could not be appointed. Therefore this was again<br />
requested in PIP of 2011-12 and again got approval. It took long time to clear the preconditions<br />
and NGOs selected so the activity started in October 2011. Now MoU is made with<br />
four Technical Support Partners and NHSRC and this is fourth month they have started work.<br />
This project is for one year only. It will finish by December <strong>2012</strong>. Therefore it is requested to<br />
continue the project for this year.<br />
Substantial numbers of <strong>health</strong> facilities in Maharashtra state are being upgraded as per IPHS.<br />
Maharashtra has started the quality improvement measures for such PHCs and hospitals. As
part of this, all the hospitals will be provided with 28 procedures required for improvement in<br />
functioning of hospitals. These procedures are prepared by experts under supervision of<br />
NHSRC. The <strong>health</strong> facilities after completion of procedures, will get ISO certification.<br />
Technical support of NHSRC is being taken for ISO certification of <strong>health</strong> institutions. As per<br />
guidelines from NHSRC, groups of <strong>health</strong> institutes will be made to facilitate the certification.<br />
The institutes will be supported by technical supervisors for certifications.<br />
The amount mentioned in the table below will be paid to NHSRC/Consultants selected to help<br />
state in getting ISO certification. Consultants have been selected by NHSRC by National<br />
Competitive Bidding. Additional budget will be required for supervision of the activity from<br />
state and regional level. The supervision will be in the form of SHS personnel, POL and<br />
contingent expenses.<br />
Budget required for certification is as per NHSRC guidelines. Total budget required is as<br />
follows:<br />
Table : - Budget required for ISO certification of Health Institutions<br />
Sr. Type of facility<br />
No of<br />
beds<br />
No. of<br />
facility<br />
Annual<br />
Budget<br />
required<br />
per<br />
facility<br />
Budget<br />
required<br />
for year<br />
<strong>2012</strong>-<strong>13</strong><br />
per facility<br />
37<br />
Rs. In Lakhs<br />
Total<br />
budget<br />
required<br />
1 PHC 6 120 2.64 2.24 269.28<br />
2 RH 30 36 4.94 4.20 151.16<br />
3 SDH 50 40 4.94 4.20 167.96<br />
4 SDH 100 20 9.91 8.42 168.47<br />
5 GH 200 3 14.86 12.63 37.89<br />
6 WH 151-300 2 14.86 12.63 25.26<br />
7 WH 335 1 19.86 16.88 16.88<br />
8 WH 60 2 6.46 5.49 10.98<br />
9 DH 151-300 17 14.86 12.63 214.73<br />
10 DH 301-450 5 19.86 16.88 84.41<br />
11 DH 541 1 24.76 21.05 21.05<br />
12 Supervision charges 267 0.25 66.75<br />
12 Total 514 1234.82
SCHEME - B.4.2.3 : BARRIER FREE ENVIRONMENT IN HOSPITALS<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
New 0 0 400 341.080<br />
38<br />
Rs. in Lakhs<br />
Remarks<br />
Hospitals need to have barrier free environment for handicap patients as per the directions of<br />
GoI. There are specialized agencies to convert the hospitals into Barrier Free Hospitals.<br />
Com<strong>mission</strong>er of Handicap has submitted one proposal for conversion of the hospital into<br />
Handicap Friendly Hospital. It is proposed to select 6 districts in the state. The Consultants<br />
approved by Government will be given responsibility of advising about the work to be carried<br />
out. Actual work will be carried out by State PWD as per GoM guidelines.<br />
Hospitals selected for this scheme are : Nashik, Parbhani, Amarawati, and Bhandara.<br />
As per remarks on this subject, estimate of the work is obtained from State PWD. Component<br />
wise budget required will be as follows:<br />
Table – Budget required for conversion of District Hospital into Barrier free hospital<br />
Rs. In Lakhs<br />
Sir Activity<br />
No. of<br />
facilities<br />
Average<br />
Budget<br />
required per<br />
unit<br />
Total<br />
budget<br />
required<br />
1<br />
Renovation work of hospital to suit the<br />
handicap persons<br />
4 20.42 81.68<br />
2 Internal electrification to suit handicap 4 2.25 9<br />
3<br />
Water Supply and sanitation specially for<br />
handicap<br />
4 2.4 9.6<br />
4 Lift with shaft for handicap 4 45 180<br />
5 Sign boards, name plates 4 1.5 6<br />
6 Ramp renovation 4 2 8<br />
7<br />
Contingency, computerization and add to<br />
DSR/Market rates<br />
4 11.7 46.8<br />
Total 341.08
SUBSECTION - B.4.4 : LOGISTICS MANAGEMENT AND IMPROVEMENT<br />
SCHEME - B.4.4.1 : EXTERNAL FACILITY SURVEY<br />
Activity deleted as per the remarks of Deputy Com<strong>mission</strong>er (MH)<br />
SCHEME - B.4.4.2 : MOBILITY SUPPORT<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2008-09 1251.2 542.6 1649.80 1103.550<br />
39<br />
Rs. in Lakhs<br />
Remarks<br />
Mobility support is required to transfer emergency patients, attending epidemics and<br />
transferring serious patients, attending accidents and natural calamity, etc. and also to<br />
transfer routine patients, support to implement the activities related to National Health<br />
Programs and visit to ASHA, ANM and <strong>health</strong> institutions for supportive supervision.<br />
Plan of action <strong>2012</strong>-<strong>13</strong><br />
Approach for mobility support will be as follows:<br />
• Support to existing ambulances in the form of repairs, POL and hiring driver if required<br />
if the state government grants are not sufficient due to higher load in <strong>health</strong><br />
institution. This budget will be provided to RKS of the institution. This will ensure 24<br />
hours availability of ambulance<br />
• Provision of ambulances wherever not available.<br />
• Review of all supervisory vehicles available in state and provision of supervisory<br />
vehicles where ever not available.<br />
Budget requirement <strong>2012</strong>-<strong>13</strong><br />
About 85% PHCs/Rural Hospitals and all District Hospitals have ambulances. However many of<br />
the presently available ambulances are off road as they require repairs. It is proposed to<br />
provide funds for repairs, POL and driver salary whichever is deficit, to these institutions<br />
through RKS with condition that repairs to be carried out only by authorized dealers.<br />
Supervisory vehicles will be provided to BPMU (30) and District level officers who are directly<br />
engaged in support and supervision of NRHM activities in the state such as RCH Officers (33)<br />
and RMO (Outreach) (33). Presently, these officers are provided hired vehicles but in two<br />
years hiring, one new vehicle can be procured. Therefore, procurement of vehicle will be
eneficial. Expenditure on driver and POL for district level supervisory vehicles will be borne<br />
from state funds.<br />
Supervisory work of the officers supervising NRHM works has increased many fold. As each<br />
<strong>health</strong> facility is being monitored from district and state level, lot of information is being<br />
collected and officers are also travelling to <strong>health</strong> facilities to go through the discrepancies.<br />
We have submitted proposal for hiring of vehicles to district officials through RCH. This costs<br />
about Rs. 3.0 Lakh per officer in one year. Currently cheaper supervisory vehicles available on<br />
RC costs about 4.5 Lakh. Thus, this cost will be cleared within one and half year. Considering<br />
life of vehicle for 12 years, this will be really beneficial to the SHS. Cost on driver and POL will<br />
be borne from regular budget of State Government. It will not have any impact on the NRHM<br />
budget. Considering this, it is requested to sanction this proposal along with the supervisory<br />
vehicles.<br />
Budget proposed for providing vehicles to all the <strong>health</strong> institutions is as follows:<br />
Sr Institution<br />
Table – : Budget required for mobility support– <strong>2012</strong>-<strong>13</strong><br />
No. of<br />
functioning<br />
institution<br />
Support for on road<br />
No. of<br />
vehicles<br />
Unit<br />
cost<br />
Budget<br />
required<br />
Requirement for new<br />
purchase<br />
No. of<br />
vehicles<br />
Unit<br />
cost<br />
Budget<br />
required<br />
40<br />
Rs. In Lakhs<br />
Total<br />
budget<br />
required<br />
1 PHC 1809 1809 0.25 452.25 30 4.9 147 599.25<br />
2 RH/SDH<br />
DH and other<br />
453 453 0.3 <strong>13</strong>5.9 21 6.9 144.9 280.8<br />
3 District<br />
hospitals<br />
Level 35 118 0.5 59 0 0 0 59<br />
4 Supervisory<br />
vehicles<br />
440 0 0 0 35 4.7 164.5 164.5<br />
Total 2737 2380 647.15 86 456.4 1103.55<br />
SCHEME - B.4.4.3 : EQUIPMENT MAINTENANCE AND REPAIRS<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2009-10 150.5 224.9 568.8 568.800<br />
Rs. in Lakhs<br />
Remarks
Health equipment is essential part of hospital. They need to be purchased and maintained<br />
properly for quality services. IPHS requires that every equipment should be repaired<br />
immediately and within 30 days. State Government has separate Health Equipment Repairs<br />
Units at all the 8 circle level and one at state level. Support to these units will help in repairs<br />
of <strong>health</strong> equipment in the state.<br />
It is difficult to repair the <strong>health</strong> equipment in difficult areas of the state as no technician is<br />
available. Experience of last year indicates that HEMR unit and private repair agencies cannot<br />
reach these difficult areas. Therefore it is opposed that separate agency will be established in<br />
High Focus districts and Melghat area of the state for repairs of equipment.<br />
Explanation for remarks on this activity is as follows:<br />
1. State Government has already established the Health Equipment Maintenance Unit at<br />
8 places. We are strengthening these units by providing mobility support, deficit<br />
manpower, additional spare parts and operational expenses.<br />
2. All the newly procured equipment are covered under AMC for one to five years<br />
depending upon contract at the time of purchase. Such equipment are repaired by<br />
company. This unit repairs all the equipment not on RC. It also helps the head of<br />
hospital to get the contract people at hospital in time.<br />
3. This unit do not handle sophisticated equipment like Sonography machine, Auto<br />
Analyser, High end ELISA machines, CT SCAN, etc. Such machines are maintained from<br />
regular funds by AMC with authorised service agency. Budget of IPHS is used in IPHS<br />
facilities only in case of gaps.<br />
4. We have serious problem of getting equipment repaired in high focus districts. This<br />
problem has become acute because we are providing lot of additional resources to<br />
these institutions for strengthening in which equipment are also supplied. Incidentally<br />
all these areas are heavy rainfall areas and due to this also equipment go out of order<br />
frequently. Many of the times the technicians from manufacturers do not come in<br />
time for repairs in these areas. Considering this, one pilot project was carried out with<br />
the help of one Mumbai based NGO to train technicians, wardboys, nurses in handling<br />
and maintaining equipment in Nandurbar district. This project was successful but after<br />
some time it was realised that it is difficult to maintain the system with the help of<br />
non-technical persons like this. Therefore it was decided to hire one agency for such<br />
purpose. At least 3 agencies two from Mumbai and one from Nagpur have shown<br />
willingness to participate in this project.<br />
Considering above remarks, it is proposed to approve the activity.<br />
Budget required for repairs of equipment is as follows:<br />
41
Table : - Budget required for Health Equipment Maintenance<br />
Sir Particulars Unit cost No. of units<br />
1<br />
2<br />
Mobility support to HEMR unit - one<br />
vehicle per circle<br />
Hiring engineer /technician (mechanical,<br />
electronic, electrical) as per requirement<br />
and load - five per circle<br />
42<br />
Rs. In Lakhs<br />
Total<br />
budget<br />
required<br />
3 9 27<br />
2.8 44 123.2<br />
3 Initial training of engineers 2.5 4 10<br />
4 Spare parts - Rs. 3 Lakh/district 3 33 99<br />
5 Civil Works as per need 1 8 8<br />
Hiring of agency for <strong>health</strong> equipment<br />
maintenance in high focus districts<br />
73 4 292<br />
6 Contingency including office maintenance 1.2 8 9.6<br />
Total 568.8<br />
SCHEME - B.4.4.4 : DISABILITY WORKSHOPS AT DISTRICT HOSPITALS<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
New 0 0 150 150.000<br />
Rs. in Lakhs<br />
Remarks<br />
Summary information – Section 42 of “The Persons With Disabilities (Equal Opportunities,<br />
Protection Of Rights And Full Participation) Act,1995’’ mentions regarding provision of Aids<br />
and appliances to persons with disabilities and the appropriate Governments shall by<br />
notification make schemes to provide aids and appliances to persons with disabilities.<br />
Accordingly every District hospital with reference to GR dated 01.03.12 Disability workshops<br />
have been sanctioned. The staff of occupational therapist, Prosthetic and orthotic technician,<br />
leather worker and helper has been sanctioned.<br />
Activities completed - Presently there is no workshop is operational.
Plan for 12-<strong>13</strong> – Approximately 700 square feet area is essential for installation of disability<br />
workshop. Equipment like Portable jigsaw machine, Drill Machine, Electric Hand drill<br />
Machine, Grinder can be procured and installed by guidance of All India Institute of physical<br />
Medicine and Rehabilitation. Splints, Calipers, Orthotic (Artificial limbs), Crutches, and Boots<br />
for leprosy patients can be prepared in workshop which will be beneficial to disabled<br />
patients.<br />
Particulars of plan<br />
Sir No Particulars<br />
Unit cost in<br />
lakhs<br />
Number of units<br />
43<br />
Total cost in<br />
lakhs<br />
1 Construction of Disability 30.00 3 90.00<br />
workshops at District<br />
Hospitals of approximate<br />
size 700 square feet<br />
2 Installation of furniture 20.00 3 60.00<br />
and equipment<br />
Total amount proposed in PIP 12-<strong>13</strong> 150.00<br />
SCHEME - B.4.4.5 : MODERNIZATION OF HOSPITAL KITCHEN<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
New 0 0 310 310.000<br />
Rs. in Lakhs<br />
Remarks<br />
Summary information – Due to increased load of patients in hospitals due to JSSK, there is<br />
need to provide quality food in limited manpower in hospital. Modern kitchen gazettes are<br />
very essential to handle increased need.<br />
Activities completed - Presently hospital kitchens of District, mental and women hospitals of<br />
more than 200 beds are providing quality food to 60% of admitted hospital patients through<br />
existing cooks.
Plan for 12-<strong>13</strong> – 23 District hospitals, 4 women hospitals of more than 200 beds and 4 mental<br />
hospitals are proposed for procurement of modern kitchen gazettes such as Mixer, Grinder,<br />
Miller Machine, Chapatti puffer, hot case, Tea urns, Bulk cooker, Refrigerators, Atta kneading<br />
machines etc.<br />
Budget requirement<br />
Sir No Particulars Unit<br />
lakhs<br />
cost in<br />
1 Provision of modern<br />
kitchen gazettes to<br />
kitchens of 23 District<br />
hospitals, 4 women<br />
hospitals of more than 200<br />
beds and 4 mental<br />
hospitals<br />
SCHEME - B.4.4.6 : DISTRICT IPHS MONITORING WING<br />
Number of<br />
units<br />
10.00 31 310.00<br />
Total cost in<br />
lakhs<br />
Issue of manpower under NRHM as discussed in State <strong>health</strong> Society EC Meeting under<br />
Chairmanship of ACS (PH & FW). Review of total posts was done and decision have been<br />
taken to retain some staff and remove some staff. Shifted to SPMU/DPMU with explanation<br />
for continuation.<br />
SCHEME - B.4.4.7 : PUBLIC HEALTH ESTATE MANAGEMENT CELL<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned for<br />
year 2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed in<br />
NPCC<br />
2011-12 0 143.19 123.90 120.300<br />
44<br />
Rs. in Lakhs<br />
Remarks<br />
Most of the <strong>health</strong> facilities in Maharashtra are constructed on land either donated by donor<br />
or on government land.<br />
There is need to update the record of land of <strong>health</strong> facilities in the state for following<br />
reasons<br />
• Infrastructure development<br />
• To make availability of land for constructions of the new <strong>health</strong> facility.<br />
• To remove the encroachment on <strong>health</strong> facility.
• To update the records of land of <strong>health</strong> facility.<br />
Many of these lands are not in the name of <strong>health</strong> department. In some facility the<br />
boundaries are not cleared.<br />
Considering the above fact, Public Health Estate Management Cell is established in<br />
state Health society & at regional places in the Deputy Director Health office during 2011-12.<br />
The State Health Society, Maharashtra Mumbai have already established four Public Health<br />
Estate Management Cell in the state & remaining five will be established till March <strong>2012</strong>.<br />
Performance of Public Health Estate management Cell<br />
As mentioned in remarks, performance of PHEC is submitted.<br />
The performance of Public Health Estate Management Cell is as follows:<br />
Sir Name of the<br />
circle<br />
No of<br />
<strong>health</strong><br />
institutes<br />
visited<br />
Record<br />
Updated<br />
Encroach<br />
ment<br />
Removed<br />
Land made<br />
available for<br />
construction<br />
1. Pune 194 451 0 0<br />
2. Aurangabad 206/65LL 87/61L 2<br />
3. Nagpur 275 122 0 0<br />
4. Latur 311 168 0 01<br />
The budget required for the continuation the project during <strong>2012</strong>-<strong>13</strong> is as follows:<br />
Table : Budget required for Estate Management Cell during <strong>2012</strong>-<strong>13</strong><br />
(Rs. In Lakhs)<br />
Sr. No. Designation No. of<br />
persons<br />
in each<br />
unit<br />
1 Senior Estate<br />
Manager<br />
2 Junior Estate<br />
Manager<br />
No. Of<br />
Unit<br />
Budget per<br />
unit<br />
Budget<br />
required<br />
45<br />
7<br />
Remarks<br />
1 8 3.60 28.8 One each at<br />
circle level.<br />
1 9 2.40 21.60 One at state<br />
level & eight<br />
at circle level
Sr. No. Designation No. of<br />
persons<br />
in each<br />
unit<br />
3 Program Officer<br />
at state level<br />
4 Program<br />
Assistant<br />
5 Travel &<br />
Mobility<br />
6 Office<br />
Contingency<br />
7 Office<br />
equipment&<br />
Furniture<br />
No. Of<br />
Unit<br />
Budget per<br />
unit<br />
Budget<br />
required<br />
46<br />
Remarks<br />
1 1 3.00 3.00 One officer<br />
at State<br />
Health<br />
Society.<br />
1+1 9 1.20 12.00 Two at State<br />
Health<br />
Society &<br />
one each at<br />
regional<br />
office.<br />
9 5.00 45.00<br />
9 0.60 5.40<br />
9 0.50 4.50<br />
Total 16.3 120.3
SECTION - B.5 : NEW CONSTRUCTION, RENOVATION AND SETTING UP OF HEALTH FACILITIES<br />
New construction, repairs of <strong>health</strong> facility infrastructure in Maharashtra is carried out by two<br />
agencies. Infrastructure Development Wing is established to carry out construction work of<br />
buildings of PHC/PHU and Sub-Centers. Contractual Junior Engineer, Deputy Engineer and<br />
Executive Engineers are appointed in this wing. This wing is headed by Superintending<br />
Engineer who is regular SE from PWD. In addition to this, Executive Engineers of PWD also<br />
supervise the work of IDW engineers wherever necessary.<br />
No additional charges are levied on the works done by IDW wing.<br />
New construction of Hospitals, Nursing Schools and Regional Warehouses is carried out by<br />
Public Works Department of Government of Maharashtra. PWD claims 5% Centage charges<br />
for all works done and it is included in estimate provided by PWD.<br />
Both the wings – IDW and PWD use DSR for making estimates.<br />
For specified works such as construction of SNCU or construction of Audiometry Room, PWD<br />
hires special architect for planning. Architect is selected from approved panel of PWD and<br />
payment to architect is made as per approved government rates. Fees of architect are<br />
included in estimate provided by PWD.<br />
Considering the volume of work being done in Health Department and time bound program<br />
of NRHM funds, PWD has appointed Chief Engineer Aurangabad as Nodal Officer for Health<br />
Department works. Positive difference with PWD is observed after appointment of Nodal<br />
officer.<br />
One new software ‘Construction Tracker’ is introduced in Maharashtra state for all <strong>health</strong><br />
department constructions. The work is registered in the system immediately after awarding<br />
administrative approval. Work is tracked till possession. It is proving very usefull to the state<br />
for timely completionof construction.<br />
SUBSECTION - B.5.1 TO B.5.3 : NEW CONSTRUCTION AND RENOVATION OF SUB-CENTERS,<br />
PHCs AND CHCs<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2005-06 4267 7095 <strong>13</strong><strong>13</strong>1.34 8866.050<br />
47<br />
Rs. in Lakhs<br />
Remarks
Health Care Infrastructure<br />
Maharashtra has established large number of <strong>health</strong> Institutions throughout the state.<br />
Construction, repairs and routine maintenance of these institutions are carried out from plan<br />
and non-plan grants of the state. Public Health Department usually does not get sufficient<br />
funds for these purposes. As a result, <strong>health</strong> infrastructure was in poor condition in most of<br />
the districts. However, after getting additional support under NRHM, now most of the <strong>health</strong><br />
institutions are repaired, having water supply and drainage facilities and electrification.<br />
Health Institutes require funds for maintenance and repairs of existing buildings,<br />
construction of additional facilities in old buildings and construction of new buildings where<br />
they are not available.<br />
A birds eye view of the infrastructure available in state and short fall is shown<br />
below.<br />
District Requirement of Infrastructure DH CHC PHC SHC<br />
Required as per population norms 30 417 2051 12637<br />
Existing Facilities 27 367 1816 10578<br />
Under Construction 2 19 144 788<br />
Shortfall 1 31 41 1271<br />
1. Progress during 2011-12<br />
Following actions have been taken to speed up the repairs and construction activities.<br />
• Infrastructure Development Wing (IDW) is established in all the districts of the State.<br />
• IDW is headed by one Superintending Engineer from Public Works Department of<br />
Government of Maharashtra on deputation. Eight posts of contractual Executive<br />
Engineers are sanctioned in the state to supervise the district civil works progress.<br />
• At district level, IDW is headed by one contractual Deputy Engineer. He is supported<br />
by 3–4 Junior Engineers. (One Junior Engineers appointed for every four blocks.)<br />
Accordingly 33 posts of Deputy Engineers are sanctioned out of which 30 are in place<br />
and 93 post of Junior Engineers are sanctioned out of which 87 posts are filled in.<br />
• Powers of administrative approval and technical sanctions are decentralized and<br />
delegated to District Societies. Accordingly, District Health Officer/Civil Surgeons have<br />
powers to sanction new construction work up to 15 Lakhs and Chief Executive Officers<br />
of Zilla Parishads have full powers for administrative sanctions of works to be under<br />
taken in their district.<br />
• Instructions are issued to all the districts to construct new buildings as per state plans<br />
of hospitals and quarters.<br />
• Public Works Department of Maharashtra State uses DSR for preparing and<br />
sanctioning work estimates. Districts are permitted to use the same rates for NRHM<br />
works.<br />
Information about new construction works sanctioned under NRHM<br />
48
Health<br />
Facility<br />
New Construction sanctioned under<br />
NRHM so far in High Focus Districts<br />
(i.e. Nandurbar / Gondia /<br />
Gadchiroli)<br />
2007<br />
-08<br />
2008<br />
-09<br />
2009<br />
-10<br />
2010<br />
-11<br />
2011<br />
-12<br />
New Construction sanctioned under<br />
NRHM so far in<br />
Non-High Focus Districts<br />
2007<br />
-08<br />
2008<br />
-09<br />
2009<br />
-10<br />
2010<br />
-11<br />
49<br />
2011<br />
-12<br />
DH<br />
SDH<br />
and<br />
0 1 0 0 0 0 1 2 1 1 6<br />
other<br />
hospital<br />
s above<br />
CHC<br />
0 0 0 0 0 0 1 0 1 0 2<br />
CHCs 0 2 0 0 0 0 7 3 0 0 12<br />
PHCs<br />
Other<br />
Health<br />
facilities<br />
above<br />
SC but<br />
0 0 0 0 11 0 <strong>13</strong> 17 8 28 77<br />
below<br />
block<br />
level<br />
(may<br />
include<br />
APHC<br />
etc.)<br />
0 0 0 0 0 0 0 1 10 0 11<br />
Sub- 5 5 7 0 21 38 234 193 103 101 70<br />
Total 5 8 7 0 32 38 256 216 123 <strong>13</strong>0<br />
81<br />
5<br />
Health<br />
Facility<br />
Information about Upgradation works Sanctioned under NRHM<br />
Upgradation sanctioned under<br />
NRHM so far in<br />
High Focus Districts<br />
(i.e. Nandurbar / Gondia /<br />
Gadchiroli)<br />
2007<br />
-08<br />
2008<br />
-09<br />
2009<br />
-10<br />
2010<br />
-11<br />
2011<br />
-12<br />
Tot<br />
al<br />
Upgradation sanctioned under<br />
NRHM so far in<br />
Non-High Focus Districts Total<br />
2007<br />
-08<br />
2008<br />
-09<br />
2009<br />
-10<br />
2010<br />
-11<br />
2011<br />
-12
DH<br />
SDH and<br />
0 2 1 3 0 37 116 56 43 20 278<br />
other<br />
hospitals<br />
above CHC<br />
0 6 4 14 3 23 63 28 10 3 154<br />
CHCs 3 9 1 0 1 38 77 77 30 9 245<br />
PHCs<br />
Other<br />
Health<br />
facilities<br />
above SC<br />
17 59 142 165 8 628 567 839 470 142 3037<br />
but below<br />
block level<br />
(may<br />
include<br />
APHC etc.)<br />
0 4 6 15 0 0 44 0 0 0 69<br />
Sub-Centres 67 126 68 293 2 606 701 676 356 219 3114<br />
Total 87 206 222 490 14 <strong>13</strong>32 1568 1676 909 393 6897<br />
Progress of Works Sanctioned under NRHM<br />
Progress of New Constructions<br />
Completed Under Construction Sanctioned but Yet<br />
Health Facility High<br />
Focus<br />
Districts<br />
Non High<br />
Focus<br />
Districts<br />
High<br />
Focus<br />
Districts<br />
Non<br />
High<br />
Focus<br />
Districts<br />
High<br />
Focus<br />
Districts<br />
Non<br />
High<br />
Focus<br />
Districts<br />
Total<br />
DH<br />
SDH and other<br />
1 5 0 0 0 0 6<br />
hospitals<br />
above CHC<br />
0 0 0 2 0 0 2<br />
CHCs 2 5 0 5 0 0 12<br />
PHCs 0 17 0 29 11 20 77<br />
Other Health<br />
facilities<br />
0 11 0 0 0 0 11<br />
Sub-Centres 15 502 8 142 15 25 707<br />
Total 18 540 8 178 26 45 815<br />
50
2. Plan for the year <strong>2012</strong>-<strong>13</strong><br />
During last four financial years, priority was given to repairs of <strong>health</strong> institutions<br />
because this resulted into making the <strong>health</strong> institutes functional with minimum budget. Now<br />
following policy decisions have been taken regarding execution of Civil Works in the state:<br />
• Henceforth minor repairs will be carried out locally by Rogi Kalyan Samittee from<br />
funds such as AMG, RKS and if necessary the IPHS funds.<br />
• For repairs of institution, either State government or IDW budget will be utilized for<br />
major repairs of <strong>health</strong> institutions.<br />
• New constructions to be focused on blocks that have list infrastructure and are<br />
backward.<br />
• Plans for new construction should be in accordance to the latest developments in<br />
technologies for hospitals constructions.<br />
• All civil works are to be budgeted under <strong>mission</strong> <strong>flexipool</strong> only (including budget for<br />
minor civil works which earlier used to be booked under RCH Flexipool.)<br />
• Priority will be given for construction of Sub-Centers, PHCs and Quarters of critical<br />
staff.<br />
• In one institution, no budget from two sources will be utilized for civil works.<br />
The Information about proposed works to be undertaken in <strong>2012</strong> -<strong>13</strong> and budget<br />
required for that is as below.<br />
District : Maharashtra<br />
Proposed PIP <strong>2012</strong>-20<strong>13</strong><br />
(Rs. In<br />
Sr.<br />
No.<br />
Type<br />
of<br />
Heal<br />
Phys<br />
ical<br />
New Construction<br />
Unit Budg Propos<br />
Cost et ed<br />
Repairs / Upgradation<br />
Phys Budget Propos<br />
ical Requir ed<br />
Total<br />
Physic Budg<br />
al et<br />
1 DH 0 0 0.00 0 11 325.00<br />
9<br />
Month<br />
s<br />
11<br />
325.0<br />
0<br />
2 SDH 0 0<br />
New<br />
0.00 0 15 204.00<br />
9<br />
Month<br />
s<br />
15<br />
204.0<br />
0<br />
3 CHC 1<br />
Constru<br />
ction 1<br />
CHC @<br />
96 L<br />
New<br />
96.00<br />
12<br />
Months<br />
57 658.25<br />
9<br />
Month<br />
s<br />
58<br />
754.2<br />
5<br />
4 PHC 53<br />
Constru<br />
ction<br />
22<br />
PHCs @<br />
2339.<br />
00<br />
12<br />
Months<br />
304<br />
1997.6<br />
6<br />
6<br />
Month<br />
s<br />
357<br />
4336.<br />
66<br />
51
5 SHC 109<br />
Total 163<br />
annexed.<br />
72 L<br />
(31<br />
Qtrs. )<br />
New<br />
Constru<br />
ction<br />
109 SCs<br />
@ 18 L<br />
1962.<br />
00<br />
4235.<br />
00<br />
9<br />
Months<br />
475<br />
862<br />
1284.1<br />
4<br />
4469.0<br />
5<br />
6<br />
Month<br />
s<br />
52<br />
584<br />
1025<br />
3246.<br />
14<br />
8866.<br />
05<br />
The list of the facilities that are proposed for new construction and upgradation is<br />
SUB-SECTION - B.5.4 : SETTING UP OF INFRASTRUCTURE DEVELOPMENT WING<br />
As per remarks, shifted to Program Management Section<br />
SUBSECTION - B.5.5 : GOVERNMENT DISPENSARIES AND OTHER RENOVATIONS<br />
SUBSECTION - B.5.6 : CONSTRUCTION OF BLOCK HEALTH OFFICE, FACILITY IMPROVEMENT,<br />
CIVIL WORKS OF BEmOC AND CEmOC CENTERS<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2009-10 245 190 1286 711.500<br />
Rs. in Lakhs<br />
Remarks<br />
Mission Flexi pool has sanctioned activity for construction of BPMU. It is proposed to<br />
construct the BPMU in all the blocks phase wise. There are 56 BPMU situated in government<br />
buildings. Repairs of these BPMU will be carried out. THO will also be provided with quarters<br />
in phased manner. As strengthening of the BPMU is very important for monitoring of NRHM<br />
activities, it is proposed strengthen this activity.The BPMU will have office, one meeting<br />
hall,furniture and quarters for THO in tribal areas.<br />
In the districts where there is no Medical College, DPMU also need to be strengthened. This<br />
will be carried out from same funds.
In remarks, it has been mentioned to submit details where the BPMU is to be established. In<br />
this regard it is submitted that, BPMU is already established in 353 places in the state. From<br />
regular side, one Taluka Health Officer (THO), one Jr. Clerk, one Health Assistant and one<br />
MPW are appointed in BPMU. One Accountant and one DEO are sanctioned under NRHM.<br />
They are appointed at all the blocks in the state.<br />
Budget requirement<br />
Budget required for this activity is as follows:<br />
Table – Budget requirement for BPMU/DPMU<br />
Sir Particulars Unit cost<br />
1<br />
2<br />
3<br />
No. of<br />
block<br />
53<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
Repairs of BPMU/DPMU quarters, etc.<br />
functioning in Govt. Buildings<br />
3.5 33 115.5<br />
New Construction of BPMU/DPMU, HQ<br />
quarters in non-tribal areas<br />
40 5 200<br />
New Construction of BPMU/DPMU,<br />
quarters in tribal and LEA areas<br />
44 9 396<br />
Total 711.5<br />
SUBSECTION - B.5.7 : MAJOR CIVIL WORKS FOR OPERATIONALIZATION OF FRU<br />
Until last Year (i.e. 2011-12) this programme was a part of RCH Programme. But as per the<br />
current Guidelines of GOI, all civil construction works are to be incorporated in Mission<br />
Flexipool. Hence this programme is incorporated under Mission Flexipool. The details are as<br />
below.<br />
FMR<br />
Code<br />
B.5.7<br />
Activity Unit Rate<br />
Minor Civil works for<br />
operationalisation of<br />
FRUs<br />
Rs. 5 Lakhs/<br />
FRU<br />
No of<br />
Institutes<br />
The list of works is annexed Separately.<br />
Total<br />
Amount<br />
Required<br />
Demand<br />
FRUs - 45 225.00 225.00
SUB-SECTION - B.5.8 : MAJOR CIVIL WORKS FOR OPERATIONALIZATION OF 24×7 PHCs<br />
B.5.8<br />
Minor Civil works for operationalisation of 24 X 7 PHCs<br />
Until last Year (i.e. 2011-12) this programme was a part of RCH Programme. But as<br />
per the current Guidelines of GOI, all civil construction works are to be incorporated in<br />
Mission Flexipool. Hence this programme is incorporated under Mission Flexipool. The details<br />
are as below.<br />
FMR<br />
Code<br />
B.5.8<br />
Activity Unit Rate<br />
Minor Civil works for<br />
operationalisation of 24<br />
X 7 PHCs<br />
Rs. 3 Lakhs/<br />
PHC<br />
No of<br />
Institutes<br />
The list of works is annexed Separately.<br />
Total<br />
Amount<br />
Required<br />
54<br />
Demand<br />
PHCs - 201 603.00 603.00<br />
SUBSECTION - B.5.9 : CIVIL WORKS TO OPERATIONALIZE INFECTION MANAGEMENT AND<br />
ENVIRONMENT PROTECTION PLAN<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2011-12 0 123.55 104.7 225.000<br />
Rs. in Lakhs<br />
Remarks<br />
As per the Environment Protection Act, every hospital is required to have the infection<br />
management and environment protection plan. Following actions are taken in Maharashtra<br />
state:<br />
All the hospitals are handing over the hospital waste to agency appointed by Government at<br />
GoM fixed rates.<br />
All the PHCs and SCs dispose of medical waste in deep burial pits as per the design approved<br />
by the act.<br />
All the doctors and nurses need to be trained in infection management and environment<br />
protection. Training of all the <strong>health</strong> facilities in block will be carried out at block level in one<br />
of the RH/SDH/DH<br />
Budget required for this activity is as follows:
Table : Budget required for Construction in Infection Management and Environment<br />
Protection Plan<br />
Rs. In Lakhs<br />
Sir Particulars<br />
1<br />
2<br />
Budget per<br />
unit<br />
No. of units<br />
55<br />
Total<br />
budget<br />
required<br />
Biomedical waste Pits at<br />
PHCs/Hospitals without central<br />
agency<br />
0.7 66 46.2<br />
Biomedical waste pits at SC<br />
conducting delivery<br />
0.3 195 58.5<br />
Total 104.7<br />
SUBSECTION - B.5.10 : STRENGTHENING OF TRAINING INFRASTRUCTURE (Training institutes<br />
and nursing Schools)<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2006-07 1548.30 1481.6 2459 1696.500<br />
Rs. in Lakhs<br />
Remarks<br />
Training is essential part of implementation of any program. Trained manpower is essential to<br />
provide quality services. Considering the importance of training in implementation of NRHM<br />
activities and in achieving the NRHM goal, utmost importance is given to training in the state.<br />
Training infrastructure in state<br />
Maharashtra has strong training infrastructure. Maharashtra has currently one Public Health<br />
Institute at Nagpur, 6 HFWTCs at divisional HQ, 33 District Training Centers, 23 Hospital<br />
Training Centers and 38 Block Training Centers. Considering the <strong>health</strong> circles and districts,<br />
one more HFWTC is established in Konkan Region under financial support of NRHM.<br />
Areas covered for strengthening<br />
Following areas are being covered for strengthening of infrastructure<br />
• Majority of training centers do not have basic training equipment. Additional required<br />
equipment will be provided to training institutes.<br />
• Vehicles require to training centers for field visits. Vehicles will be hired by the<br />
institute as and when required.
• Civil Works or extension of training and staying capacity of the institute as per need of<br />
institute<br />
• Support in up keeping of training institute premises particularly the hostel.<br />
Training institutes covered for strengthening<br />
Following training institutes are covered for strengthening<br />
• District Training Centers (33)<br />
• Hospital Training Centers (23)<br />
• Health and Family Welfare Training Centers (7)<br />
• Public Health Institute Nagpur (1)<br />
• Nursing Schools (31)<br />
Compliance of remarks<br />
Compliance about remarks are as follows:<br />
1. Approval for civil works and construction of Training Institutes is Rs. 1039.63 Lakh (Not Rs.<br />
1481.6 Lakh). Expenditure for this activity is Rs. 1007.592 (97%) for the year 2011-12.<br />
2. This budget is utilized mainly for maintenance / repairs of main building and hostel Extension.<br />
One HFWTC is constructed (Thane), one new hostel is constructed at Nagpur and extension of<br />
hostel is carried out at Nashik, Aurangabad and Amravati.<br />
3. From the budget of year 2011-12, Extension of HFWTC Nagpur Hostel, Repairs of Kitchen of<br />
Nagpur HFWTC, Electrification of Hostels, New Hostel at Pune, Construction of DTT Building at<br />
3 places (released Rs. 15 Lakh as first installment) were sanctioned and approved.<br />
4. For year <strong>2012</strong>-<strong>13</strong>, budget for Training Institutions and Nursing Schools is requested in one<br />
activity so budget is increased. This year, remaining amount of new hostel at Pune, Kolhapur<br />
and Thane will be paid, Kitchen of Nashik and Amravati will be repaired. In addition to this,<br />
budget for minor repairs of main and hostel buildings will also be carried out.<br />
Budget is revised for all the centers considering additional budget received under reappropriation.<br />
Final requested budget is as follows:<br />
Budget requirement for strengthening of training institutes<br />
Budget required for these activities is mentioned below:<br />
Table – Budget requirement for strengthening of training institutes<br />
Sir Activity<br />
Average<br />
Unit cost<br />
No. of<br />
units<br />
56<br />
Rs. In Lakhs<br />
Budget<br />
requirement<br />
1 Minor civil works and furniture<br />
i District Training Center 3 33 99<br />
ii Hospital Training Center 2 23 46<br />
iii HFWTCs and PHI 15 8 120
Sir Activity<br />
Average<br />
Unit cost<br />
No. of<br />
units<br />
57<br />
Budget<br />
requirement<br />
iv Nursing Schools 6 31 186<br />
v BTCs 1 8 8<br />
Total 459<br />
2<br />
Construction/extension<br />
institute<br />
of training<br />
i District Training Center 18 3 54<br />
ii Hospital Training Center 85 3 255<br />
iii HFWTCs and PHI 45 8 360<br />
iv Nursing Schools 45 8 360<br />
v BTCs 0 0 0<br />
Total 1029<br />
3<br />
Provision of required training aid and<br />
equipment<br />
i District Training Center 1 33 33<br />
ii Hospital Training Center 0.5 23 11.5<br />
iii HFWTCs and PHI 3 8 24<br />
iv Nursing Schools 4 31 124<br />
v BTCs 0 0 0<br />
Total 192.5<br />
4<br />
Library for training institutes and data<br />
management center<br />
2 8 16<br />
Grand Total 1696.5<br />
Subsection B.5.11: Third Party Evaluation of Civil Works<br />
In NRHM, execution of civil works pertaining to state sector Buildings (i.e. District<br />
Hospitals, Sub District Hospitals and CHCs) is done by State PWD and execution of works<br />
pertaining to Zilla Parishad sector i.e. PHCs and SCs is done by Infrastructure Development<br />
Wing (IDW) established in every district. As far as State PWD is concerned there is a separate<br />
wing called “Vigilance and Quality Control Wing” for monitoring the quality of works being<br />
executed by PWD. But for the works executed by IDW there is no independent quality<br />
assurance wing.<br />
Hence it is decided to get the quality control work (pertaining to IDW works) done by<br />
appointing a separate agency at State level for “Third party evaluation.” The State Executive
Committee also sanctioned the proposal for appointing a separate agency for third party<br />
evaluation in the E.C. meeting held on 22-12-2011.<br />
The scope of the work for “Third Party Evaluation” is decided on the basis of system existing<br />
in “Sarva Shiksha Abhiyan” in Education Department and it is as below :<br />
1. The consultant / representative (Engineer) shall visit each site of work for minimum<br />
four times during the construction of work. These visits shall be when the construction work<br />
is at Excavation level, at plinth level, at beam / slab level and at completion stage for issue of<br />
completion certificate.<br />
2. The consultant, at his own cost, shall check the quality of the materials brought on the<br />
site of work and ensure that the materials are in accordance with the specifications generally<br />
prescribed for the work. The laboratory test results of the materials tested be submitted to<br />
district CEO, ZP.<br />
3. consultant should remain present in the co-ordination / review meeting to be held at<br />
State level or at District level once in a month or earlier as required (at no extra cost.)<br />
4. As per the intimations, the consultant or his authorized Engineer should accompany to<br />
the IDW Engineers when they take site visits / organize meetings at District level.<br />
5. If any deviation in design / construction or compromise in quality is observed during<br />
the site visit of consultant, it should be immediately reported to CEO, ZP at district level and<br />
SE, IDW, Mumbai for further action.<br />
6. Consultant shall organize with his own arrangement and equipments, at his cost, a<br />
one day workshop to impart training to District IDW Engineers at mutually agreed suitable<br />
place at district. The expenses towards the TA & DA of participants except the consultant) will<br />
be borne by NRHM. A suitable place will be made available free of cost to consultant for<br />
arranging such training programme.<br />
7. The consultant shall appoint two Engineers (Minimum Qualification B.E. Civil) for each<br />
district. If the no. of works in any district are more than 500 then an extra Engineer for 250<br />
works should be appointed.<br />
8. Consultant shall submit monthly report about the general progress of the works (for<br />
each work).<br />
9. Consultant should suggest the remedial measures to be carried out if any defects are<br />
noticed, during construction.<br />
10. Consultant should suggest the ways and means for economical construction. (To<br />
reduce the cost of construction without affecting quality of work.)<br />
11. Consultant should suggest methodology “to check and ensure the quality of work<br />
done” (by IDW Engineer) and check the work quality accordingly.<br />
12. Consultant shall not issue any instructions directly if in his opinion it is found<br />
necessary to change specifications or modify design. The same shall be brought to the notice<br />
of regional Executive Engineer and SE, IDW, Mumbai.<br />
<strong>13</strong>. The consultant shall have minimum 3 years experience in the field of civil works of<br />
similar magnitude to that of the works covered in the proposed project.<br />
58
14. Consultant shall have to prepare “Manual for good construction practices” and<br />
“Checklist” covering all the items to be executed as per the estimate and furnish it to IDW,<br />
Engineers.<br />
15. After the work is completed consultant shall issue completion certificate as per format<br />
approved by SE, NRHM, Mumbai.<br />
The procedure for appointing such agency at state level is in progress and it is<br />
expected that the agency will be fixed upto the end of March <strong>2012</strong>. Hence provision for the<br />
above activity is necessary in PIP <strong>2012</strong>-<strong>13</strong>.<br />
Provision is done on lumpsum basis i.e. @ 2.0% of the total budget for civil<br />
construction. The total budget for civil construction (i.e. Mission <strong>flexipool</strong> + Minor civil works<br />
for FRUs and 24 x 7 PHCs) is 88.66 + 2.25 + 6.03 = 96.94 Crores.<br />
Hence budget required for third party evaluation of civil works is :-<br />
2.0 % x 9694 (Lakhs) = 194 Lakhs.<br />
59
SECTION - B.6 : CORPUS GRANT TO HMS/RKS<br />
SUBSECTION - B.6.1 TO B.6.3 : ROGI KALYAN SAMITEE (RKS) OF DH/SDH/CHC/PHC<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2005-06 2446 2449 2457 2458.000<br />
60<br />
Rs. in Lakhs<br />
Remarks<br />
Rugna Kalyan Samitee (RKS) is important step towards communalization of <strong>health</strong> care<br />
delivery. It is established to improve the hospital services, make the services community<br />
oriented and self-sufficiency of community in planning and implementation of their <strong>health</strong><br />
needs. Well functioning RKS supported by VHCs forms excellent responsive <strong>health</strong> service<br />
delivery model.<br />
All the functioning <strong>health</strong> facilities such as PHCs/RHs/DHs have established RKS and<br />
registered.<br />
Budget requirement for year <strong>2012</strong>-<strong>13</strong><br />
Budget requirement for RKS in Maharashtra is given in table below:<br />
Table – : Budget requirement for RKS for year <strong>2012</strong>-<strong>13</strong><br />
No. of<br />
Rs. In Lakhs<br />
Total budget required<br />
Sir Type of facility<br />
functioning<br />
facilities<br />
Unit rate<br />
Budget<br />
required<br />
1 PHC 1810 1.00 1810.00<br />
2 CHC(including<br />
RH/SDH/WH/GH/Malvani Malad)<br />
458 1.00 458.00<br />
4 DH including Leprosy, Mental, TB,<br />
Ortho and Referral Hospitals<br />
38 5.00 190.00<br />
Total 2306 2458.00
Year of starting<br />
the<br />
scheme/initiative<br />
SECTION : B.7 : PREPARATION OF DISTRICT HEALTH ACTION PLANS<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2006-07 277.8 292.8 370.75 370.750<br />
61<br />
Rs. in Lakhs<br />
Remarks<br />
In order to make NRHM fully accountable, the district <strong>health</strong> action plan will be the principal<br />
instrument for planning, implementation and monitoring, formulated through a participatory<br />
and bottom up planning process. District Health Mission constituted as per guideline is<br />
responsible for the planning of district.<br />
GOI in NRHM Activities and Norms has published that up to Rs. 20.0 Lakhs can be utilized per<br />
district for surveys, workshops, studies, consultations, orientation in the process of<br />
preparation of District Health Action Plans.<br />
Budget requirement<br />
Considering the bottom up approach being used by Maharashtra and also the funds utilized<br />
during preparation of PIP of 2011-12, it is proposed to request for the budget as mentioned<br />
below for preparation of PIP of year <strong>2012</strong>-<strong>13</strong>.<br />
Table –: Budget required for preparation of PIP for year <strong>2012</strong>-<strong>13</strong><br />
Sir Particulars Unit cost<br />
No.<br />
units<br />
of<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
1 District Health Action Plan at block level 0.75 353 264.75<br />
2<br />
HFWTC for Preparation and Compilation<br />
workshops<br />
6 8 48<br />
3 Circle offices for supervision 1 8 8<br />
4<br />
State PIP (All components - meeting,<br />
review, printing, etc)<br />
50 1 50<br />
Total 370.75
SECTION - B.8 : PANCHAYATI RAJ INITIATIVE<br />
SUBSECTION - B.8.1& B.8.2 : CONSTITUTION AND ORIENTATION OF COMMUNITY LEADERS<br />
AND VHSC, SHC, PHC, CHC, ETC& : ORIENTATION WORKSHOP, TRAINING AND CAPACITY<br />
BUILDING OF PRI AT STATE, DISTRICT HEALTH SOCIETIES AND PHC LEVEL<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
New 0 <strong>13</strong>7.81 317.70 176.500<br />
62<br />
Rs. in Lakhs<br />
Remarks<br />
In Maharashtra, Village Health Committees have developed in all revenue villages, SC<br />
Committees in all SCs and RKS in all <strong>health</strong> facilities at and above PH level. Orientations<br />
training of members of these committees have been conducted during 2009-10. It is<br />
proposed to carry again the orientation of these members with the help of SHSRC. Budget<br />
required will be for snacks of the members and booklet to be given to each member. Training<br />
of all VHNSC and SC members in PHC along with RKS members will be carried out at PHC level.<br />
There will be around 100 participants for each orientation camp. Responsibility of this<br />
training will be given to Health and Family Welfare TrainingCentres.<br />
Large number of Panchayat Raj leaders are involved in NRHM. In Maharashtra, Panchayat<br />
elections are being conducted in February <strong>2012</strong>. New Members will be elected in all the Zilla<br />
Parishads. These members need to be oriented.<br />
Compliance of remarks is as follows:<br />
1. Trainings were started in July 2011 but discontinued as it was realised that Panchayat<br />
elections were to be held around November. Elections were held and new members<br />
came into existence in February. Training of elected members conducted in March<br />
<strong>2012</strong>.<br />
2. Total trained persons are 35636 RKS members and 39755 VHC members.<br />
3. Considering the trainings conducted, budget is revised and submitted for approval.<br />
4. New members will be trained in July August <strong>2012</strong>.
Budget required for this activity is as follows:<br />
Table –: Budget required for PRI member workshops<br />
Sir Particulars Unit cost<br />
No. of<br />
batches<br />
63<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
1 Preparation of training material 0.1 353 35.3<br />
2 Charges for arrangement and food 0.2 353 70.6<br />
3 Contingency 0.1 353 35.3<br />
4 Supervision charges to HFWTC/block 0.1 353 35.3<br />
Total 176.5<br />
SUBSECTION - B.8.3 : ORIENTATION WORKSHOPS FOR DISTRICT AND STATE HEALTH<br />
SOCIETY MEMBERS<br />
Activity deleted as per remarks<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
SUBSECTION - B.8.4 : GUIDED TOURS FOR MLAs, MLCs AND OFFICE BEARERS OF ZILLA<br />
PARISHADS<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2011-12 0 56.8 102.6 68.400<br />
Rs. in Lakhs<br />
Rs. in Lakhs<br />
Remarks<br />
MLAs, MLCs and MPs are now members of various monitoring committees for NRHM<br />
activities. Many of them are now a days taking keen interest in NRHM activities. During last<br />
year, It was proposed to organise one orientation camp plus guided tours to them in one of<br />
the districts of each circle. Same program is being organised during this year.<br />
As office bearers of Zilla Parishads will change, this program is being expanded then last year.<br />
This scheme will be implemented through Deputy Director i/c circles.<br />
As MLAs were busy in Panchayat Elections, the tour programs were postponed many times.<br />
The plan was to conduct these programs at regional level but MLAs insisted to see facilities of<br />
the district only. Total 6 tour programs were organised and 19 MLAs attended the program.<br />
The program is completely revised this year. Budget provision is also reduced.
Budget required for this activity is as follows:<br />
Table : - Guided tours for MLAs<br />
Sir Particulars Unit cost No. of units<br />
64<br />
Rs. in Lakhs<br />
Budget<br />
required<br />
1 Orientation material per batch 0.3 12 3.6<br />
2 Lodging and boarding charges for MLA/MP 2 12 24<br />
3 Expenditure of travel 2.4 12 28.8<br />
4<br />
Supervision charges and contingency to<br />
Deputy Director i/c circle<br />
1 12 12<br />
Total 68.4
Year of starting<br />
the<br />
scheme/initiative<br />
SECTION - B.9 : MAINSTREAMING OF AYUSH<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2009-10 645.2 <strong>13</strong>94.82 1240.53 <strong>13</strong>58.<strong>13</strong>0<br />
65<br />
Rs. in Lakhs<br />
Remarks<br />
Indian Systems of Medicine & Homoeopathy (ISM&H) have proven strengths of treating<br />
common and chronic diseases. With a view to make available the benefits of Ayurveda,<br />
Unani, Siddha, Yoga & Naturopathy and Homoeopathy to the public at large, so that the<br />
people can exercise their choice in accessing and specialized treatment centers of ISM&H in<br />
the Allopathic hospitals. The objectives is to build bridges across medical systems by providing<br />
general and specialized therapies of Ayurveda, Unani medicine, Siddha, Yoga & Naturopathy<br />
and Homeopathy for utilization as an adjunct or better alternative to conventional medical<br />
treatment. Similarly of Medicine & Homeopathy is a matter of concern as it has put the<br />
credibility of these systems at stake. It has been felt that this situation needs to be addressed<br />
with concerted efforts.<br />
Following actions are taken for AYUSH scheme<br />
• AYUSH facility – Ayurved, Homeopathy, Unani, Yoga and Naturopathy facilities are<br />
started in all District Hospitals by appointing contractual doctors.<br />
• 6 District Hospitals are provided AYUSH Wing (indoor, outdoor Panchakarma and<br />
Ksharsutra facility and of AYUSH). For this AYUSH department grant is being utilized.<br />
• AYUSH OPD and IPD facility started in 17 District Hospitals and some SDH and RH<br />
• Ayurvedic and Unani Doctors are appointed on regular basis and 509 contractual<br />
AYUSH doctors are appointed in Rural, Sub-District and District Hospitals.<br />
Medicines are purchased through IPHS, RKS, DPDC and other available funds as<br />
Maharashtra did not receive AYUSH medicine grants from GoI.<br />
• Budget at state level will be utilized for IEC, Training, Contingency, innovatives and<br />
salary as per requirement.<br />
Plan of action – <strong>2012</strong>-<strong>13</strong><br />
• This year ‘Suvarnaprashan Sanskar’ facility will be provided at few institutes as<br />
an innovative.<br />
• Also we have decided to start ‘Ayurved Gram’in selected grams on pilot basis.<br />
PIP of AUSH scheme is in two parts as follows:
Part – A : Budget for Man Power for AYUSH specialists and staff under mainstreaming as well<br />
as IEC and Training in AYUSH is submitted to Mission Flexipool in this section.<br />
Part – B: Procurement of medicines, AYUSH equipment, instruments and civil works through<br />
AYUSH funds. This part will be submitted to AYUSH department<br />
Budget requirement<br />
Budget is required for establishing AYUSH Centers in hospitals under mainstreaming,<br />
establishment and functioning of District AYUSH cell and functioning of State AYUSH Cell. In<br />
Maharashtra, AYUSH Coordinator will be appointed in 22 districts for AYUSH administration.<br />
In 10 districts AYUSH officers are appointed as District AYUSH Officer in 2011-12.<br />
Currently, training of AYUSH doctors is in various National Health Programs. They did not<br />
have opportunity to get clinical training to update themselves in AYUSH. It is proposed to<br />
provide training to these officers in Ayurvedic Colleges. Curriculum for the training will be<br />
decided in consultation with Director (Ayurved). In addition to this, many of the allopathic<br />
doctors are also taking interest in Ayurvedic issues. It is proposed to provide one introductory<br />
training for such doctors.<br />
Training under AYUSH<br />
Training is important component of AYUSH. It is proposed to provide training of<br />
mainstreaming to AYUSH doctors, as well as training in specialized subjects such as<br />
Panchakarma, Ksharsutra. If additional budget is needed for these training, that will be met<br />
from regular training budget.<br />
It is also proposed to conduct training of Alopathic Doctors in basic AYUSH concepts and<br />
commonly used remedies in AYUSH.<br />
IEC/BCC under NRHM – Mainstreaming of AYUSH<br />
It is important to provide information of AYUSH to community. It is proposed to conduct<br />
AYUSH mela per district. No. may be increased as per demand and sanction from SHS.<br />
Summary of budget requirement<br />
Total requirement of Budget under AYUSH<br />
Table – Budget requirement under AYUSH-<strong>2012</strong>-<strong>13</strong><br />
Sir Particulars Months<br />
A Hospitals AYUSH Services<br />
PG MO (one each<br />
Ay/Ho/Un) at DH<br />
1 (Salary PG MO- @<br />
Budget<br />
/unit<br />
No. of<br />
Units<br />
66<br />
Rs. in Lakhs<br />
Total<br />
budget<br />
required<br />
12 2.33 37 86.14
Sir Particulars Months<br />
2<br />
3<br />
4<br />
5<br />
6<br />
Rs.19,400)<br />
PG MO (one each<br />
Ay/Ho/Un) at DH<br />
(Salary PG MO- @<br />
Rs.19,400)<br />
PG MO at WH<br />
(Salary PG MO- @<br />
Rs.18,000)<br />
UG MO at DH/SDH /RH<br />
(Salary of Graduate MO @<br />
Rs. 15,120/MO/PM)<br />
UG MO at DH/SDH /RH<br />
(Salary of Graduate MO @<br />
Rs. 15,120/MO/PM)<br />
Pharmacist one at DH<br />
(Salary @ Rs. 9180/ PM )<br />
Y & N at DH<br />
(Salary @ Rs. 7776/ PM )<br />
Y & N at Vacant of DH<br />
(Salary @ Rs. 7776/ PM )<br />
Y & N at WH<br />
(Salary @ Rs. 7200/ PM )<br />
Budget<br />
/unit<br />
No. of<br />
Units<br />
67<br />
Total<br />
budget<br />
required<br />
5 0.97 35 33.95<br />
5 0.90 8 7.56<br />
12 1.8 495<br />
5 0.75 79<br />
898.<strong>13</strong><br />
59.72<br />
12 1.10 24 26.44<br />
12 0.93 12<br />
5 0.39 12<br />
5 0.36 8<br />
11.20<br />
4.67<br />
2.88<br />
Massagist cum Atendant<br />
(Salary @ Rs. 7020/ PM)<br />
Total of AYUSH Hospital<br />
8 0.56 48 26.96<br />
Services<br />
Special budget for MO at<br />
1157.64<br />
PHC in Sindhudurg 12 1.68 36 60.48<br />
B District AYUSH Cell<br />
1<br />
Dist. AYUSH Officer<br />
(Salary @ Rs. 19400/ PM) 12 2.33 9 20.95
Sir Particulars Months<br />
3<br />
4<br />
Budget<br />
/unit<br />
No. of<br />
Units<br />
68<br />
Total<br />
budget<br />
required<br />
DEO for AYUSH Cell<br />
(Salary @ 10260) 10 1.03 33 33.86<br />
TA to DAO & Co<br />
coordinator<br />
(AYUSH Centre*5000) 0.05 245 12.25<br />
5 Contingency (DH*15000) 0.15 33 4.95<br />
Total of District AYUSH<br />
Cell 72.01<br />
C State AYUSH Cell<br />
AYUSH<br />
IEC,Training,TA/DA,<br />
innovative and<br />
1<br />
contingency and salary if<br />
required<br />
68<br />
Total State level Budget 68<br />
Grand total (A+B+C) <strong>13</strong>58.<strong>13</strong>
Year of starting<br />
the<br />
scheme/initiative<br />
SECTION - B.10 : IEC/BCC UNDER MISSION FLEXI-POOL<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2011-12 0 1251.41 1853.03 1439.03<br />
69<br />
Rs. in Lakhs<br />
Remarks<br />
In the developmental communication era IEC/BCC is playing very vital and strategic role and<br />
especially in the field of reproductive and child <strong>health</strong>, IEC & BCC activities are plying equally<br />
very important role. For generating demands regarding services available at grass root level<br />
and to create awareness in community is a very hard task for <strong>health</strong> and family welfare<br />
department.<br />
SUBSECTION – B.10.1 : STRENGTHENING OF BCC/IEC BUREAU<br />
In Maharashtra for planning, implementation and monitoring of IEC/BCC activities an<br />
independent State Health IEC Bureau is established in the year 1996 which is headed by the<br />
Deputy Director of Health Services, a Mass Media Specialist. Every district has a small IEC<br />
unit of 2-3 officials functioning under the supervision of District Health Officer.<br />
Planning, implementation and monitoring of various IEC/BCC activities under<br />
Reproductive & Child Health Program as well as other various <strong>national</strong> <strong>health</strong> programs are<br />
being carried out throughout the year through the State Health IEC Bureau. "Maharashtra<br />
Arogya Patrika’ a monthly magazine in Marathi is being published and circulated regularly by<br />
the State Health IEC Bureau for continuous <strong>health</strong> education to <strong>health</strong> providers and<br />
community in the State. Parivartan Express, a very unique Audio Visual Van is run by State<br />
Health IEC Bureau. Various activities such as <strong>health</strong> exhibitions, film shows are organized<br />
throughout the State with the help of this Parivartan Express.<br />
Table – Strengthening of IEC Bureau<br />
Sir Particulars Unit cost<br />
1<br />
2<br />
3<br />
4<br />
Hiring of IEC consultancy : Rs. 2.00 lakhs per<br />
month X 12 months = Rs. 12.00 lakhs<br />
Appointment of Communication expert to publish<br />
all the works / schemes of NRHM.<br />
Exhibition set for district media units: 33 districts<br />
X Rs. 1.5 lakhs per district = Rs. 66.00 lakhs<br />
Development of Information centre at IEC Bureau<br />
= Rs. 10.00 lakhs<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
12 1 12<br />
3.5 1 3.5<br />
1.5 33 49.5<br />
10 1 10
Sir Particulars Unit cost<br />
5<br />
6<br />
No. of<br />
units<br />
70<br />
Budget<br />
required<br />
POL to Audio Visual Van 'Parivartan Express' for<br />
state level exhibitions = Rs. 3.00 lakhs<br />
3 1 3<br />
POL to IEC van at districts = Rs. 1.00 lakhs X 33<br />
districts = Rs. 33.00 lakhs<br />
1 33 33<br />
Total 111<br />
SUBSECTION - B.10.2 : DEVELOPMENT OF STATE BCC/IEC STRATEGY<br />
The State has developed on IEC/BCC strategy with focus on interpersonal communication,<br />
print and electronic media, community media such as folk art, rallies, street plays, newspaper<br />
advertisements as well as local need based IEC activities at district level.<br />
No budget is requested for this activity for year <strong>2012</strong>-<strong>13</strong>.<br />
SUBSECTION - B.10.3: IMPLEMENTATION OF BCC/IEC STRATEGY<br />
While implementing IEC/BCC Plan following issues will be focused.<br />
• Message will be well designed to solve the identified <strong>health</strong> problems and<br />
issues.<br />
• IEC/BCC Messages, Material and media will be linked with programme objectives.<br />
• Integrated approach will be adopted for implementing IEC/BCC activities.<br />
• Programmes will be strictly monitored for timely dispatch of IEC material to proper<br />
destination and its utilization<br />
• Instead of mass media approach, IPC approach will be adopted for disseminate the<br />
message among the <strong>rural</strong> masses.<br />
• The district will be focal point for developing local specific IEC.<br />
• Special training programme will be organized for developing the communication skills<br />
of service providers and IEC personals.<br />
• State will encourage the Best IEC practices.<br />
• Role of different functionaries for implementation and supervision will be ensured.<br />
• Decentralized and participatory approach will be adopted.<br />
• Service providers at grass root level will be equipped with proper IEC material<br />
methods.<br />
and<br />
• Media people as well as journalists will be encouraged with best awards.<br />
• Health Melas will be organized for mass awareness.<br />
• Mass publicity campaigns will be organized for declining the sex ratio.<br />
Activities for B.10.3.1 to B.10.3.4<br />
Inter personal communication
For behavioral change, Inter personal communication is very effective tool. For this purpose,<br />
counseling and interactive sessions with ASHAs, ANMs, and Anganwadi Workers, group<br />
meetings at village and block level, workshop for women groups, community leaders,<br />
adolescent groups at block and district level has been proposed. 358 workshops at block level<br />
(@Rs. 5000) and 33 workshops at district level (@Rs. 10000) total<br />
Rs. 21.20 lakh are proposed for the IPC activities.<br />
Community media - Folk Art:<br />
For creating awareness regarding various <strong>health</strong> programs and projects, the activities like folk<br />
art, Rallies, Street plays have been proposed. 300 folk programs @Rs. 4000 will be organized<br />
in each district. Provision of Rs. 12 lakhs is made in the PIP.<br />
Community media - Rallies:<br />
On occasion of <strong>health</strong> days, fairs and campaigns, 5 rallies in each district @ Rs. 10000 will be<br />
organized. Rs. 16.50 lakhs have been proposed for 165 rallies.<br />
Outdoor media - print materials:<br />
For the use of <strong>health</strong> providers and beneficiaries, the print material like folders, flash cards<br />
and flip books are very useful. Folders and flash cards are very easy to carry and it can be<br />
used in small groups. The flip books will be used by <strong>health</strong> workers for Inter personal<br />
communication or group discussions. The issues like Mother and Child care, Immunization,<br />
Breast Feeding, PCPNDT, NSV, JSSK. JSY, Institutional delivery, referral services, Nutrition, Age<br />
at Marriage, Spacing methods will be sensitized through the print material. For creating<br />
awareness and demand generates pictorial message will be given through flex banners,<br />
hoardings and electricity bills. The message regarding JSY, NSV, PCPNDT, Immunizations, Age<br />
at Marriage will be given through banners and these banners will be displayed at various<br />
<strong>health</strong> institutions like District hospitals, RH, PHCs etc.. There are 162 hoardings in the<br />
premises of <strong>health</strong> institutes and bus stands. Messages will be displayed on all the 162<br />
hoardings. The message on electricity bill is one of the very useful medium which reach in<br />
every house regularly. The message regarding PCPNDT will be given on 50 lakh bills in<br />
selected districts. Following are the item-wise budgetary details:<br />
• Folders - 1,00,000 folders x 10 subjects x Rs. 2.00 = Rs. 20.00 lakhs.<br />
• Flash cards - 10,00,000 flash cards x 10 subjects x Rs. 1.00 = Rs. 100.00 lakhs<br />
• Flip books - 5000 flip books x 3 subjects x Rs. 50.00 = Rs. 7.50 lakhs<br />
• Flex banners (6' x 4' x 2') - 12,000 banners x 5 subjects x Rs. 120/- = Rs. 72.00 lakhs<br />
• Messages on hoardings - Rs. 3100 x 162 hoardings = Rs.45.20 lakhs<br />
Thus, a budget of Rs. 244.70 lakhs is proposed during the year <strong>2012</strong>-<strong>13</strong> for the above<br />
publicity materials.<br />
71
Electronic media:<br />
To reach the masses, television and radio is the best option. The T.V. & Radio programs are<br />
watched by all classes of community. Various programs like serials, dances and music, News,<br />
discussions, interviews are telecasted and broadcasted for different target groups.<br />
Considering the importance of T.V. & Radio following activities are proposed.<br />
• Telecasting of TV spots : Rs. 60,000/- per telecast x 475 telecasts = Rs. 285.00 lakhs<br />
• Broadcasting of Radio Jingles : Rs. <strong>13</strong>,000/- per broadcast x 500 broadcasts = Rs.65.00<br />
lakhs<br />
Thus, a budget of Rs350.00 lakhs is proposed during the year <strong>2012</strong>-<strong>13</strong> for publicity through<br />
electronic media.<br />
Newspaper advertisements:<br />
Newspaper is very popular and effective medium, through which <strong>health</strong> messages can be<br />
reached up to different target groups. Pictorial advertisements will be published in<br />
newspapers @ Rs. 20000/- per advertisement x 600 advertisements. Thus, a budget of Rs.<br />
120.00 lakhs is proposed for this<br />
activity.<br />
Summary of budget requirement<br />
Table – Budget required for Implementation of IEC/BCC strategy<br />
Sir Activity<br />
Rs. In Lakhs<br />
Budget<br />
1 Inter-personal communication 21.2<br />
2 Community media (Folk art) 12<br />
3 Community media (Rallies) 16.5<br />
4 Print material 244.7<br />
5 Electronic media 350<br />
6 Newspaper advertisements 120<br />
Total 764.4<br />
SUBSECTION - B.10.4 : HEALTH MELA<br />
For mass awareness regarding various <strong>health</strong> programs, <strong>health</strong> mela is the best opportunity.<br />
We can provide <strong>health</strong> check-up services as well as awareness campaign in the same mela. In<br />
Maharashtra, there are eight <strong>health</strong> circles. One <strong>health</strong> mela in each <strong>health</strong> circle will be<br />
organized. Each Mela will be for the period 3 days. The mela will be organized in selected big<br />
hospital premises or public ground. The facilities for <strong>health</strong> check-ups and diagnostic purpose<br />
will be provided to community by specialists. Health exhibitions, film shows, folk programs<br />
will be arranged in the mela. IEC material will be distributed to the beneficiaries.<br />
72
Pre-publicity of the camp through banners, posters, Davandi, Radio publicity will be done.<br />
Transport of public to the venue of Health mela, Remuneration of Private Specialist doctors (if<br />
required) and mela expenditure will be required.<br />
Rs. 8.00 lakhs X 8 circles = Rs.64.00 lakhs<br />
SUBSECTION - B.10.5 :CREATING AWARENESS ON DECLINING SEX RATIO ISSUE<br />
Declining sex ratio is one of the big challenge before <strong>health</strong> services in the state. State is<br />
tackling this issue with creating awareness as well as implementations of law.<br />
For creating awareness, the media like T.V., Radio, Newspaper, hoardings, messages<br />
on electricity bills, Rallies, pictorial floats, banners, posters, exhibitions, folk program will be<br />
utilized.<br />
(1) Telecasting of TV spots : Rs. 60,000/- per telecast x 100 telecasts = Rs 60.00 lakhs<br />
(2) Broadcasting of Radio Jingles : Rs. <strong>13</strong>,000/- per broadcast x 46 broadcasts = Rs. 06.00<br />
lakhs<br />
(3) Messages on electricity bills - Rs. 1.60 x 50 lakh bills = Rs. 80.00 lakhs<br />
(4) Newspaper advertising : Rs 15,000 X 100 advertisements = Rs. 15.00 lakhs<br />
Thus, a budget of Rs 161.00 lakhs is proposed during the year <strong>2012</strong>-<strong>13</strong> for this<br />
activity.<br />
SUBSECTION - B.10.6 : OTHER ACTIVITIES<br />
Awards for Journalists<br />
Award will be honored to journalists for best press articles and stories on 'Mother and Child<br />
Health' topic. For the award scheme, evaluation of articles will be done by expert committee.<br />
and awards will be distributed in a special function at state level. Details of the award scheme<br />
are as follows:<br />
1) Selection procedure : Rs. 2.00 lakhs<br />
2) Award distribution ceremony : Rs. 2.00 lakhs<br />
3) Pre-publicity of award scheme : Rs. 25.00 lakhs<br />
4) Prizes : Rs. 00.63 lakhs<br />
( I prize : Rs. 25,000/- + II prize : Rs. 15,000/- + III prize: Rs. 10,000/- + IV prize : Rs.<br />
1,5000/- + V prize : Rs. 5,000/-)<br />
Thus. a budget of Rs. 29.63 lakhs is proposed for this award scheme.<br />
73
Award to district for best performance in IEC :<br />
Awards will be given to best three districts on performance basis in IEC. Evaluation will be<br />
done on the performance of the year 2011-12 and the winner districts will be awarded with a<br />
momento in the same function of journalists. Therefore budget is requested only for awards.<br />
A budget of Rs. 2.00 lakhs is proposed for this purpose.<br />
Exhibitions in major fairs in districts:<br />
In each district, exhibitions, film shows will be arranged in the major fairs where more than 1<br />
lakh people gathered. 5 exhibitions will be arranged per year. in each district. Thus 165<br />
exhibitions will be arranged in 33 districts.<br />
Rs. 20,000 X 165 exhibitions = Rs. 33.00 lakhs<br />
Budget required for other activities<br />
Total budget required for other activities is as mentioned in table below:<br />
Table – Budget requirement for other activities<br />
Rs. In Lakhs<br />
Sir Particulars Unit cost No. of units<br />
Budget<br />
required<br />
1 Awards for journalists 29.63 1 29.63<br />
2 Award to district for best performance in IEC 2 1 2<br />
3 Exhibitions in major fairs in districts<br />
Printing of Maharashtra Arogya Patrika Magazine<br />
0.2 165 33<br />
4<br />
and to provide it to Sarpanch, ASHAs, all <strong>health</strong><br />
institutes in the state (97,000 copies per month X<br />
97<br />
10 months) = 9,70,000 X Rs. 10 = Rs. 97.00 lakhs<br />
Funds will be given to 6 tribal districts for printing<br />
0.0001 970000<br />
5 of IEC material in local tribal language = 6 districts X<br />
16<br />
Rs. 2.00 lakhs = Rs. 12.00 lakhs 2 8<br />
6<br />
Preparation of floats on the occasion of 15 th August<br />
and 26 th January = Rs. 1.00 lakh X 33 districts =33<br />
33<br />
Lakhs<br />
1 33<br />
Total 210.63<br />
74
Budget summary for IEC/BCC activities – <strong>2012</strong>-<strong>13</strong><br />
Total budget required for the state considering implementation of above mentioned activities<br />
is as follows:<br />
Table – Budget required for IEC/ BCC activities - <strong>2012</strong>-<strong>13</strong><br />
Rs. In Lakhs<br />
Sr Activity Budget proposed<br />
1 Strengthening of BCC/IEC Bureau 111<br />
2 Development of State BCC/IEC Strategy 0<br />
3 Implementation of BCC/IEC Strategy 764.4<br />
4 Health Mela 64<br />
5 Creating awareness on declining sex ratio 161<br />
6 Other activities 210.63<br />
Total <strong>13</strong>11.03<br />
75
Year of starting<br />
the<br />
scheme/initiative<br />
SECTION - B.11 : MOBILE MEDICAL UNITS<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2008-09 <strong>13</strong>53.06 608.02 932.92 932.920<br />
76<br />
Rs. in Lakhs<br />
Remarks<br />
National Rural Health Mission, Framework for Implementation (2007-12) has mentioned<br />
support to Mobile Medical Units in <strong>rural</strong> areas of the state. Objective of providing these units<br />
is to take <strong>health</strong> care to the doorstep of the public in the <strong>rural</strong> areas, especially in underserved<br />
areas. For states like Maharashtra, GOI has suggested MMU with diagnostic facilities.<br />
Vehicles for all the 40 MMU have been received and MMU has started functioning. Work<br />
done by MMUs in last two months is as follows:<br />
Table : Work done by MMU in 2011-12<br />
Sir Indicator<br />
Work done<br />
December 2011 Progressive<br />
1 OPD 3<strong>13</strong>58 148890<br />
2 ANC Checkup 1748 6002<br />
3 PNC Checkup 1088 2768<br />
4 Urine test 1<strong>13</strong>3 3276<br />
5 Blood tests 2316 8856<br />
6 BS for MP 729 2720<br />
7 Sputum for AFB 323 893<br />
8 VDRL Test 283 996<br />
Recurring Cost per MMU<br />
NRHM guidelines have suggested Rs. 19.87 Lakh /district /annum as recurring cost for MMU.<br />
Recurring cost include salary of MMU staff and operational expenses. Salary of MMU staff is<br />
proposed as follows:<br />
Table : Salary of MMU staff<br />
Rs. in Lakhs<br />
Sir Name of the staff Monthly salary<br />
Salary for <strong>2012</strong>-<br />
<strong>13</strong><br />
1 Medical Officer 0.3 3.6
Sir Name of the staff Monthly salary<br />
Salary for <strong>2012</strong>-<br />
<strong>13</strong><br />
2 Staff Nurse 0.<strong>13</strong> 1.56<br />
3 Pharmacist 0.1 1.2<br />
4 Lab-technician 0.1 1.2<br />
5 Driver (Dispensary vehicle) 0.07 0.84<br />
6 Driver (passenger vehicle) 0.07 0.84<br />
Total 0.64 9.24<br />
MMU of Maharashtra have started functioning from July 2011. Considering the experience of<br />
last 6 months, the recurring cost is calculated. MMU are getting very good response, so there<br />
is substainal increase in recurring cost. It is requested to sanction the revised cost. Last year<br />
recurring cost was for half year so it was less. Cost is increased in following areas:<br />
1. There is slight increase in salary of staff as annual salary increase is 8% in<br />
Maharashtra.<br />
2. Recurring cost of vehicles increased as there is increase in Diesel prices and also now<br />
the vehicles will be out of warranty.<br />
3. Budget for medicines increased as OPD has increased by 150% then expected. This is<br />
seen from the report of this scheme.<br />
Each of the activity implemented by State is monitored from State level. Weekly performance<br />
of all MMU is monitored from State level. Monthly report of all the visits on daily basis are<br />
collected and analysed. Inventory of medicines, equipment and consulambles is also<br />
monitored. For all these activities, we need monitoring cell. Therefore, it is requested to<br />
continue the monitoring cell.<br />
Medical officers and nurses of MMU need to be trained every year for refreshing the<br />
knowledge and also to introduce them to various activities being introduced in the State.<br />
Considering this, this activity may also be approved.<br />
Considering the patient load of MMU and experience of SHS Maharashtra regarding<br />
operational cost per MMU, budget as mentioned below is requested :<br />
Table : Recurring cost of MMU : <strong>2012</strong>-<strong>13</strong><br />
Sir Particulars Unit rate<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
A Recurring cost of MMU<br />
1 Salary of MMU Staff 9.24 40 369.6<br />
1 Recurring cost of vehicles 6 40 240<br />
2 Maintenance of equipment 0.72 40 28.8<br />
3 Consumables 1.2 40 48<br />
77
Sir Particulars Unit rate<br />
No. of<br />
units<br />
78<br />
Budget<br />
required<br />
4 Medicines 3.5 40 140<br />
6 Reporting, stationary and meeting expenses 0.36 40 14.4<br />
7 Overheads 2 40 80<br />
Total 920.8<br />
B MMU cell at SPMU<br />
1 Salary of Program Officer 3 1 3<br />
2 TA/DA to Program Officer 0.6 1 0.6<br />
3 Salary of Program Assistants 1.26 2 2.52<br />
4 Contingency at SHS including civil works 1.2 1 1.2<br />
Total 7.32<br />
C Training of MMU Staff 1.2 4 4.8<br />
Grand Total 932.92
SECTION - B.12 : REFERRAL TRANSPORT<br />
SUBSECTION – B.12.1& B.12.2 : PRE HOSPITAL EMERGENCY MEDICAL RESPONSE<br />
(AMBULANCE) SERVICES (EMS)<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2010-11 4944.5 3076.28 10785.4 1<strong>13</strong>01.400<br />
79<br />
Rs. in Lakhs<br />
Remarks<br />
Emergency Medical Services exists to fulfill the basic principles of first aid, which are to<br />
Preserve Life, Prevent Further Injury, and Promote Recovery. This strategy developed for prehospital<br />
trauma care is based on the Golden Hour Theory, i.e. that a trauma victim’s best<br />
chance for survival is in well equipped hospital so the patient should be shifted to hospital<br />
within one hour. Currently, ambulance services provide as a transport operation only, simply<br />
to take patients from their location to the nearest medical treatment.<br />
Considering the importance of establishment of pre-hospital emergency medical response, it<br />
is decided to establish such service in Maharashtra.<br />
1. Activities Completed<br />
Following actions have been taken so far for this purpose:<br />
• Proposal submitted to Government regarding establishment of services.<br />
• Cabinet decision for establishment of pre-hospital ambulance services in state.<br />
• AIIMS, New Delhi is appointed as consultant agency to establish the scheme in<br />
state.<br />
• Financial bid opened and negotiation with L-1 in progress.<br />
2. Plan of action for <strong>2012</strong>-<strong>13</strong><br />
During <strong>2012</strong>-<strong>13</strong> agency will be selected for delivery of pre-hospital emergency medical<br />
care with the help of consultants. Services will be provided in the state in phased<br />
manner.<br />
Hospitals will be prepared in the areas as per recommendation of consultants. Help of<br />
IPHS upgraded hospitals will be taken for this purpose. If required private <strong>health</strong> care<br />
providers will also be considered. MIS system will be developed for the pre-hospital<br />
emergency medical response services.<br />
3. Requirement of Ambulance<br />
This project is of total 937 ambulances. Out of these,247 Ambulance will be for<br />
Corporation areas
and 690 Ambulance for <strong>rural</strong> areas of the state. Detailed year wise breakup of<br />
Ambulance is<br />
Mentioned below:<br />
Table-Yearwise requirement of Ambulances<br />
Sr.No Year NRHM GOM Total<br />
ALS BLS Total ALS BLS Total ALS BLS Total<br />
1 <strong>2012</strong>-<br />
<strong>13</strong><br />
86 259 345 31 93 124 117 352 469<br />
2 20<strong>13</strong>-<br />
14<br />
86 259 345 30 93 123 116 352 468<br />
Total 172 518 690 61 186 247 233 704 937<br />
Explanation for remarks on EMS<br />
• Population coverage for the ambulances is 1.0 Lakh population in <strong>rural</strong> areas and 2.0 Lakh<br />
population in urban areas. As NRHM supported ambulances will be plying in mainly <strong>rural</strong><br />
areas, they will cover 6.90 Crore population of the state.<br />
• These ambulances will be provided to women for delivery in case of emergency only. Thus<br />
mother in obstructed labour, heavy bleeding, etc. will be transported. However, planned<br />
ad<strong>mission</strong> or transportation after delivery will not be carried out by the EMS ambulances.<br />
• OPEX budget is for following activities:<br />
o Procurement of ambulances – Rs. 32.3 Lakh for ALS ambulance (172 ambulances) and<br />
Rs. 22.05 Lakh for BLS Ambulance (518 Ambulances).<br />
o Software for the scheme and State Control Room – Rs. 1000.0 lakh.<br />
• This scheme cannot be compared with JSSK, because under JSSK, we are providing transport<br />
to women for delivery who are not in labour and for discharge of mothers also. Similarly for<br />
neonates, services are provided after discharge through regular ambulances. Hospital to<br />
hospital referral if it is not emergency will not be covered under EMS. Considering this, it is<br />
clear that these two services are not duplication of services but are complementary to each<br />
other.<br />
Considering above explanation, it is requested to approve this activity.<br />
1. Budget requirement for year <strong>2012</strong>-<strong>13</strong><br />
Budget required is for three major activities. These are:<br />
• Procurement of ambulances<br />
• Recurring cost of ambulances (operational cost)<br />
• Cost of establishment of the Central Station and Software<br />
• Cost for establishment of monitoring mechanism<br />
Detailed budget related information is as follows:<br />
80
Financial bid of tender is opned.The L-1 rates are Capital cost:Rs.32.3 Lakh/ALS ambulance<br />
and Rs.22 .05Lakh/BLS ambulance. Operational cost : Rs. 1.5 Lakhs/ALS ambulance per month<br />
and Rs. 1.4 Lakh/BLS abundance/month.<br />
During year <strong>2012</strong>-<strong>13</strong>, total 468 Ambulances are proposed to be purchased. Out of these, 124<br />
Ambulances are for Corporation areas and 344 Ambulances for Rural areas.<br />
For Ambulances provided to Corporation areas, total expenditure of procurement of<br />
ambulances and recurring cost will be borne by Government of Maharashtra.For Ambulances<br />
of Rural areas, NRHM will bear 100% capital cost and 60% recurring cost and GoM will<br />
bear 40% recurring cost. Recurring cost share of GoM will increase to 60% in 20<strong>13</strong>-14 and<br />
80% in 2014-15.<br />
Budget requirement as per abovementioned facts is submitted in table below:<br />
Si<br />
r<br />
Table - Budget requirement of EMS – NRHM and GoM share – <strong>2012</strong> – <strong>13</strong><br />
Rs. In Lakhs<br />
Rate/unit cost NRHM GoM Total<br />
Activity<br />
NRH<br />
M<br />
GoM No Budget<br />
Required<br />
No Budget<br />
Require<br />
d<br />
81<br />
No Budget<br />
Require<br />
d<br />
A Capital<br />
Expenditure<br />
1 ALS Ambulances 32.3 32.3 86 2777 31 1001 117 3778<br />
(100 exp of NRHM<br />
veh by NRHM and<br />
100% exp of GoM<br />
veh by GoM)<br />
2 BLS Ambulances 22.05 22.05 259 5710 93 2050 352 7760<br />
(100 exp of NRHM<br />
veh by NRHM and<br />
100% exp of GoM<br />
veh by GoM<br />
Total 345 8487 124 3051 469 11538<br />
B Recurring<br />
Expenditure<br />
1 ALS-GoM<br />
Ambulances<br />
0 9 0 0 31 279 0 279<br />
(100%<br />
GoM)<br />
Exp by<br />
2 ALS – NRHM 5.4 3.6 86 464.4 86 309.6 774<br />
Ambulance (60%<br />
exp by NRHM &<br />
40% exp by GoM)
Si<br />
r<br />
Activity<br />
Rate/unit cost NRHM GoM Total<br />
NRH<br />
M<br />
GoM No Budget<br />
Required<br />
No Budget<br />
Require<br />
d<br />
82<br />
No Budget<br />
Require<br />
d<br />
3 BLS – NRHM 0 8.4 0 0 93 781.2 781.2<br />
Ambulances<br />
(100%<br />
GoM)<br />
Exp by<br />
4 BLS – NRHM 5 3.4 259 1295 259 880.6 2175.6<br />
Ambulances (60%<br />
exp by NRHM &<br />
40% exp by GoM)<br />
Total 1759.4 2250.4 4009.8<br />
Grand Total 10246.4 5301.4 15547.8<br />
As mentioned in table above, budget required from NRHM side for procurement and running<br />
of ambulances for year <strong>2012</strong>-<strong>13</strong> is Rs.10246.4 Lakhs.<br />
In addition to ambulance services, budget will also be required for establishment of Central<br />
Station, software and monitoring of the EMS. Therefore total budget required for the Prehospital<br />
Emergency Medical Response Service for NRHM during the year <strong>2012</strong>-<strong>13</strong> will be as<br />
mentioned in table below:<br />
Table: Budget required for EMS from NRHM<br />
RS. In Lakhs<br />
Sr. No. Particulars Budget<br />
Required<br />
1 Contribution of NRHM- 1 st year (100 capital and 60% recurring) 10246.4<br />
2 Budget required for software, establishment of control room and<br />
incidental expenses (approximate)<br />
1000<br />
3 Budget required for appointment of one senior officer as<br />
consultant and co-coordinator for EMS<br />
4.80<br />
4 Budget required for appointment of Program Officer (1) 2.88<br />
5 Budget required for appointment of 2 Medical Officer (Rs.3.6 L x 2) 7.20<br />
6 Budget required for appointment of Training Consultant (1),<br />
Program Officer IT (1), Bio-medical Engineer (1), Mechanical<br />
Engineer (1) for EMS (Rs.2.88 L x 4)<br />
11.52<br />
7 Budget required for appointment of 1 Accountant (Rs. 1.2) 1.20<br />
8 Budget required for appointment of 2 Program Assistant (Rs. 1.2 L<br />
x 2)<br />
2.40<br />
9 Budget required to for PEMRS cell establishment and consultancy<br />
services<br />
25.00<br />
Total 1<strong>13</strong>01.4
SECTION - B.<strong>13</strong> : SCHOOL HEALTH PROGRAM<br />
(Proposed in RCH Flex-pool)<br />
83
SECTION - B.14 : PPP/NGOs<br />
SUBSECTION - B.14.1 : NON-GOVERNMENTAL PROVIDERS OF HEALTH CARE (RMPs/TBAs)<br />
(No budget requested)<br />
SUBSECTION - B.14.2 : PNDT AND SEX RATIO<br />
(Budget requested under RCH)<br />
SUBSECTION : B.14.3.1: INVOLVEMENT OF PRIVATE SPECIALIST ORGANIZATION FOR<br />
PROVIDING SPECIALISTS<br />
The Activity has been deleted. PPP Cell is responsible for all the activites being implemented<br />
in collaboration with private organisations. This cell is shifted to Program Management with<br />
due explanation.<br />
Subsection : B.14.3.2 : ORGANIZATION OF EPILEPSY CAMPS WITH THE HELP OF EPILEPSY<br />
FOUNDATION MUMBAI<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed in<br />
PIP <strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed in<br />
NPCC<br />
2011-12 0 15.9 68.2 53.900<br />
84<br />
Rs. in Lakhs<br />
Remarks<br />
Epilepsy is one of the chronic diseases with significant prevalence in school going<br />
children's & in adults but very little attention is given as compare to other important disease<br />
in the public <strong>health</strong> . More than 5000 students have been found having Epilepsy in the state<br />
who requires specialist care to overcome this problem. Seven Epilepsy Camps were organized<br />
at district places in the state during 2011-12.<br />
The detail performance of Epilepsy camps conducted in 2011-12 is as follows.<br />
Table – Performance of Epilepsy Camps conducted during year 2011-12<br />
Sr.No District Hospital No of Neuro<br />
physician or<br />
epidemiologi<br />
st present in<br />
camps.<br />
1 Sindhudurg District<br />
Hospital,<br />
Total No.<br />
Of<br />
epilepsy<br />
patients<br />
examined<br />
& treated<br />
No. Of EEG<br />
(Electro<br />
Encephalo<br />
grams)<br />
test done<br />
No. of<br />
patients<br />
and<br />
parents<br />
given<br />
counseling<br />
by<br />
psychologi<br />
st<br />
9 120 26 45
Sr.No District Hospital No of Neuro<br />
physician or<br />
epidemiologi<br />
st present in<br />
camps.<br />
Oras<br />
Total No.<br />
Of<br />
epilepsy<br />
patients<br />
examined<br />
& treated<br />
No. Of EEG<br />
(Electro<br />
Encephalo<br />
grams)<br />
test done<br />
85<br />
No. of<br />
patients<br />
and<br />
parents<br />
given<br />
counseling<br />
by<br />
psychologi<br />
st<br />
2 Nashik District<br />
Hospital<br />
Nashik<br />
15 167 58 35<br />
3 Satara District<br />
Hospital<br />
Satara<br />
19 376 57 50<br />
4 Parbhani District<br />
Hospital<br />
Parbhani<br />
14 155 46 40<br />
5 Amravati District<br />
Hospital<br />
Amravati<br />
14 399 55 60<br />
6 Thane Sub–District<br />
Hospital<br />
Jawhar<br />
6 183 40 41<br />
7 Gondia District<br />
Hospital<br />
Gondia<br />
9 588 117 35<br />
Total 7 1988 399 306<br />
There are many children and women suffering from Epilepsy. Stigma about this<br />
disease prevents them to get proper care and treatment. Students suffering from Epilepsy are<br />
particularly at disadvantages as early diagnosis and treatment will cure the disease and also<br />
will not affect the academic performance of the child.<br />
Considering above situation, following actions are proposed during the year <strong>2012</strong>-<strong>13</strong><br />
• Campaign to educate the community about misconceptions about Epilepsy prevention<br />
and treatment.<br />
• Organization of eleven Epilepsy camps in the state for diagnosis & treatment of<br />
Epilepsy in collaboration with Epilepsy Foundation Mumbai.<br />
• To provide counselling to the epileptic patient and relatives.<br />
• To provide OT, PT and speech therapy to epileptic patient.
Budget requirement<br />
Budget will be required for following activities<br />
• Transportations of the specialists<br />
• Staying arrangements for specialists<br />
• Incidental charges for the camp arrangement & Stationery for the camps.<br />
• Medicines, consumables, etc.<br />
• IEC<br />
It is proposed to organize 11 camps in various districts of Maharashtra during <strong>2012</strong>-<strong>13</strong>.<br />
Detailed budget requirement is as follows:<br />
Table -: Budget required for Epilepsy camps<br />
86<br />
Rs. In Lakhs<br />
SR Activity Unit cost<br />
No. of.<br />
units<br />
Budget<br />
required<br />
1 Travel charges to specialists and team 1 11 11<br />
2 Staying arrangements for specialists 0.3 11 3.3<br />
3 Arrangements of camps 0.25 11 2.75<br />
4<br />
Honorarium to EEG technicians OT, PT<br />
and speech therapy technician<br />
0.1 11 1.1<br />
5 IEC for camps 0.5 11 5.5<br />
6<br />
7<br />
Medicines and consumables for camps<br />
and for regular treatment ( Regular camp<br />
2.00 lakh and follow-up Medicine 1.00<br />
lakh)<br />
2.5 11 27.5<br />
Diet facility to the patients (Tribal areas<br />
only)<br />
0.25 11 2.75<br />
Total 6.2 53.9<br />
B.14.3.3: PROVIDING TELEMEDICINE SPECIALTY NODE TO EPILEPSY FOUNDATION FOR FREE<br />
CONSULTATION AND FOLLOW UP OF EPILEPSY PATIENTS<br />
The scheme is not proposed as per GOI Comment
B.14.3.4: CAPACITY BUILDING AND ORGANIZATION OF EPILEPSY DAY<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed in<br />
NPCC<br />
New 0 0 25.6 21.600<br />
87<br />
Rs. in Lakhs<br />
Remarks<br />
Epilepsy is one of the important diseases of Public Health Importance. The prevalence of<br />
epilepsy is an average one in thousand children & also quite common in adult populations<br />
there are many new methods come for diagnosis & treatment. More than five thousand<br />
school boys are dictated suffering of from Epilepsy in school <strong>health</strong> examinations. To treat<br />
them properly & give regular follow-up, training of Paediatrician & Physician from district<br />
hospital along with the nurses is proposed.<br />
There could be many children & women suffering from Epilepsy. Stigma about this<br />
disease prevents them to great a good care & service. There are many misconceptions<br />
regarding Epilepsy in society. Considering above situation the following action is proposed<br />
during the year <strong>2012</strong>-<strong>13</strong>.<br />
• Training of Medical Officer to improve the diagnostic skill<br />
• Proper treatment to the epileptic patients by Health care provider<br />
• Regular follow-up & proper management of the patients<br />
• Improve the skill & Knowledge of nurses for patients care<br />
• Create awareness in society regarding Epilepsy<br />
• Organization of Epilepsy day in the state to create the awareness<br />
The Epilepsy Foundation, Mumbai non -profit organization from Mumbai with a panel<br />
of eminent neuro physician is willing to provide technical resource free of cost.<br />
The budget provision for the capacity building of Paediatrician, Physician & other<br />
Medical Officer including nurses is as follows.<br />
Budget Proposed <strong>2012</strong>-<strong>13</strong><br />
(Rs. In Lakhs)<br />
No.<br />
SR Particulars Unit cost of.<br />
units<br />
1. Organization of one day training to the<br />
Medical Officer (Paediatrician &<br />
Physician)<br />
Budget<br />
required<br />
0.10 100 10.00
2. Organization of three day workshop for<br />
hospital nurses<br />
0.05 100 5.00<br />
3. Organization of Epilepsy day & IEC 0.20 33 6.60<br />
Total 0.35 21.6<br />
B.14.3.5: HEALTH ADVISE CALL CENTER<br />
Year of starting<br />
the scheme/<br />
initiative<br />
2011-12<br />
SUMMARY INFORMATION OF THE SCHEME / INITIATIVE<br />
88<br />
(Rs. In Lakhs)<br />
Remarks<br />
The Government of India accorded approval to set Health Advice Call Centre in<br />
Maharashtra during 2011-12. The Objective of the Health Advice Call Centre is 24x7 medical<br />
advices to <strong>health</strong> care provider for quick decision to provide smooth, effective and qualitative<br />
<strong>health</strong> care. To begin with a Call Centre of 10 seats is to be set during the year.<br />
The <strong>health</strong> advice is be given to caller who is dialling simply 3 digit toll free number<br />
“104” from landline or any mobile phone. To begin with the call centre is rendering advice to<br />
ANMs, ASHA worker, School Health personnel and Medical Officers of PHC & NGOs from<br />
NRHM, It will guide <strong>health</strong> personnel’s for timely referral, proper intervention and<br />
managements of the patients and effective implementation of National Health Programs. It<br />
will work as an effective tool for disease surveillance and also in disaster management.<br />
The Health Advice Call Centre will be fully functional from 23 January <strong>2012</strong>.<br />
The Health Advice Call Centre will be very useful for giving instructions to the Health<br />
Care Provider during Epidemics and other various Health Campaigns.<br />
The specialist’s advice by Paediatrician, Gynaecologist and Public Health Specialists<br />
will be provided 24x7 to the caller.<br />
Objectives:-<br />
Budget<br />
sanctioned for<br />
year 2011-12<br />
(in lakhs)<br />
143<br />
Budget proposed for<br />
PIP <strong>2012</strong>-<strong>13</strong> (in<br />
lakhs)<br />
184.60<br />
Budget<br />
proposed to<br />
NPCC (in<br />
lakhs)<br />
86.690<br />
1) 24x7 free call for <strong>health</strong> information to <strong>health</strong> care provider.<br />
2) Provide Medical advice on minor ailments.
3) To give guidance to the Medical and Paramedical Health Care Provider for School<br />
Health Program (Examination & Treatment)<br />
4) To give 24x7 Technical supports to Health Care Provider for smooth and effective<br />
<strong>health</strong> care.<br />
5) Provide Information to Health Care Providers for quick action in epidemic<br />
outbreak, disaster, natural calamities and in major accidents.<br />
6) Guidance to Health Care Provider for effective implementation of Various National<br />
& State Health Program.<br />
7) Provide Directory Information of hospitals/Institutes regarding various services /<br />
Facility including Blood bank and Eye bank for proper and early referral.<br />
8) Guidance to Mobile Medical unit , Medical officer & others staff<br />
9) Guidance to NGO of sickle cell disease for effective implementation of program.<br />
Linkages<br />
1) Linkage with EMS<br />
2) Linkage with Referral Transport<br />
3) Linkage with other Help lines with <strong>health</strong> department.<br />
Implementation Strategies:-<br />
This project is implemented on turnkey basis. In first phase Call Centre of 10 seats to<br />
be set. The service provider has established the call centre (control room), appointed the<br />
manpower for this call centre, given training to them and has to run the call centre. The<br />
service provider has developed all required software and provided hardware.<br />
HMRI, Hyderabad is a service provider for Health Advice Call Centre. The MOU is done<br />
with HMRI, Hyderabad on 11/10/2011.<br />
The ownership of software, hardware and project vest Government of Maharashtra.<br />
The call centre is being set at Pune Chest Hospital, Aundh, Pune. The call will be answered in<br />
Marathi and English.<br />
Budget required<br />
The recurring expenditure will be for salary to staff, call charges and maintenance of the<br />
system.<br />
It is proposed that recurring cost for the year <strong>2012</strong>-<strong>13</strong>, 60% of recurring cost will be borne by<br />
NRHM and 40% by State Government. The share of NRHM in recurring cost will reduced from<br />
60% to 40% in second year then it will reduce to 20% in third year. Considering this, budget<br />
required for this scheme is as follows:<br />
Table – budget required for Health Advice Call Centre <strong>2012</strong>-<strong>13</strong><br />
89<br />
Rs. In Lakhs
Type of<br />
Budget<br />
Total budget required for year <strong>2012</strong>-<br />
<strong>13</strong><br />
NRHM<br />
Share<br />
State Share Budget<br />
Required<br />
Remarks<br />
Capital Cost 10 0 10 • Two seat to be added for<br />
additional specialist physician &<br />
surgeon.<br />
Recurring<br />
cost<br />
• 100% capital cost contribution by<br />
NRHM<br />
76.69 19.17 95.86 • 80% of recurring cost<br />
contribution by NRHM.<br />
Total 86.69 19.17 105.86<br />
• 20% of recurring cost is<br />
contribution by State<br />
Government.<br />
Details of Recurring Cost of Health Advice Call Center (<strong>2012</strong>-<strong>13</strong>)<br />
Rs. in Lakhs<br />
Sr. Particulars Unit Cost No. of Units<br />
1<br />
2<br />
3<br />
HACC Recurring Cost<br />
Service Provider Charges (As per<br />
MOU)<br />
Telephone Expenditure / Outgoing/<br />
SMS Charges etc.<br />
Workshops/Meeting/ IEC/contingency<br />
expenditure<br />
90<br />
Budget<br />
required<br />
79.86 1 79.86<br />
10.00 1 10.00<br />
6 1 6<br />
Total 95.86<br />
SUBSECTION - B.14.4 : NGO PROGRAM : GRANT IN AID TO NGOs<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2007-08 516.5 284.4 247.800<br />
Rs. in Lakhs<br />
Remarks
The Government of Maharashtra is committed to improve the <strong>health</strong> care services for all with<br />
particular focus on women & children living in the un-served and underserved areas in the<br />
districts of the state.<br />
Under National Rural Health Mission, RCH II has taken up steps to achieve objectives with<br />
partnership of non-government organizations, like Mother NGO , Field NGOs ,& Service NGO<br />
under NGO scheme. NGOs are playing a vital role in providing complementary &<br />
supplementary services to Government.<br />
The Service NGO scheme aims at strengthening the role of these NGOs not only in awareness<br />
and demand generation but also the service delivery for contributing towards reduction of<br />
Infant Mortality, Maternal Mortality , and Total Fertility.<br />
Current Status of NGO Scheme<br />
MNGO Scheme:<br />
At present 2 MNGOs are working in two Districts i.e. Nandurbar & Gadchiroli. (Both Districts<br />
are terrain and tribal districts.)<br />
SNGO Scheme<br />
Phase I<br />
Sr.<br />
No.<br />
Present status of SNGO Scheme in Maharashtra:<br />
District covered<br />
No. Of PHCs<br />
covered<br />
No. Of Villages<br />
covered<br />
91<br />
Populations<br />
covered<br />
1 06 22 484 4,95,332<br />
PhaseII<br />
In the year 2011-12, 8 NGOs are select for implementing Service NGO scheme as indicated<br />
below.<br />
Sr.<br />
No.<br />
District covered<br />
No.of PHCs<br />
covered<br />
(Proposed)<br />
No.of Villages<br />
covered<br />
(Proposed)<br />
Populations<br />
covered<br />
(Proposed )<br />
1 08 38 420 6,28,566
Activity Proposed for <strong>2012</strong>-<strong>13</strong><br />
• For Service NGO scheme - Selection of NGOs in most difficult /Tribal areas in Gadchiroli,<br />
Nandurbar, Nashik, Dhule, Bhandara, Gondiya, Chandrapur , Amravati , Beed and Yeotmal<br />
districts.<br />
• External Evaluation – Conduction of external evaluation of those MNGO/SNGOs who have<br />
completed one year in implementation of various programmes under NGO scheme as per<br />
GOI guidelines through external agency.<br />
• Training for NGOs<br />
• Quarterly meeting of NGOs<br />
• Annual Workshop of NGOs<br />
• Monitoring & Evaluation of the project(Internal )<br />
Compliance of remarks of GoI<br />
MNGO Scheme<br />
Underserved areas of the district is identified and MNGO volunteers promote beneficiaries to<br />
get the services from regular <strong>health</strong> service infrastructure. Thus, Field NGOs working under<br />
MNGO take the children and pregnant women to Village <strong>health</strong> Nutrition Day for services.<br />
This scheme is for three years and one MNGO is to be selected per district. This scheme<br />
started in 2007 so the scheme is complete in almost all the districts except 2 districts in the<br />
state.<br />
SNGO Scheme<br />
This scheme is for the area where there is no Government Hospital or available Govt Hospital<br />
is not functioning properly.<br />
Eight such hospitals have been identified in the state. These NGOs are required to conduct<br />
baseline survey first and then start the services. Currently baseline survey is being<br />
implemented.<br />
Budget requirement for <strong>2012</strong>-<strong>13</strong><br />
Table : Budget requirement for NGO Scheme<br />
92<br />
Rs. In Lakhs<br />
Sir Activity Proposed<br />
No.of<br />
Units<br />
Unit cost<br />
Budget<br />
required<br />
1 MNGO SCHEME 2 15 30<br />
2 SNGO SCHEME PHASE- (Existing NGOs) 7 15 105
Sir Activity Proposed<br />
3<br />
SNGO SCHEME PHASE- (New NGOs) Only for<br />
Nandurbar, Gadchiroli, Nashik, Amravati,<br />
Beed, Yavatmal, Chandrapur, Bhandara,<br />
Dhule, Gondia)<br />
No.of<br />
Units<br />
Unit cost<br />
93<br />
Budget<br />
required<br />
10 8.5 85<br />
4 EXTERNAL EVALUATION<br />
TRAINING TO NGOs (before & During the<br />
9 1 9<br />
5 project like Baseline, data software, Writing<br />
project proposal, record keeping etc.)<br />
19 0.2 3.8<br />
6 Quarterly meeting 4 0.4 1.6<br />
7 Annual workshop 1 2 2<br />
8 Monitoring & Evaluation 19 0.6 11.4<br />
Total 247.8
SECTION - B.15 : PLANNING, IMPLEMENTATION AND MONITORING<br />
SUBSECTION - B.15.1 : COMMUNITY BASED PLANNING & MONITORING (CBPM)<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2007-08 292.22 292.1 241.10 234.320<br />
94<br />
Rs. in Lakhs<br />
Remarks<br />
Community based monitoring and planning of <strong>health</strong> services under NRHM is a participatory,<br />
multi-stakeholder process for increasing accountability and responsiveness of public <strong>health</strong><br />
services while improving their implementation. This process was launched at state level in<br />
Maharashtra in mid-2007. After a series of initiation, selection and capacity building<br />
processes at state and district levels, field level implementation started in early 2008. Field<br />
level implementation of Community monitoring in five districts of Maharashtra, initially on a<br />
pilot basis, and then as a component of the State PIP, has now completed four years.<br />
Significant expansion of these activities took place in two further phases, with addition of<br />
new blocks and villages in five districts in mid-2009 and then addition of 8 new districts in<br />
early 2011. Within the state wherever CBM has been implemented, the sense of ownership of<br />
the public <strong>health</strong> services has definitely improved in the community. CBM has ensured<br />
accountability through participatory monitoring and dialogue, has contributed to increasing<br />
utilisation of public <strong>health</strong> facilities, and has induced various improvements in local <strong>health</strong><br />
services. Further since end-2010 Community based planning has also been initiated, wherein<br />
community based processes are now informing local <strong>health</strong> planning, through people’s<br />
participation and decentralised inputs.<br />
With this background, the main focus of Community based monitoring and planning (CBMP)<br />
activities in the period <strong>2012</strong>-<strong>13</strong> would be-<br />
1. Partial phasing out of external inputs, maintenance of core monitoring activities and<br />
development of community based planning in field areas of 5 districts where CBMP<br />
process is being implemented at field level since early 2008.<br />
2. Continuation phase including initiation of community based planning processes in<br />
expanded areas of 5 districts where CBMP process is being implemented since mid-<br />
2009; awareness and dissemination programmes in some additional areas beyond the<br />
existing CBMP areas, in order to widen and expand the scope of Community based<br />
monitoring and planning processes.
3. Completion of one cycle of community monitoring and consolidation of processes in 8<br />
new districts of the State where CBMP activities have started in 2011.<br />
4. Continuation of state level inputs for capacity building, coordination, financial<br />
management, state level events and publication, as well as some wider dissemination<br />
of Community based monitoring and planning process with emphasis on voluntary<br />
activities.<br />
Proposed coverage of community based monitoring and planning activities and plan of<br />
action in the year <strong>2012</strong>-<strong>13</strong><br />
Coordination of state level events, along with training, technical inputs and capacity building<br />
inputs for NGOs at various levels would continue to be managed by SATHI as the existing<br />
State Nodal NGO. Major activities in this year are planned as follows:<br />
1. Partial phasing out of external inputs, maintenance of core monitoring activities and<br />
development of community based planning activities in pilot phase areas of 5<br />
districts<br />
In 5 districts, Community based monitoring and planning process is being implemented in<br />
certain areas since early 2008 where PHCs covered are 39 and under these PHCs total of 195<br />
villages have been covered (this number is slightly lower than the initial 225 villages, since in<br />
two blocks the process has been discontinued due to withdrawal of specific organisations<br />
from these blocks).<br />
The overall strategy would be for partial phasing out of external inputs by civil society<br />
organisations in these areas, with lower scale of inputs but sustaining core community<br />
monitoring activities. The emerging activity of community based planning which was initiated<br />
since 2010 will continue to be developed. Financial inputs for these areas would be reduced<br />
in scale to approximately half of the scale for the previous year (2011-12). The following<br />
activities would be supported in these areas:<br />
o Sustaining core Community monitoring activities with lower scale of external<br />
support- The core community monitoring activities such as meetings of<br />
Community based monitoring and planning committees at different levels,<br />
selective data collection and periodic dialogue between VHSC members and<br />
Health care providers would be continued. These activities would be supported<br />
with lower level of resources given the overall strategy of partial phasing out of<br />
external inputs in these areas. In continuation with data collection during<br />
February- March 2011, the certain Public Hearings in Thane and Pune would be<br />
conducted during April- May <strong>2012</strong>.<br />
o Orientation/training of newly elected PRI members who are part of monitoring<br />
and planning committees at different levels- In the most of existing areas,<br />
elections of PRI members at different levels are taking place, so training and<br />
orientation workshops for newly formed VHSCs as well as elected PRI members at<br />
different levels would be conducted.<br />
95
o Activities for development of community based planning at village, PHC and RH<br />
RKS, and block PIP levels- Based on initial experiences in 2010-11, workshops<br />
would be conducted for RKS members as well as CBMP committees regarding<br />
decentralised planning. The objective of these workshops would be to enable RKS<br />
members to properly understand their role and responsibilities in planning the<br />
appropriate use of various flexible funds at facility level, with a clear focus on<br />
patient welfare and addressing issues identified through the community<br />
monitoring process. Also activities for awareness and capacity building of<br />
community members, VHSC and CBMP committees would be conducted regarding<br />
local <strong>health</strong> planning and giving concrete suggestions for utilization of NRHM<br />
flexible funds.<br />
2. Consolidation of activities in expansion areas of 5 districts where CBMP process is<br />
being implemented since mid-2009<br />
Community based monitoring and planning process has been expanded in 14 blocks of 5<br />
districts since mid-2009. In these areas, total number of PHCs covered is 33 and total of 245<br />
villages as well as 93 Sub-Centers are covered by CBMP. The expansion has been taken place<br />
at different levels, so considering this the following activities would be taken up in these<br />
areas:<br />
2.1 Along with core community monitoring activities, development of community<br />
based planning activities- The core activities such as regular meetings of<br />
monitoring and planning committees, next round of data collection, Jan Sanvad<br />
/Jan Sunwais at different levels would be conducted. Activities like orientation<br />
workshops for RKS committees, awareness and capacity building of community<br />
members, VHSC and CBMP committees about monitoring and suggestions for<br />
utilization of NRHM funds would be conducted in these expansion areas.<br />
2.2 Orientation/training of newly elected PRI members who are part of monitoring<br />
and planning committees at different levels- In the most of the expansion areas,<br />
PRI elections at different levels are taking place hence training as well as<br />
orientation workshops for members of newly formed VHSCs as well as newly<br />
elected PRI members at different levels would be conducted.<br />
2.3 Activities for facilitation of monitoring of Integrated Child Development Scheme<br />
(ICDS) services-In this phase attempt would be to conduct activities for facilitation<br />
of systematic monitoring of ICDS services such as analysis of information at<br />
different levels for identification of issues related to ICDS, dialogue with concerned<br />
ICDS officials at block and district levels. Further towards inter-sectoral convergent<br />
action, visits of VHSC members to block level officials responsible for key <strong>health</strong><br />
related services like ICDS and Water supply would be organised.<br />
2.4 Orientation of broader range of civil society organisations regarding Community<br />
monitoring and planning – District level workshops would be organised with<br />
participationofdiverse civil society organisations active in the district, regarding<br />
community awareness building, collection of information on functioning of <strong>health</strong><br />
96
services, participatory dialogue and intervention in decentralised planning,<br />
enabling more groups to develop community based action to improve <strong>health</strong><br />
services in their respective areas, while working on a voluntary basis. After<br />
sensitization of dozens of new organisations regarding the CBM framework and<br />
process, based on data collection by these organisations, in the coming year<br />
participatory dialogue involving civil society stakeholders and Health providers<br />
would be organized in the Ratnagiri, Latur, Parbhani , Osmanabad, and Solapur<br />
(beyond existing CbM areas for last 2 districts .)<br />
3. Development of Community based monitoring and planning in eight new districts-<br />
In these new districts, the selection and approval of District and Block Nodal NGOs has been<br />
completed and activities have been initiated during 2011. In these eight districts, total<br />
number of PHCs covered are 48 and under each PHC five villages are covered i.e. total of 240<br />
villages. Similar to earlier phase districts, in these districts key monitoring levels would be at<br />
the Village, PHC, Block and District levels.<br />
The following activities would be taken up in these districts and blocks in continuation of<br />
current activities:<br />
3.1 Activities for completion of first round of community monitoring-<br />
In the period 2011-12 in 8 new districts, due to delay in approval of nodal organisations at<br />
official level, only part of the cycle of community monitoring activities could be carried out. In<br />
<strong>2012</strong>-<strong>13</strong>, the plan would be to complete the first round of Community monitoring activities at<br />
different levels including completion of CBMP committee formation, data collection at PHC<br />
and RH levels and Jansunwais / Jansanvad at block and district level. Further the second cycle<br />
of monitoring would be started<br />
3.2 Activities to involve and sensitise additional stakeholders and initiating<br />
Community based planning at village and PHC/RH RKS levels -<br />
Awareness and capacity building workshops would be conducted for different stakeholders<br />
(PRI members, ASHAs), exchange programme would be organised in other districts,<br />
orientation workshops would be held for RKS committee members, awareness and activation<br />
programmes at community level and for members of VHSC and CBMP committees about<br />
monitoring and suggestions for utilization of NRHM funds.<br />
In this phase, taking all districts together, a total of <strong>13</strong> districts, 37 blocks, 120 PHCs and 680<br />
villages would be involved in Community based monitoring and planning activities.<br />
Further in the coming year a round of regional follow up workshops and dialogue events<br />
would be organised in various regions of the state to promote wider awareness and to<br />
encourage voluntary civil society activities for communitisation of <strong>health</strong> services.<br />
4. Budget requirement-<br />
Budget will be required for various CBMP activities focused in <strong>13</strong> districts as follows:<br />
1. Budget for State level coordination and activities<br />
97
Sr.<br />
No.<br />
Table A :- Budget Required for State Level Activities<br />
Rs. in Lakhs<br />
Budget Line items Budget Amount<br />
1 State level Salary and Honorarium 32.98<br />
2 Travel and field Expenses 2.07<br />
3 State level Workshops, Training & Meetings 10.00<br />
4 Office & Communication Expenses 1.20<br />
5 Publications/process documentation 7.0<br />
6 Overheads 6.39<br />
Total 59.64<br />
2. Budget for 5 districts pilot phase areas - partial phasing out of external inputs,<br />
maintenance of core community monitoring and planning activities<br />
Table B :- Budget Required for 5 Districts – pilot phase areas<br />
98<br />
Rs. in Lakhs<br />
Sr. No. Budget Line items Budget Amount<br />
1 Honorarium 6.3<br />
2 Field Expenses 2.1<br />
3 Workshops, Training & Meetings 7.3<br />
4 Facilitation of Data Gathering, preparation of Report<br />
cards<br />
0.11<br />
5 Jan Sanwad / Jan Sunwai 2.57<br />
6 Office & Communication Expenses 0.<strong>13</strong><br />
7 Publication/process documentation 0.21<br />
7 Overheads 2.25<br />
Total 20.96<br />
3. Budget for 5 districts for expansion areas since mid 2009<br />
Table C :- Budget for 5 districts expansion areas<br />
Sr. No. Budget Line items<br />
Rs. In Lakhs<br />
Budget Amount<br />
1 Honorarium 27.54<br />
2 Field Expenses 5.4
3 Workshops, Training & Meetings 16.97<br />
4 Facilitation of Data Gathering, preparation of Report<br />
cards<br />
5 Jan Sanwad / Jan Sunwai 6.86<br />
6 Office & Communication Expenses 0.47<br />
7 Publication/process documentation 0.67<br />
8 Overheads 7.37<br />
Total 64.40<br />
4. Budget for activities in 8 new districts<br />
Table D :- Budget required for 8 new districts<br />
Sr. No. Budget Line items<br />
Rs. In Lakhs<br />
Budget Amount<br />
1 Honorarium 35.52<br />
2 Field Expenses 6.72<br />
3 Workshops, Training & Meetings 11.96<br />
4 Formation/expansion of committees 7.74<br />
5 Office & Communication Expenses 0.29<br />
6 Facilitation of Data Gathering, preparation of Report<br />
cards<br />
3.36<br />
7 Jan Sanwad / Jan Sunwai 9.36<br />
8 Publication/process documentation 0.88<br />
9 Overheads 9.10<br />
Total 84.93<br />
5. Summary of budget requirement<br />
Table D :- Summary of Budget Requirement for CBMP <strong>2012</strong>-<strong>13</strong><br />
Sr. No. Budget Line items<br />
Rs. In Lakhs<br />
Budget Amount<br />
1 Budget for State Level activities<br />
99<br />
3.51<br />
59.64
2 Budget for 5 Districts pilot phase areas 20.96<br />
3 Budget for 5 Districts expansion areas 68.79<br />
4 Budget for 8 new districts<br />
100<br />
84.93<br />
Total 234.32<br />
SUBSECTION - B.15.2 : QUALITY ASSURANCE<br />
Quality Assurance program was initiated in the State during the year 2009-10 with support<br />
from UNFPA. During the first phase 6 districts namely Ahmednagar, Aurangabad, Akola,<br />
Chandrapur, Kolhapur and Raigad were taken. During the 2 nd phase in 2010-11 , 6 additional<br />
districts namely Satara, Jalna, Wardha, Amrawati, Thane and Nashik were taken. During 3 rd<br />
phase in 2011-12 , 6 more districts namely Buldhana, Jalgaon, Bhandara, Osmanabad,<br />
Parbhani and Beed were taken.<br />
The program will continue in year <strong>2012</strong>-<strong>13</strong> in all 18 districts with support from UNFPA. A State<br />
Quality Assurance Cell will be created at State Level.<br />
A) State Quality Assurance Cell :- It will be composed of following persons.<br />
1. State Quality Assurance Nodal Officer<br />
2. Full time Consultant Quality Assurance - (Qualification: Public <strong>health</strong> with 5 years of<br />
experience in MCH)<br />
3. Data entry Operator<br />
A) Budget for State Quality Assurance cell is as follows.:-<br />
Salary :- Salary of State Quality Nodal Officer will be supported by UNFPA. Budget for salary of<br />
other persons is shown in State PIP.<br />
Mobility Support :- One vehicle will be hired @ Rs.25000/- per month for consultants.<br />
Office Expenditure & contingency :- Lump sum amount of Rs.5000/- per month. Thus total<br />
amount of Rs.0.60 Lakhs.<br />
Support for establishing QA Cell :- Lump sum amount of Rs. 1.00 Lakhs is kept for office<br />
equipment and furniture.<br />
Organization of meetings:- Lump sum amount of Rs.50000/- kept.<br />
B) District Quality Assurance Cell :- It is composed of District Quality Assurance<br />
coordinator and Data Entry Operator cum accountant.
Budget for District Quality Assurance Cell is as follows.<br />
Salary :- Salary of District QA coordinators of 12 districts in 1 st and 2 nd Phase for 3 months will<br />
be supported by UNFPA. Budget for remaining 9 months for salary and TA/DA will be from<br />
State Budget in PIP. An amount of Rs. 42.12 Lakhs is kept for this purpose.<br />
Budget for salary & TA/DA of district QA coordinators of remaining 6 districts in 3 rd Phase is<br />
shown in State PIP. An amount of Rs.30.24 Lakhs is kept for this purpose.<br />
Budget for salary of Data Entry Operator cum accountant for 18 districts is shown in State PIP.<br />
An amount of Rs.21.6 Lakhs is kept for this purpose.<br />
Office Expenditure & contingency :- Lump sum amount of Rs.3000/- per month. Thus total<br />
amount of Rs.6.50 Lakhs for 18 districts.<br />
Support for establishing QA Cell :- Lump sum amount of Rs. 0.50 Lakhs is kept for office<br />
equipment and furniture for 18 districts.<br />
Organization of meetings:- Lump sum amount of Rs.5000/- kept for 18 districts.<br />
Detailed budget requirement is mentioned in table below<br />
Table – Budget required for QA Cell<br />
101<br />
Rs. In Lakhs<br />
Sr. No. Activity Unit Cost No of units<br />
Total Budget Rs.<br />
In Lakhs<br />
A State level<br />
State Quality Assurance Nodal<br />
1 Officer (Salary by UNFPA) 6.6 0 0<br />
2<br />
Full time Consultant Quality<br />
Assurance - (Qualification: Public<br />
<strong>health</strong> with 5 years of experience<br />
in MCH)<br />
4.8 1 4.8<br />
3 Data entry Operator 1.2 1 1.2<br />
4<br />
Mobility Support<br />
2.5 1 2.5<br />
5<br />
6<br />
Office expenditure & contingency<br />
Support for establishing QA Cell at<br />
State Level<br />
0.05 12 0.6<br />
1 1 1<br />
7 Organization of meetings 0.5 1 0.5<br />
Total for State Cell 10.6<br />
B District Level<br />
1 District QA Coordinators<br />
0.36 12 38.88<br />
2 (Contractual Position for 12<br />
0.06 6 3.24<br />
3<br />
Districts which were taken up in<br />
2009-10 & 2010-11 )<br />
42.12
Sr. No. Activity Unit Cost No of units<br />
Total Budget Rs.<br />
In Lakhs<br />
4 District QA Coordinators<br />
0.36 6 25.92<br />
5 (Contractual Position for 6 Districts 0.06 6 4.32<br />
6 which were taken up in 2011-12 )<br />
30.24<br />
7<br />
Office expenditure & contingency<br />
0.03 18 6.5<br />
8<br />
9<br />
Support for establishing QA Cell at<br />
district Level<br />
Organization of review meeting at<br />
district level<br />
0.5 18 9.0<br />
0.05 18 0.9<br />
Total of Districts cell 161.1<br />
Total State & District 171.7<br />
SUBSECTION - B.15.3 : MONITORING AND EVALUATION<br />
Compliance of remarks<br />
• State of Maharashtra has already started process of facility based reporting. Two meetings<br />
with GoI are held during March <strong>2012</strong>. It is expected that Maharashtra will start the GoI MIS by<br />
May <strong>2012</strong>.<br />
• Basic data required for GoI MIS facility based reporting is being collected and scruitinised for<br />
each facility in the state.<br />
• Officer at state level identified and name communicated to GoI.<br />
• This year MIS data is used for preparation of PIP. Identification of facilities for IPHS or other<br />
strengthening, identification of delivery points, continuation of schemes, etc are all decided<br />
based on MIS data of the facilities.<br />
• All the meetings mentioned in the proposal are important for monitoring of the program and<br />
providing fresh guidelines and mid time corrections. No. of meetings held in state are as<br />
follows:<br />
• District level meetings of Medical Officers for NRHM activities – 264<br />
• State level monthly meetings held for district level staff – 104<br />
• Special review meetings including meetings of DHO/CS/CEO ZP and senior officers – 103<br />
• Meetings of higher officers (Deputy Directors and above) under Chairmanship of Additional<br />
Chief Secretary (PH & FW) – 27.<br />
• All these meetings proved very important for NRHM as field level difficulties were discussed in<br />
meetings. All the new guidelines were discussed during these meetings and guidelines<br />
changed accordingly.<br />
Monitoring is regular collection, compilation and analysis of selected indicators of various<br />
Programs to enable <strong>health</strong> managers to determine whether key activities are being carried<br />
102
out as per the plan. It is carried out at service delivery unit through direct contact with <strong>health</strong><br />
workers as well as at the managing office by examining periodic reports. Monitoring provides<br />
feedback to project manager in order to improve the operation plan and to take mid-course<br />
corrective measures if necessary.<br />
Evaluation of a program or of a component helps to assess the tracking/success/failure of any<br />
program and also the reasons for the above. It is also necessary task at regular interval for<br />
ongoing projects and at the end of the projects/initiatives and also before up scaling any<br />
program initiative.<br />
ACTIVITY - B.15.3.1 : MONITORING OF NRHM ACTIVITEIS (A+B+C components)<br />
Monitoring and evaluation under <strong>health</strong> department is mainly carried out as follows:<br />
• Regular MIS: The state has well-developed computerised web based system, which<br />
includes all <strong>national</strong> <strong>health</strong> programmes. Fixed date schedule has been prepared for<br />
data entry & feedback is given regularly to all the districts & the programme officers<br />
from the Directorate level. Schedule of MIS and data flow is submitted below.<br />
• Quarterly meetings of senior officers under chairmanship of Add. Chief Secretary at<br />
Regional level.<br />
• The Directorate holds regular annual meetings of all District Health Officers, Civil<br />
Surgeons, Deputy Directors & programme officers & review is taken.<br />
• Monthly meeting of Deputy Directors & Programme officers by the Directorate.<br />
• At various levels like regional & district level concerned officers take regular meetings<br />
for which fixed date schedule has been prepared. Similarly in each PHC monthly<br />
review meetings are organised of all workers & supervisors for which fixed date<br />
calendar has been prepared.<br />
Program Monitoring and Evaluation Framework<br />
The current monitoring system of Public Health Department has a major focus on quantitative<br />
reporting on performance at various levels. This information is generated right from the subcenter<br />
level up to state level. Each bureau/desk receives the information, which is analyzed<br />
and correlated for checking correctness of data and synchronization of events. Annual<br />
surveys are conducted for some items (e.g. eligible couple survey).<br />
The dates of data collection, compilation, analysis and feedback are fixed. Total state report is<br />
ready by 15 th of every month. Level wise MIS collection and dates of information sub<strong>mission</strong><br />
schedule is as follows:<br />
103
Sir Level<br />
Submitting<br />
unit<br />
Table : Flow of HMIS Information<br />
To whom<br />
submitted<br />
1 Facility SC PHC<br />
2 Facility PHC<br />
3 Facility<br />
4 District<br />
5 District<br />
6 District<br />
RH/SDH/WH<br />
/GH/DH<br />
District MIS Cell<br />
(DHO Side)<br />
District MIS Cell<br />
(Civil Surgeon<br />
side)<br />
Reports checked at District MIS<br />
Cell by concerned supervisors<br />
and MIS cell officers<br />
District<br />
HMIS Cell<br />
• Circle MIS<br />
Cell<br />
• Bureaus –<br />
related<br />
reports<br />
• Director<br />
HMIS Cell<br />
• NRHM Cell<br />
MO Meeting is held at District<br />
level by DHO and MS<br />
RH/SDH/GH/WH meeting is<br />
Date of<br />
completion of<br />
activity<br />
Last day of<br />
month<br />
5 th of every<br />
month<br />
5 th of every<br />
month<br />
8 th of every<br />
month<br />
10 th of every<br />
month<br />
11 th of every<br />
month<br />
Remarks<br />
SC ANM and MPW<br />
submit SC report in<br />
prescribed format – on<br />
paper - to PHC on last<br />
day of month in PHC<br />
MIS meeting<br />
Report entered in Web<br />
Based HMIS Software<br />
either at PHC or at<br />
Block Office<br />
Report entered in Web<br />
Based HMIS Software at<br />
RH / SDH / GH / DH<br />
level<br />
Checking the reports,<br />
call back to Facility in<br />
case of errors,<br />
correction of errors.<br />
This starts from 3 rd to<br />
8 th of every month<br />
District MIS report is<br />
made accessible to<br />
Circle offices, related<br />
Bureaus, Director cell<br />
and NRHM cell.<br />
Compilation of reports<br />
is responsibility of the<br />
Director HMIS Cell.<br />
Reports are discussed.<br />
Review of work done<br />
and plan for next<br />
104
Sir Level<br />
7 Circle<br />
8<br />
9<br />
State<br />
level<br />
State<br />
level<br />
Submitting<br />
unit<br />
To whom<br />
submitted<br />
held by Civil Surgeon at District<br />
level<br />
DHO/CS DCP District level<br />
officers meeting at circle level<br />
Meeting of all Program Officers<br />
by concerned bureaus to review<br />
and plan – detailed review<br />
Meeting of all Deputy Directors<br />
and Bureau Chiefs<br />
Date of<br />
completion of<br />
activity<br />
12-<strong>13</strong> of every<br />
month<br />
7 th to 15 th<br />
every month<br />
16 th of every<br />
month<br />
Flow of information of HMIS is as per the figure given below:<br />
SUB CENTER<br />
Figure : Flow of information of HMIS in Maharashtra<br />
PHC RH/SDH/GH/WH<br />
DISTRICT MIS CELL (Health Centers and Hospitals)<br />
Remarks<br />
month is decided.<br />
Circle review and plan<br />
for next month<br />
Program Officers and<br />
supervisors attend<br />
meeting at state level.<br />
This is specific for large<br />
program like ASHA,<br />
IPHS, RKS, School<br />
Health.<br />
Review of work done<br />
and next month<br />
planning.<br />
Attended by Director of<br />
Health Services,<br />
Com<strong>mission</strong>er (FW) &<br />
MD and ACS (PH & FW)<br />
105
Data collected at SC level is in hard copy. HMIS is web based from PHC onwards.<br />
Blue arrow indicate data flow and yellow arrow indicates feedback<br />
In Maharashtra, components of the NRHM are monitored from various bureaus as mentioned<br />
in table AND FIGURE above. These Bureaus are situated at Mumbai and Pune. Therefore each<br />
bureau has separate monitoring unit for its components. Considering this, budget is<br />
separately requested for RCH and FW Bureau as follows:<br />
Plan of implementation <strong>2012</strong>-<strong>13</strong><br />
Following activities are proposed for monitoring and evaluation for year <strong>2012</strong>-<strong>13</strong><br />
1. Strengthening of MIS<br />
All the BPMUs have been provided Computers and contingency to run the computers and<br />
internet under NRHM. Following actions will be taken to strengthen the present MIS system:<br />
• Revision, printing and dissemination of MIS formats consisting of all NRHM indicators<br />
related to VHC, RKS, IPHS, AMG, etc. to VHCs, SHCs, PHCs, RH and all other reporting<br />
units.<br />
• Online/offline entry<br />
DY. DIRECTOR I/C CIRCLE<br />
DHS CELL / DIRECTOR OF HEALTH SERVICES<br />
• Training of at least one member of reporting units in revised MIS formats<br />
• Improving the quality of reporting<br />
NRHM MIS CELL / COMMISSIONER (FW) & MD NRHM<br />
• Monthly Institute wise review of all reporting units.<br />
• Provision of computer and internet services to remaining PHCs, RH and districts.<br />
106
• Establishment of data banks at all the district HQ to fulfill all the needs of district.<br />
• Establishment of M & E Cell at district HQ and State HQ for concurrent monitoring<br />
2. Review Meetings<br />
Review meetings are very important for routine monitoring of the program. Review<br />
meetings supported by good documents on progress of the program are important. During<br />
year 2007-08, review meetings conducted by Additional Chief Secretary (PHD & FW) have<br />
proved to be very effective. Considering this and the experience of these years, review<br />
meetings are proposed & are being taken during year 2008-09 as below:<br />
Table – : Review meetings proposed during 2010-11Rs. In Lakhs<br />
Sir Meeting Frequency<br />
1<br />
2<br />
3<br />
4<br />
5<br />
6<br />
7<br />
DPM/DRCHO review meeting at HQ<br />
by Mission Director<br />
DAM meetings at HQ by Mission<br />
Director<br />
Three meetings of CEO ZP, DHO, and<br />
CS, Deputy Director and Bureau<br />
Chiefs by ACS (PHD) at divisional<br />
headquarters (6 divisions × 3<br />
quarters). Out of these, one will be<br />
planning meeting and other two<br />
review meetings. (Total attendance<br />
is more than 120 persons)<br />
Monthly meetings at district level.<br />
One meeting per month will be<br />
conducted for RCH/NRHM activities<br />
at district level<br />
Subject wise meetings of district<br />
level supervisory staff , state level<br />
officers, etc at divisional, bureau and<br />
state level (ASHA, School Health,<br />
IPHS, RKS, MCTS, JSSK, Sickle Cell,<br />
Telemedicine, etc)<br />
MS RH/SDH and THOs (8 circles × 2<br />
meetings)<br />
Review by Nodal Officers to allotted<br />
Districts – Budget for travel/DA/Stay<br />
of nodal officer<br />
Budget<br />
required<br />
per<br />
meeting<br />
No. of<br />
meetings<br />
107<br />
Budget<br />
required<br />
Monthly 0.9 12 10.8<br />
Monthly 0.5 12 6<br />
Every four<br />
months per<br />
circle<br />
Once month<br />
for all<br />
districts<br />
Monthly and<br />
Bimonthly<br />
4 18 72<br />
0.05 396 19.8<br />
0.5 48 24<br />
Quarterly 1 16 16<br />
One<br />
meeting/<br />
quarterly/dist<br />
0.05 128 6.4
Sir Meeting Frequency<br />
8<br />
Review meetings at <strong>national</strong> level to<br />
be attended by State level officers<br />
Budget<br />
required<br />
per<br />
meeting<br />
No. of<br />
meetings<br />
108<br />
Budget<br />
required<br />
As per need 12 0.5 6<br />
Total 161<br />
3. Staff for Monitoring and Evaluation<br />
Very large data is being collected for RCH and NRHM activities at district level. Various new<br />
schemes are coming up requiring new MIS indicators. Considering this, the MIS system at<br />
state and district level is strengthened with the help of NRHM. One post of Statistical Officer<br />
and 2-3 posts of Statistical Assistants and Statistical Investigators are sanctioned from State<br />
Budget. Considering the quantum of the work increased after introduction of NRHM,<br />
additional posts are sanctioned for M & E.<br />
The Statistical Officer is overall in charge of the District M & E Cell. One person experienced in<br />
HMIS is required to analyze and interpret the data and brief the DHO/CS about situation and<br />
advice corrective measures. For this, one Public Health Specialist is appointed in the state for<br />
every district. Statistical Investigators are appointed in districts depending upon number of<br />
reporting units.<br />
At state level, MIS consultant, Senior M & E Officer, statistical investigators and computer<br />
specialists are appointed.<br />
Considering the remarks for this activity, one Circular is issued to all the districts saying that<br />
regular officer / supervisor should be responsible for each activity under NRHM. Contractual<br />
staff will support the system and not replace or work as independent to regular system. One<br />
workshop of RCH Officer and DPM regarding this is organized in third week of April to work<br />
out details.<br />
This year no new post is requested for M & E. All the posts mentioned are continued since<br />
last 3 years. Details are as follows:<br />
Table – : Staff required for Monitoring and Evaluation – <strong>2012</strong>-<strong>13</strong><br />
Sir Particulars Unit cost<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
A State Level<br />
1<br />
MIS Consultant (Public Health) (Rs.<br />
45000/PM)<br />
5.4 1 5.4<br />
2 M & E Consultant -state level (0.38L/PM) 4.54 1 4.54<br />
3 Sr. M & E Officer (28000/PM) 3.36 1 3.36<br />
4 Stat. Investigator (4) Rs. <strong>13</strong>500/SI/PM 1.62 4 6.48
Sir Particulars Unit cost<br />
No. of<br />
units<br />
109<br />
Budget<br />
required<br />
5 Travel and DA to SPOs 2.5 9 22.5<br />
5 Computer specialists (2) Rs. 27000/PM 3.24 2 6.48<br />
B District Level<br />
3<br />
District /Circle<br />
24000/PM)<br />
M & E Officer (Rs.<br />
2.64 41 108.24<br />
4 TA/DA to M & E Officer 1.2 41 49.2<br />
5 TA to Statistical Officer 1.2 33 39.6<br />
6 Stastical Investigator (2-4/dist) 1.26 98 123.48<br />
Total 369.28<br />
4. Other expenses<br />
Budget is also required for printing of formats, contingency, office expenses, stationary,<br />
equipment and maintenance of website of HMIS. Budget required for these activities is as<br />
follows:<br />
Table – : Other expenses in M & E – <strong>2012</strong>-<strong>13</strong><br />
Sir Particulars Unit cost<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
1 Workshop for revision of MIS formats 0.8 4 3.2<br />
2 Printing of revised formats<br />
I SHC formats (10579 SC × 24 formats) 0.002 10579 21.158<br />
Ii PHC Formats (1816 PHCs × 24 formats) 0.006 1816 10.896<br />
Iii Rural Hospital (455 RH × 24 Formats) 0.003 455 1.365<br />
Iv District Hospital (23 DH × 24 Formats) 0.003 23 0.069<br />
3 Trainings (one day hands on) 0.5 33 16.5<br />
4 Contingency at district level 1.5 33 49.5<br />
5<br />
Contingency at state level (Mumbai +<br />
Pune)<br />
12 2 24<br />
6 Creation and maintenance of Website 15 2 30<br />
Total 156.688<br />
5. Establishment of State Data Health Center<br />
Objectives<br />
1) To maintain programme wise web based/ non-based MIS data.<br />
2) Feedback to state programme officers for data correction/ elimination of errors.<br />
3) To provide outputs / report to State Programme Officers
4) Submit Information at State/ National level as a regular requirement as well as for meetings.<br />
Required Infrastructure<br />
1) Minimum 4000-5000 sq feet office space in a building is required to establish a SHDC,<br />
containing Server room, Computer lab, Office rooms along with Officers cabin, record room,<br />
gents/ladies toilets etc. (Server with specification and supporting system will be design by a<br />
specialist like system analyst)<br />
2) Facilities as a part of building such as Electricity, Fans, lights, electricity back-up etc.<br />
3) Vehicle parking space for staff adjacent to Office.<br />
4) Air-conditioning as per requirement for server room and computer lab.<br />
5) Facilities: Internet / Internet, LAN / WAN, two telephone lines including intercom.<br />
Roll of State Programme Officers<br />
1) Follow up with field officers for online data entry work.<br />
2) Obtain not web-based MIS report from field officers and submit consolidated reports to SHDC.<br />
3) Correspondence for rectification of misleading/ wrong data based on validation output<br />
received from SHDC.<br />
4) Submit data finalization certificate to SHDC on monthly basis.<br />
5) Maintain liaison with SHDC.<br />
Manpower<br />
Sr.<br />
No.<br />
1<br />
Name of Post Qualificati<br />
on<br />
System<br />
Analyst (For a<br />
term of 2<br />
years)<br />
4 Statisticians<br />
BE<br />
(Comp/IT)<br />
with SAP<br />
specializat<br />
ion<br />
M.Sc.(stat<br />
) with<br />
Computer<br />
knowledge<br />
and<br />
experience<br />
in Health<br />
Programm<br />
e<br />
Basic Functions (Job Description)<br />
-Develop and plan hardware<br />
system and software that will be<br />
needed for each National Health<br />
Programmed<br />
-To integrate various software<br />
currently being used for National<br />
Health Programme<br />
-To be responsible for all data<br />
related activities of Data Centre<br />
for various programme at<br />
different levels.<br />
-To access data to be sent to State<br />
Programme Officer the validation.<br />
-Finalization of reports after<br />
corrective measures in validation<br />
errors from State Programme<br />
Officers.<br />
-To provide information/ reports<br />
required at various review<br />
meeting held at State and<br />
National level.<br />
-To maintain liaisons with State<br />
programme officers<br />
No<br />
Required<br />
At<br />
Mumbai<br />
Centre<br />
110<br />
No<br />
Required<br />
At Pune<br />
Centre<br />
Will work for both<br />
the centers at<br />
Mumbai and Pune<br />
2 2
Budget<br />
Sr.<br />
No<br />
A) Salary<br />
Name of<br />
Post<br />
No<br />
Pune<br />
Consolidated<br />
Salary per<br />
month (Rs)<br />
Total<br />
Budget<br />
for a<br />
year<br />
Pune<br />
Centre<br />
No<br />
Mumbai<br />
Consolidated<br />
Salary per<br />
month (Rs)<br />
Total<br />
Budget<br />
for a<br />
year<br />
Mumbai<br />
Centre<br />
(in lakh)<br />
111<br />
Grand<br />
total<br />
1<br />
System<br />
Analyst<br />
1 0.5 5 0 0.5 0<br />
5<br />
2 Statisticians 2 0.2 4 2 0.2 4 8<br />
Total 9 4 <strong>13</strong><br />
B) Allowances to Staff<br />
TA and DA allowances for staff members Pune center Rs. 2.00 lakh, & Mumbai Center Rs. 2.00<br />
lakh.<br />
C) Material and Supplies<br />
Sr.No Item<br />
No.<br />
Pune Centre Mumbai Centre<br />
Unit<br />
Cost /<br />
Unit<br />
(Rs)<br />
Total<br />
Budget<br />
(In<br />
lakh)<br />
No.<br />
Unit<br />
Cost/<br />
Unit<br />
(Rs)<br />
Total<br />
Budget<br />
(In<br />
lakh)<br />
Grand<br />
Total<br />
1<br />
Desktop<br />
computers<br />
10 0.35 3.5 10 0.35 3.5<br />
7<br />
2 Laptops 2 0.4 0.8 2 0.4 0.8 1.6<br />
3<br />
Printer (One BW<br />
one Colour)<br />
2 0.5 1 2 0.5 1<br />
2<br />
4 Scanner (Big) 1 0.7 0.7 1 0.7 0.7 1.4<br />
5<br />
Furniture and<br />
Lan system<br />
1 10 10 1 10 10<br />
20<br />
6<br />
Contingency ,<br />
stationary<br />
Server including<br />
1 6 6 1 6 6<br />
12<br />
6 supportive<br />
1 10 10 1 10 10<br />
software<br />
20<br />
Sub Total of (C) 32 18 27.95 32 64
Total of Data Center<br />
Sir Activity Budget requirement<br />
1 Salary <strong>13</strong><br />
2 Allowances to staff 2<br />
3 Material and supplies 64<br />
Total 79<br />
Total budget requirement<br />
Total budget required for Monitoring and Evaluation is as follows:<br />
Table : Total budget required for Monitoring and Evaluation<br />
Sir Particulars<br />
Rs. In Lakhs<br />
Unit cost<br />
1 Meetings for monitoring of the activities 161<br />
2 Manpower for Monitoring & Evaluation 369.28<br />
3 Other expenses 156.688<br />
4 Establishment of Data Center 79<br />
Total 765.968<br />
ACTIVITY - B.15.3.2 : COMPUTERIZATION OF HMIS, E-GOVERNANCE & E-HEALTH<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2007-08 258.4 220 11<strong>13</strong>.68 11<strong>13</strong>.680<br />
112<br />
Rs. in Lakhs<br />
Remarks<br />
Considering the volume of activities being carried out by Public Health Department, number<br />
of persons involved and amount data generated in system, it has been decided to<br />
computerize all the activities in the state step by step. Ultimate aim of the computerization is<br />
to get real time data for all important indicators and enable the higher level managers to act<br />
upon without any time lag.
Presently, following E-Governance activities are being carried out or in execution stage in the<br />
state<br />
• E-office introduced for the first time in Maharashtra at NRHM Mumbai. It has<br />
started functioning well.<br />
• Biometric attendance system in all <strong>health</strong> offices, PHCs and hospitals. Biometric<br />
system is installed in all the Hospitals. Once it is functional, PHCs will be<br />
introduced in the system.<br />
• Development of ASHA software – ASHA software already developed. Information<br />
of about 60000 ASHA in place. Software has helped to pay compensation to ASHA<br />
in time.<br />
• Hospital MIS software being established in State initially for 23 District Hospitals, 4<br />
General Hospitals and 8 Women Hospitals. This software will completely<br />
computerise the hospital functioning and will improve the efficiency of the system.<br />
• Inventory management - Computerization of Medicine distribution system –<br />
already started and providing good results. Now daily monitoring of all the<br />
important medicines in all <strong>health</strong> facilities of state is possible. This has resulted<br />
into saving of medicines from expiry, calculating correct demand, indications<br />
before the medicine is out of stock.<br />
• Computerization of Medical Equipment inventory – This software is also in<br />
progress and is being prepared with the help of agency appointed by Department<br />
of Information Technology, Govt. of Maharashtra.<br />
• Fund transfer through E-banking to district level – already started in all the<br />
districts, circle offices and training centres.<br />
• Payment of cheques through e-banking – Cheques to venders and other personnel<br />
are now being paid through e-banking.<br />
• Tally ERP-9 Introduced at state, district and block level.<br />
• GIS mapping with the support from UNICEF – GIS maps are being used for decision<br />
making and presentation in the state.<br />
• Use of MCTS software and HMIS software as per GoI guidelines.<br />
• E-transfer – All the request transfers are now online. Officers interested in request<br />
transfer will have to submit their request online to the Government. These<br />
requests will be considered based on need and transfers will be made.<br />
Considering the implementation of all the above mentioned activities in the state following<br />
actions are proposed for year <strong>2012</strong>-<strong>13</strong> :<br />
1. Creation of awareness among <strong>health</strong> officials for E-Governance: All the officers of<br />
Health Department need to know the strengths of E-Governance and advances of<br />
technology available for <strong>health</strong> related monitoring. If they understand the concepts<br />
and benefits of E-Governance, then they will start monitoring from their own.<br />
Considering this, now there is one session of senior IT expert regarding technologies<br />
1<strong>13</strong>
available for <strong>health</strong>. As these sessions are included in regular meetings, no additional<br />
cost is required for this activity.<br />
2. Expansion of E-Office to other State level Offices: E-Office is started in SHS office and<br />
senior officers related to NRHM such as Director of Health Services, Additional Chief<br />
Secretary (PH&FW), etc. The software is from NIC and installation, training,<br />
handholding for one year, maintenance, etc. is being carried out by NIC. One<br />
department of Directorate (Joint Director (Hospitals)) is also included in the scheme.<br />
Now it is proposed to expand this scheme to all the state level offices in Mumbai,<br />
Pune and Nagpur. These offices will require Computers, Scanners, cabling, etc. for<br />
these offices. This is very important for Maharashtra as State level offices in the state<br />
are situated in three different cities and at 8 different places.<br />
3. Establishment and Expansion of Hospital Software : Maharashtra has 455 hospitals<br />
and bed strength of these hospitals ranges from 30 beds to 550 beds. It is proposed to<br />
completely computerise these hospitals in phased manner. Initially all District<br />
Hospitals, all women hospitals and hospitals above 200 beds (General Hospitals) are<br />
being computerised and later on 100 bedded hospitals will be included for<br />
computerisation. The software for computerisation is prepared by Tata Consultancy<br />
Services and will be procured from Maha-online a Government of Maharashtra<br />
company. Budget required for this will be for software, computers, servers and LAN<br />
and also for additional manpower for initial period till the system settles down.<br />
4. Biometric Attendance System : Biometric Attendance System is introduced in the<br />
state. Initially, all the offices from State to District level are covered and then the<br />
Hospitals are covered. Now, it is proposed to cover all the Primary HealthCentres in<br />
the state. This activity is separately mentioned in next chapter.<br />
Budget requirement<br />
As mentioned above, budget is required for procurement of software, hardware and<br />
manpower. Budget required for each of the software system is as follows:<br />
Table – Budget requirement for E-Governance<br />
Sir Particulars Unit rate<br />
No. of<br />
units<br />
114<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
A Expansion of E-Office in State Offices<br />
1 Payment to NIC for software 20 1 20<br />
2 Procurement of Computers 0.4 214 85.6<br />
3 Procurement of Scanners 0.8 36 28.8<br />
4 Lan system 2 8 16<br />
5 Internet connectivity 1.2 6 7.2<br />
6 Computer specialist (one for one building) 2.64 6 15.84<br />
7 Overheads 2 6 12<br />
Total 165.44
Sir Particulars Unit rate<br />
B<br />
Establishment and Expansion of Hospital<br />
Software<br />
No. of<br />
units<br />
115<br />
Budget<br />
required<br />
1 Payment to 'Maha Online for Software 300 1 300<br />
2 Procurement of Computers 0.4 1240 496<br />
4 Lan system 5 23 115<br />
5 Internet connectivity 1.2 23 27.6<br />
6 Manpower 2.64 6 15.84<br />
7 DEO (4/hospital) (92) 1.2 92 110.4<br />
8 Pharmacy Officer (2/Hospital) (46) 1.2 92 110.4<br />
9 Overheads 1 23 23<br />
Total 898.24<br />
C<br />
Other E-projects that will come up during <strong>2012</strong>-<br />
<strong>13</strong><br />
10 5 50<br />
Grand Total 11<strong>13</strong>.68<br />
SUBSECTION - B.15.3.3 : MOTHER AND CHILD TRACKING SYSTEM<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2006-07 0 1963.4 632.354<br />
Rs. in Lakhs<br />
Remarks<br />
As per Govt. of India instructions, Mother and Child Tracking System (MCTS) e-<strong>mission</strong> mode<br />
project under National e-governance plan is being implemented in the State. Exhaustive<br />
attempts are being made to capture the data in MCTS. In Maharashtra, presently, <strong>rural</strong> data is<br />
being captured and uploaded on MCTS web portal. Recently the State has also undertaken<br />
the rash drive to correct the existing data of current year 2011-12 in MCTS. State has further<br />
planned to capture the data from urban area for uploading in MCTS. State, Regional and<br />
District level verification of MCTS Data is the core activity which is being implemented since<br />
last few months. The State has also stressed on real time Data Entry in MCTS software for the<br />
services delivered to beneficiaries. Review meetings are conducted at the State, Regional,<br />
District and Block level regarding the progress of MCTS and utmost importance has been<br />
given to update and validate the records in MCTS. The data of more than <strong>13</strong>.50 lakhs<br />
mothers and 8.50 lakhs children has been captured online on MCTS web portal so far.<br />
Further, the data of 19 thousand ANMs and 59 thousand ASHAs has also been registered as
grass root <strong>health</strong> care providers in MCTS. In order to ensure quality RCH service delivery,<br />
MCTS is the most effective monitoring tool . Keeping in view the wider spectrum of MCTS<br />
activities, it is necessary to strengthen it at all level by providing some sort of support from<br />
NRHM as indicated below:<br />
(1) Printing and supply of MCTS Registers:<br />
As per Govt. of India instructions, it is necessary to provide one RCH register (with Part-A for<br />
eligible couple survey and Part-B for Mother and Child Tracking System) designed by Govt. of<br />
India to each village and <strong>health</strong> facility (excluding Sub-centre) in the State . At present 43722<br />
villages, 1816 PHCs, 367 Rural Hospitals/CHCs (30 bedded), 56 Sub-district hospitals (50<br />
bedded), 24 Sub-district hospitals (100 bedded), 3 General Hospitals (200 bedded), 9 Women<br />
Hospitals, 2 Regional Super Specialty Hospitals and 23 District Hospitals are existing in the<br />
State (Total 46022). In order to provide the RCH Register to all these villages and <strong>health</strong><br />
facilities, a budget of Rs. 115.05 lakhs will be required during <strong>2012</strong>-<strong>13</strong> as indicated below.<br />
Sr. No. Activity<br />
1<br />
Printing and Supply of RCH Registers to each<br />
village and <strong>health</strong> facilities in the State<br />
(2) Support for PHCs for preservation of records:<br />
Unit<br />
cost Rs.<br />
Physical<br />
Target<br />
116<br />
Amount<br />
proposed<br />
Rs. in lakhs<br />
250.00 46022 115.05<br />
Currently five types of work plans are being generated from MCTS web portal out of which<br />
three (ANC, Delivery, PNC) are for mothers and two (Infant Immunization, Child<br />
Immunization) are for children. Each <strong>health</strong> provider and Institution wise work plans are<br />
generated and they should be preserved in respective files. The fundamentals of tracking<br />
basically depend on 18 digit beneficiary ID. Out of which the first <strong>13</strong> digits of MCTS ID<br />
(Separate for Mother and Child) are Unique for every Institution. It is a cumbersome<br />
procedure to write all 18 digits ID on register as well as on beneficiary card by the <strong>health</strong><br />
provider. Hence, it will more appropriate to provide a <strong>13</strong> digits rubber stamp to each ANM so<br />
that they can stamp the MCTS ID Number on Register and Beneficiary card simultaneously.<br />
Considering the drainage workload and catchment area of PHCs it is proposed to provide Rs.<br />
4000/- to each PHC exclusively for providing stationary and <strong>13</strong> digits rubber stamps to the<br />
<strong>health</strong> providers, because, visibility of clear MCTS ID number on the beneficiary cars as well as<br />
in the register will ensure to root the concept of tracking by ID in <strong>health</strong> system. Regarding<br />
the stationary and rubber stamps for other institutions, it is proposed to incur the same from<br />
the contingency available with them. Thus a budget of Rs. 72.64 lakhs (Rs. 4000.00 x 1816<br />
PHCs) is proposed during the year <strong>2012</strong>-<strong>13</strong>.
(3) Strengthening of State MCTS Cell:<br />
Presently the MCTS activities are being monitored through a Cell established at State Family<br />
Welfare Bureau, Pune which is manned by one Medical Officer on deputation basis and<br />
supervised by one Assistant Director (FW). Keeping in view the heavy workload it is proposed<br />
to strengthen the State MCTS Cell by providing following inputs during the year <strong>2012</strong>-<strong>13</strong>.<br />
Sr.<br />
No.<br />
Attribute Number<br />
Monthly<br />
remuneration Rs.<br />
117<br />
Total<br />
amount Rs.<br />
in lakhs<br />
1 Statistical Investigator 2 9,600.00 2.30<br />
2 Data Entry Operator<br />
4 Computers, 2 printers, 4 UPS, 1<br />
2 9,600.00 2.30<br />
3<br />
scanner, 1 laptop, 1 tablet PC,<br />
furniture, utility software and other<br />
contingency.<br />
Hiring of vehicle for monitoring and<br />
Lump sum 10.00<br />
4<br />
supervision activities in the field @<br />
Rs. 25,000/- per month for 12<br />
months.<br />
25,000.00 3.00<br />
Total 17.60<br />
Thus, a budget of Rs. 17.60 lakhs is proposed during <strong>2012</strong>-<strong>13</strong> for this activity.<br />
(4) Training of District staff in MCTS Activities:<br />
MCTS Web Portal is dynamically changing & day to day updates are being incorporated. To<br />
aware the recent changes on MCTS Web Portal to district, block and periphery level officers<br />
as well as data entry operators, MCTS Online Web Portal training is proposed at every DTTC<br />
and HFWTCs as indicated below:<br />
a) Basic training – Basic training of MCTS data entry and operationalization of MCTS web<br />
portal will be imparted to the newly appointed Data Entry Operators. Considering 50<br />
trainee per district, an amount of Rs. 150/- per person is proposed. So the total budget<br />
for basic training will (50 X 33 X Rs. 150) = Rs. 2.47 lakhs.<br />
b) On-going training – To aware new things on MCTS web portal, on-going reorientation<br />
training will be given to the Data Entry operators already appointed. 6 trainings are<br />
proposed during <strong>2012</strong>-<strong>13</strong> considering one training at every two month. Considering 75<br />
participants per district, an amount of Rs. 150 per person is proposed. So total budget for<br />
on-going training will be (75 X33X Rs.150 X6) = Rs. 22.27 lakhs.
c) Hands on Training of all THOs at HFWTCs – Each Circle will conduct one day Hands on<br />
Training of MCTS with GIS of all THOs in HFWTC. The training will be conducted twice in a<br />
year . With 353 THOs and 200 Rs. per participant and 400 Rs per trainer ( two trainers at<br />
each HFWTC) the total budgetary provision for same will be will be ( 353 THOs X Rs.200 X<br />
2 ) + (12 Trainers X Rs.400 x 2) = Rs. 1.50 lakhs. The budget will be distributed to the<br />
HFWTCs.<br />
Thus, a total budget of Rs. 168.16 lakhs ( i + ii (a) (b) & (c) is proposed during <strong>2012</strong>-<strong>13</strong> .<br />
(5) Review of MCH tracking activities<br />
(a) State Level Workshop :-<br />
It is proposed to organize a two days midyear MCTS review workshop. The participants for<br />
this workshop will be the DHOs, Civil Surgeons, Medical Officers of Health of Municipal<br />
Corporations, Municipal Com<strong>mission</strong>ers, Chief Executive Officers of Zilla Parishads, Regional<br />
Deputy Directors and other concerned officers. A budget of Rs. 5.00 lakhs is proposed during<br />
<strong>2012</strong>-<strong>13</strong>.<br />
(b) State Level Meetings:-<br />
As MCTS has been initiated in urban & <strong>rural</strong> area, monthly review meetings of concerned<br />
representatives from urban (MOH) & <strong>rural</strong> (DHO & CS) will be taken. Considering 100<br />
participants (Representatives from DHO + CS + MOH) per meeting , Rs. 100 per participant is<br />
proposed for lunch & Snacks. The total budget requirement for this will be (100 X 100 X 12 ) =<br />
Rs. 1.20 Lacs.<br />
(c) District Level Meeting : -<br />
It is proposed to organize a monthly review meeting at district for review of block MCTS<br />
activities. A budget of Rs. 1000/- per meeting per month is proposed for meeting the<br />
expenses of tea, snacks etc. Thus, a budget of Rs. 12000/- per district will be required during<br />
<strong>2012</strong>-<strong>13</strong>. So for 33 districts, the total budget will be Rs. 3.96 lakhs required. Thus, a budget of<br />
Rs. 3.96 lakhs is proposed during <strong>2012</strong>-<strong>13</strong>.<br />
(d) State Project e-Mission Team (SPeMT) Member meetings:-<br />
As per GOI instructions State Project e-Mission Team (SPeMT) Members should meet at least<br />
once in a month to take review of progress of MCTS in the State. Rs. 1000 per meeting is<br />
proposed as contingency . So total budget for SPeMT member meetings will be 1000 X 12 =<br />
Rs. 0.12 lakhs.<br />
(e) District Project e-Mission Team (DPeMT) Member meetings:-<br />
As per GOI instructions District Project e-Mission Team (DPeMT) Members should meet at<br />
least once in a month to take review of progress of MCTS in the State. Rs. 1000 per meeting is<br />
proposed as contingency. So total budget for DPeMT member meetings will be 1000 X 12 X<br />
33 = Rs. 3.96 Lacs.<br />
Thus, a budget of Rs. 12.75 lakhs (1 to 4) is proposed during <strong>2012</strong>-<strong>13</strong>.<br />
118
(6) Monitoring Data collection & Data Quality<br />
MCTS Data Collection through standard Android Telephony (voice data uploading on web<br />
based central server & data entry by accessing voice data) :<br />
An innovative project has been proposed with technical support from UNICEF & RIDDHI,<br />
Private Software Company for MCTS Data Collection & data entry. In order to implement this<br />
innovative project, it is necessary to have an android based voice data capturing software<br />
preinstalled in GPRS enabled Android Handsets with the ANMs & PHC Medical Officers. The<br />
captured MCTS data will be recorded in preformed voice data format which will be sent<br />
through GPRS to web based central server from which it can be accessed at the data entry<br />
points and MCTS data entry can be done in real time fashion. The PHC level Data for other<br />
Parameters e.g. Daily OPD count, Delivery Count etc. will be sent through GPRS enabled<br />
Android handset available at PHC level. It is, therefore, proposed to provide one GPRS<br />
enabled Android handset to each ANM and MO PHC . The financial implications required for<br />
this purpose are shown as below:<br />
(a) Procurement of Android mobile handset with GPRS connectivity:<br />
Sr.<br />
No.<br />
1<br />
Item<br />
Unit cost<br />
Rs.<br />
Physical<br />
target<br />
119<br />
Total<br />
amount Rs.<br />
in lakhs<br />
Provision of Android Handsets to all tribal<br />
SC and 10% nontribal SC (2055+853=2908)<br />
and all tribal PHCs and 10% of nontribal<br />
PHCs (315+150=465). Total Android phone<br />
requirement is 2908+465=3373<br />
6300.00 3373 212.499<br />
Total 212.499<br />
(b) Training on Android telephony:<br />
i) State level training – Initially it is proposed to train 2 trainers per district at State<br />
level for data uploading through GPRS enabled Android mobile handset. For 33<br />
districts, the total trainees will be 66. A budget of Rs. 1.32 lakhs (Rs. 2000.00 x 66<br />
participants including organization cost) is proposed for this purpose during <strong>2012</strong>-<strong>13</strong>.<br />
ii) Block level training – All ANMs & PHC functionary staff will be trained at block level<br />
training. Expenditure of Rs. 5000 per block is proposed to train and hands on demo for<br />
all ANMs & Medical Officers in Taluka. Hence total budget for same will be 353 x Rs.<br />
5000.00 = Rs. 17.65 lacs.
Thus a total budget provision for Material Procurement & Training in this Standard Android<br />
Telephony innovative for MCTS data capturing will be Rs. 231.469 lacs.<br />
(7) Establishing of State Level MCTS Call Center:<br />
It is proposed to establish a dedicated State level MCTS Call Centre for verification of MCTS<br />
data telephonically from the state level. For this purpose, 5 lady call assistants, 5 telephone<br />
lines, 5 computers with internet connection will be required. The financial implications<br />
required for this purpose will be as follows:<br />
Sr.<br />
No.<br />
Description Number Monthly<br />
remuneration<br />
Rs.<br />
120<br />
Total Amount<br />
Rs. in lakhs<br />
1 Lady Call Assistants 8 9,600.00 7.68<br />
2 5 computers, internet, furniture, and 5<br />
telephone lines<br />
Lump sum 5.00<br />
3 Recurring expenditure Lump sum 2.00<br />
Total 14.68<br />
Thus, a budget of Rs. 14.68 lakhs is proposed during <strong>2012</strong>-<strong>13</strong>.<br />
Sr.<br />
No. Activity<br />
Summary budget<br />
Unit cost<br />
Rs.<br />
Physical<br />
target<br />
Rs. In Lakhs<br />
Amount<br />
proposed<br />
Rs. in lakhs<br />
1 Printing and supply of MCTS registers 0.0025 46022 115.055<br />
2 Support for PHCs for preservation of records 0.04 1816 72.64<br />
3 Strengthening of State MCTS Cell 17.6 1 17.6<br />
4 Training of District Staff 168.16 1 168.16<br />
5 Review of MCH tracking activities 12.75 1 12.75<br />
6 Monitoring Data Collection & Data quality 231.469 1 231.469<br />
8<br />
Establishing of State Level MCTS Call<br />
Centre<br />
14.68 1 14.68<br />
Total 632.354
SUBSECTION – B.15.3.4 : STRENGTHENING OF SUPERVISION AND MONITORING SYSTEM<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2006-07 258.4 220 484.4 484.140<br />
121<br />
Rs. in Lakhs<br />
Remarks<br />
The state has established the Health Management Information system for easy monitoring<br />
and data retrieval. This helps in Monitoring and supportive supervision of <strong>health</strong> institutions.<br />
Such an attempt to automate the records of <strong>health</strong> institutions would help, in the long run, to<br />
reduce the workload of maintaining physical records and in compilation and collation of data<br />
generated. This would also facilitate timely reporting of data as well as analysis and<br />
interpretation of various data generated. In the future, such an initiative can pave way for<br />
attempting emerging trends in medicine like telemedicine.<br />
Support is required to establish and maintain the E-Governance system which is submitted in<br />
this chapter.<br />
Plan of action<br />
It is also proposed to support the program offices directly involved in the NRHM activities. Six<br />
old and three new important Disease Control Programs get funds as per PIP. However some<br />
program offices such as Nursing, Hospitals, Primary <strong>health</strong> institutions actually implement<br />
important activities of program but are not directly provided funds. Therefore it is proposed<br />
to provide funds to these institutions along with the peripheral <strong>health</strong> institutions.<br />
Public Health Department have ambulances and supervisory vehicles. It is proposed to<br />
computerize the total history of all vehicles and improve the proportion of on road vehicle in<br />
the state.<br />
It is also proposed to provide one data entry operator, one accountant and one statistician to<br />
all the disease control program cells to strengthen the management of the programs.<br />
As there will be large scale computerization from State as well as NRHM funds, there is need<br />
off training all the staff of <strong>health</strong> department and also need to develop computer labs at each<br />
district HQ for data entry, checking the entered data, follow up of the data submitted by the<br />
districts and hands on training to supervisory staff of PHCs and CHCs. Therefore it is proposed<br />
to develop one Computer Laboratory for each of the district HQ. The Computer Lab will be<br />
established in one room – preferably the HTT building and if not possible then in DTT building.<br />
This lab will be under control of HMIS Cell of the district.
Budget requirement<br />
Budget is required for establishment of Computer Laboratory, internet facility, salary of<br />
support staff required for supervision provided to the program officers and related facilities<br />
to all the concerned Program Officers at state level.<br />
Budget required for this purpose is as follows:<br />
Table – : Budget requirement for strengthening MIS and supervision<br />
Rs. In Lakhs<br />
Sir Particulars Unit cost<br />
1<br />
2<br />
Replacement of old computers and maintenance<br />
of existing computers in all the State level<br />
offices<br />
Establishment of Data Bank for online HMIS in<br />
District<br />
No. of<br />
units<br />
122<br />
Budget<br />
required<br />
12 8 96<br />
i Procurement of Computers (6 per district) 0.3 198 59.4<br />
ii<br />
Procurement of Heavy Duty Printers (2 per<br />
district)<br />
0.3 66 19.8<br />
iii LAN System 2 33 66<br />
iv Civil Works 5 33 165<br />
3<br />
Provision of one DEO, one accountant and one<br />
statistician to collect and compile program data<br />
to 6 program offices + one accountant for<br />
payment of meetings at SHS (19 persons)<br />
1.26 19 23.94<br />
4 Support to program offices 6 8 48<br />
5 Support to MIS section of Directorate 6 1 6<br />
Total 484.14
SUBSECTION - B.15.3.5 : ESTABLISHMENT AND FUNCTIONING OF GRIEVANCE CELLS<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2010-11 27.81 38.4 42.84 42.840<br />
123<br />
Rs. in Lakhs<br />
Remarks<br />
Many times complain are received by SHS and districts regarding various shortfalls in<br />
activities implemented under NRHM. Presently, these complain are entertained by concerned<br />
officers and dispatched to concerned districts for further action.<br />
Considering the importance of grievance redressal, one grievance cell at SHS Mumbai and one<br />
each at Deputy Director Circle HQ have been established in 2010-11. These cells will continue<br />
to work during the year <strong>2012</strong>-<strong>13</strong>.<br />
Composition of the cell at Deputy Director i/c circle office will be as follows:<br />
• Deputy Director i/c circle or his representative<br />
• One NGO representative, preferably the CBM NGO of the city<br />
• One retired judge or senior journalist of the city<br />
This committee meets once a week. One person is appointed from Social Work or Journalism<br />
background full time to coordinate the mattes. He/She will register the complaint, get the<br />
information collected from concerned department and inform the complainant.<br />
Non-official members will be paid Rs. 500/visit + local travel charges.<br />
Compliance of remarks on grievance Cell is as follows:<br />
• During the year 2011-12, Grevence cell received total 291 complaints. All these complaints<br />
were processed. Out of these, action completed in <strong>13</strong>1 complaints and action in process in<br />
160 complaints.<br />
• Lot of complaints are received regarding grievances against regular staff. Such complaints are<br />
tracked till enquiry is made and enquiry report is sent to DHS for further action. Enquiry has<br />
been started against <strong>13</strong> officers due to constant follow up of the Grevence Cell.<br />
• Currently, grievance Cell is also entrusted responsibility of tracking the news appear in local<br />
newspapers.<br />
• Telephone charges are doubled due to increase in follow up of the complaints to district and<br />
state HQ. This is good indication.
Budget requirement<br />
Budget required for grievance cell is for telephone and Grievance Redressal Officer. Budget<br />
will be required to one state cell and one cell each for 8 circle offices in state. Total budget<br />
required is as follows:<br />
Table - : Budget requirement for grievance cell<br />
Sir Activity Unit cost<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
1 Telephone charges 0.48 9 4.32<br />
2 Salary of GR Officer 2.4 9 21.6<br />
3 Salary of DEO to GR Officer at state 1.26 2 2.52<br />
3 TA/DA to nonofficial members 1.2 8 9.6<br />
4 Contingency 0.6 8 4.8<br />
Total 42.84<br />
124
SECTION - B.16 : PROCUREMENT<br />
Procurement procedure inn Maharashtra is transparent. Procedures adopted by Maharashtra<br />
are as follows:<br />
Procurement methods<br />
Procurement in Maharashtra takes place by following methods<br />
1. Medicine Procurement from State Government Budget and from activities under<br />
Mission Flexi pool through State Government Rate Contact. From April <strong>2012</strong>, this<br />
purchase will be made through Open Tender System (Two envelop system).<br />
2. Medicine procurement where there is no RC through tender system (two envelop<br />
system).<br />
3. Medicine procurement from RCH funds and from DCP funds through one tender<br />
system only by following World Bank procurement procedure.<br />
4. There are no rate contracts for equipment. Therefore equipment are procured<br />
through only open tender system. For State and MFP funds 2 envelop system is used<br />
and for RCH and for RCH and DCP funds World Bank Procurement Procedure (one<br />
envelop) system is used.<br />
5. Computers, printers and UPS procured either through DGS & D RC or State DIT RC<br />
whichever is cheaper for required specification computer.<br />
6. Furniture and some selected item procurement through Government Rates fixed by<br />
Industries Department in concurrence with Finance Department of Government of<br />
Maharashtra.<br />
Procurement agency<br />
As per NRHM Guidelines, Maharashtra has established one dedicated Procurement Cell in the<br />
state. This cell is headed by officer at the level of Joint Director. He/she is supported by<br />
Deputy Director (Procurement) and two Assistant Directors of procurement. This cell is<br />
supported by contractual technical staff paid from NRHM funds.<br />
Tender system<br />
E-tendering system is used for all the tenders. Instrument/equipment are tested by expert<br />
panel usually from senior Professors from Government Medical Colleges from Mumbai, Pune<br />
and Aurangabad. Laboratory tests, chemical tests are performed in accredited laboratories<br />
wherever necessary.<br />
Approval of tenders<br />
• Firstly approval for procurement of goods is given. For this, demand for particular<br />
item, budget provision, specifications and which method of procurement is being used<br />
is checked and approval is given.<br />
125
• Once the tender process is completed and financial bids are opened, total record is<br />
submitted to Committee under Chairmanship of ACS (PH & FW). Members of<br />
committee include Secretary (Finance), Secretary (Industries) and CSPO. Joint Director<br />
(Proc) is member secretary of committee. Procurement order is given only after the<br />
approval of committee.<br />
• Payment is made only after getting original receipts from the consignee. No advance is<br />
paid if not mentioning in Tender.<br />
Funds for procurement of medicines<br />
Source of funds for medicines with approximate budget are mentioned below:<br />
1. State government funds for PHCs and SCs – Rs. 32 Crores<br />
2. State Government funds for Hospitals – 57 Crores<br />
3. State Government funds for DCPs – 14 Crores.<br />
4. GoI funds for RCH activities – Rs. 70 Crores<br />
5. GoI funds for PHCs and Hospital under IPHS – 19 Crores.<br />
Total funds availability – GoM funds Rs. 103 Crores + GoI funds Rs. 89 Crores = total Rs. 192<br />
Crores.<br />
Above figures do not include the medicines particularly Anti-snake venom, Anti rabies vaccine<br />
and emergency medicine through Cess Funds of Zilla Parishads as these figures are not<br />
collected at state level.<br />
Procurement for year <strong>2012</strong>-<strong>13</strong><br />
In order to provide quality RCH services, it is necessary to ensure the availability of essential<br />
drugs and equipment at all <strong>health</strong> facilitates. Following equipment, drugs and supplies are<br />
proposed under Maternal Health, Child Health and Family Planning during <strong>2012</strong>-<strong>13</strong>.<br />
Sl. No. Activity<br />
Unit cost<br />
Rs. in<br />
lakhs<br />
Physical<br />
targets<br />
126<br />
Amount<br />
Proposed<br />
Rs. in<br />
lakhs<br />
B 16.1 Procurement of Equipment<br />
B 16.1.1 Procurement of equipment : MH<br />
Operationalize Comprehensive Abortion<br />
1 Care services (including MVA / EVA<br />
and Medical Abortion) at <strong>health</strong> Center<br />
64.38<br />
Sub-total for Maternal Health 64.38<br />
B 16.1.2 Procurement of equipment : CH<br />
1<br />
Mannequin (Baby Model for NSSK<br />
training)<br />
0.060 208 12.50<br />
2<br />
Kelly Forceps for PPIUCD for District<br />
and Women Hospitals (3 sets for each<br />
0.0045 93 0.42
Sl. No. Activity<br />
Unit cost<br />
Rs. in<br />
lakhs<br />
Physical<br />
targets<br />
127<br />
Amount<br />
Proposed<br />
Rs. in<br />
lakhs<br />
institute)<br />
Sub-total for Child Health 12.92<br />
B 16.1.3 Procurement of equipment : FP<br />
1<br />
NSV kit (@ 10 kits per district &<br />
corporation)<br />
0.03375 560 18.90<br />
2 Printing of R3(6000) & R4(6000) registers 0.00150 12000 18.00<br />
Sub-total for Family Planning 36.90<br />
B 16.1.4 Procurement of equipment : IMEP 0 0 0<br />
B 16.1.5 Procurement of others<br />
Support for ARSH Counselors at District<br />
1<br />
HQ- Procurement of 1 Computer with<br />
printer, scanner & UPS at 33 District HQ<br />
ARSH Clinics @ Rs. 50000/- per clinic<br />
Printing of 400 Training modules for<br />
0.50 33 16.50<br />
2 Medical Officers of newly selected blocks<br />
for CBA activities under ARSH<br />
Printing of 1600 Training modules for<br />
0.001 400 0.40<br />
3 ANMs/LHVs of newly selected blocks<br />
for CBA activities under ARSH<br />
Printing of 5250 Training modules for<br />
0.0005 1600 0.80<br />
4<br />
ASHAs & 5250 training modules for<br />
AWWs of newly selected blocks for CBA<br />
activities under ARSH<br />
Printing of new record keeping registers<br />
0.0003 10500 3.15<br />
5<br />
and formats, Stock keeping, Outreach<br />
activity registers as provided by GoI @<br />
Rs. 2000/- per clinic (140 ARSH Clinics)<br />
Register & format for 850 ANMs to be<br />
0.02 140 2.80<br />
6 continued in 222 Municipal Council area<br />
@ Rs. 500 per ANM (Municipal Councils)<br />
0.01 850 4.25<br />
Sub-total for Other(ARSH & URBAN)<br />
School Health<br />
Purchase of Height & weight<br />
27.90<br />
7 measurement scale for calculation of BMI<br />
at state level<br />
0.03 440 <strong>13</strong>.20<br />
8 Software for Database at state level 20.00 1.00 20.00<br />
9 Laptop Purchase 0.35 853 298.55<br />
Sub-total School Health 331.75<br />
Total for equipment (B 16.1) 473.85<br />
B 16.2 Procurement of Drugs and supplies<br />
B 16.2.1 Drugs & supplies for Maternal Health<br />
1 Sub-center Kit-A (Rural) 0.11 10579 1163.69<br />
2 Sub-center Kit-B (Rural) 0.07 10579 740.53
Sl. No. Activity<br />
3<br />
4<br />
5<br />
6<br />
7<br />
8<br />
Essential Obstetric Care drug kit for<br />
PHCs<br />
SBA drug kit for PHCs (658 – 24x7<br />
PHCs/54 PHCs in HFD<br />
SBA drug kit for CHC/FRU (369 CHCs,<br />
74 SDH) (In HFD 50)<br />
SBA drug kit for DH/WH/OH (23 DH, 9<br />
WH, 4 OH) (In HFD 3)<br />
Emergency Obstetric Care drug kit for<br />
FRUs (184 CHC FRU, 23 DH, 9 WH, 4<br />
OH= 220 ) (in HFD 21)<br />
Sub-center kit –A+B (Urban ) 112 Health<br />
Posts) (Municipal Corporations)<br />
Unit cost<br />
Rs. in<br />
lakhs<br />
Physical<br />
targets<br />
128<br />
Amount<br />
Proposed<br />
Rs. in<br />
lakhs<br />
0.21 1816 381.36<br />
0.24 658 157.92<br />
0.24 443 106.32<br />
0.24 36 8.64<br />
1.50 220 330.00<br />
0.18 112 20.16<br />
9 SBA kit for Maternity Homes (Urban) 0.24 64 15.36<br />
10<br />
Emergency Obstetric Care Drug Kit for<br />
Maternity Homes (Urban)<br />
1.50 64 96.00<br />
11<br />
SBA drug kit for DH/WH/OH (23 DH, 9<br />
WH, 3 OH)<br />
Drug kit for RTI/STI (Kit-1) ( for 658-<br />
0.24 35 8.40<br />
12 24X7 PHC & 456 CHC/SDH/WH (54<br />
PHC/50 CHC in HFD)<br />
Drug kits for RTI/STI (Kit 2) ( for 658<br />
0.00025 25208 6.30<br />
<strong>13</strong> 24X7 PHC & 456 CHC/SDH/WH (54<br />
PHC/50 CHC in HFD)<br />
Drug kits for RTI/STI (Kit 3) ( for 658<br />
0.00010 66728 6.67<br />
14 24X7 PHC & 456 CHC/SDH/WH (54<br />
PHC/50 CHC in HFD)<br />
Drug kits for RTI/STI (Kit 4) ( for 658<br />
0.00032 14828 4.74<br />
15 24X7 PHC & 456 CHC/SDH/WH (54<br />
PHC/50 CHC in HFD)<br />
Drug kits for RTI/STI (Kit 5) ( for 658<br />
0.00040 2966 1.19<br />
16 24X7 PHC & 456 CHC/SDH/WH (54<br />
PHC/50 CHC in HFD)<br />
Drug kits for RTI/STI (Kit 6) (For 658<br />
0.00030 7414 2.22<br />
17 24X7 PHC & 456 CHC/SDH/WH (54<br />
PHC/50 CHC in HFD)<br />
Drug kits for RTI/STI (Kit 7) ( for 658<br />
0.00049 29657 14.53<br />
18 24X7 PHC & 456 CHC/SDH/WH (54<br />
PHC/50 CHC<br />
RPR test kits ( for 658 24X7 PHC & 456<br />
0.00049 1483 0.73<br />
19 CHC/SDH/WH (54 PHC/50 CHC in<br />
HFD)<br />
RTI-STI- drug kits for link workers<br />
0.00060 12677 7.61<br />
20 Drug kits for RTI/STI (Kit 1) 0.00025 16296 4.07<br />
21 Drug kits for RTI/STI (Kit 2) 0.00010 43140 4.31
Sl. No. Activity<br />
Unit cost<br />
Rs. in<br />
lakhs<br />
Physical<br />
targets<br />
129<br />
Amount<br />
Proposed<br />
Rs. in<br />
lakhs<br />
22 Drug kits for RTI/STI (Kit 3) 0.00032 <strong>13</strong>899 4.45<br />
23 Drug kits for RTI/STI (Kit 4) 0.00040 479 0.19<br />
24 Drug kits for RTI/STI (Kit 5) 0.00030 19024 5.71<br />
25 Drug kits for RTI/STI (Kit 6) 0.00049 1984 0.97<br />
26 Drug kits for RTI/STI (Kit 7)<br />
HIV whole blood test kits 6<strong>13</strong>000 kits for<br />
0.00049 1984 0.97<br />
27<br />
estimated 6<strong>13</strong>000 ANCs in districts. Total<br />
no. of kits 76680 for 69710 ANCs from<br />
HFD<br />
Supply of safe delivery kits 7275 kits for<br />
estimated 1455 HIV positive del. in PHC<br />
0.00025 674300 168.58<br />
28 & in case of HFDs 486 safe del. Kits<br />
required for estimated 97 HIV positive<br />
del. In PHCs.<br />
Printing of consent forms & laboratory<br />
0.0025 7275 18.19<br />
29<br />
forms each for testing of pregnant<br />
mothers estimated no. 6<strong>13</strong>000 @ Rs.70/for<br />
100 forms<br />
Treatment of Severally anemic mothers<br />
0.00070 674300 4.72<br />
30 by Parental Iron treatment to pregnant<br />
mothers<br />
0.005 16912 84.56<br />
31<br />
Supply of Sanitary Napkins to JSY<br />
beneficiaries in Rural Institutions<br />
0.0005 340647 170.30<br />
32<br />
Operationalise Comprehensive Abortion<br />
Care services MMA drug kits<br />
0.00088 31719 27.91<br />
Sub-total for Maternal Health (1 to 33) 3567.30<br />
B 16.2.2 Drugs & supplies for Child Health<br />
Drug kit for Sick New Born and<br />
1 Child/Neonatal Resuscitation for all<br />
PHCs<br />
Emergency drug kit for New Born and<br />
2<br />
Child for 24x7 PHCs<br />
Drug kit for Sick New Born and Child for<br />
3<br />
FRU/CHCs<br />
Emergency drug kit for newborn and<br />
4<br />
child for FRUs<br />
Drug kit for Sick newborn and child for<br />
5<br />
DH, WH and GH.<br />
Emergency drug kit for newborn and<br />
6<br />
child for DH, WH & GH<br />
Drug kit for sick newborn and<br />
7 child/neonatal resuscitation for Urban<br />
Health Posts<br />
Drugs required for mass De-worming<br />
8<br />
and Vitamin A supplementation<br />
0.047 1816 85.40<br />
0.081 658 53.30<br />
0.041 220 9.02<br />
0.183 220 40.26<br />
0.083 34 2.81<br />
0.337 34 11.45<br />
0.047 218 10.25<br />
- - 330.00
Sl. No. Activity<br />
Unit cost<br />
Rs. in<br />
lakhs<br />
Physical<br />
targets<br />
<strong>13</strong>0<br />
Amount<br />
Proposed<br />
Rs. in<br />
lakhs<br />
Sub-total for Child Health ( 1 to 8) 542.49<br />
B 16.2.3 Drugs & supplies for Family Planning<br />
1 Inj. Lignocain 1% 30 ml vial Rs. 16.00 <strong>13</strong>7500 22.00<br />
2 Inj. Pentazocin 1ml Amp Rs. 3.55 387500 <strong>13</strong>.75<br />
3 Chromic Catgut 10 (box of 10 pieces) Rs. 300.00 8250 24.75<br />
4 Autoclave Strips (boxes) Rs.459.00 10000 4.59<br />
Sub-total for Family Planning (1 to 4) 65.09<br />
B 16.2.4 Supplies for IMEP<br />
General drugs and supplies for <strong>health</strong><br />
B 16.2.5 facilities<br />
1<br />
2<br />
3<br />
4<br />
5<br />
Procurement of iron folic acid tablets for<br />
adolescent boys and girls & School<br />
teachers, AWWs (No. of beneficiaries,<br />
*52, + 20 percent of it , *0.60 paise)<br />
Procurement of Albendazole tablets for<br />
adolescent boys and girls<br />
(No. of beneficiaries* 2, + 10 percent of it<br />
*0.60 paise)<br />
Procurement of Sub-center Kit A @ Rs.<br />
11000 for 59 HP & Kit B @ Rs. 7000 for 59<br />
HP total of Rs. 18000 per HP (Municipal<br />
Councils)<br />
Procurement of Kit A & B for 850 Urban<br />
ANMs<br />
Sub-total for general drugs (ARSH &<br />
URBAN)<br />
School Health medicine Purchase at State<br />
Level<br />
0.000006 9707038 1837.99<br />
0.000006 9707038 128.<strong>13</strong><br />
0.18 59 10.62<br />
0.18 850 15.30<br />
1992.04<br />
0.83 440 365.20<br />
Total for drugs and supplies (B16.2) 6532.12<br />
Grand total (B16.1 + B16.2) 7005.97<br />
Summary Table Procurement RCH<br />
Sr.No. Activity Budget Rs. Lakhs<br />
B 16.1 Procurement of Equipment
Sr.No. Activity Budget Rs. Lakhs<br />
1 Maternal Health 64.38<br />
2 Child Health 12.92<br />
3 Family Planning 36.90<br />
4 ARSH & URBAN 27.90<br />
5 School Health 331.75<br />
Sub Total Procurement of Equipment 473.85<br />
B 16.2 Procurement of Drugs and supplies<br />
1 Maternal Health 3567.30<br />
2 Child Health 542.49<br />
3 Family Planning 65.09<br />
4 ARSH & URBAN 1992.04<br />
5 School Health 365.20<br />
Sub Total Procurement of Drugs and supplies 6532.12<br />
Total RCH Procurement 7005.97<br />
SECTION - B.17 : PNDT ACTIVITIES<br />
(Covered under Component A – RCH Flexipool)<br />
<strong>13</strong>1
SECTION - B.18 : REGIONAL DRUG WAREHOUSE<br />
SUBSECTION - B.18.1 : STATE PROCUREMENT MANAGEMENT<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2007-08 <strong>13</strong>21.2 599.6 783.12 783.720<br />
<strong>13</strong>2<br />
Rs. in Lakhs<br />
Remarks<br />
Timely supply of good quality drugs as well as logistics management is of critical importance<br />
in any <strong>health</strong> system. Maharashtra state is completely reorganizing the procurement set up<br />
within the state and is in process of revision of existing procurement policy.<br />
Procurement strengthening plan f – <strong>2012</strong>-<strong>13</strong><br />
Salient features of the procurement of goods and services in state are as follows:<br />
• Currently medicine and equipment are partly procured at state and partly at district<br />
level. As Procurement Division of the state is now fully functional all the purchases in<br />
<strong>2012</strong>-<strong>13</strong> will be by Procurement Division of the state.<br />
• E-tendering software and Inventory control software is introduced in the state. This<br />
has enabled to get precise information about stock situation of every drug and<br />
equipment and also in procurement.<br />
• Demand generation, distribution of drugs and stock position is completely<br />
computerized. Data entry is made at PHC level onwards.<br />
• Medicines purchased will be stored in Regional and District warehouses. Therefore 8<br />
warehouses at regional level and 33 warehouses at district level will be strengthened.<br />
• Currently there are two warehouses in each district. One for DHO (for PHCs) and one<br />
for CS (for DH and CHCs). Now onwards, only one warehouse will be constructed in<br />
District Hospital premises. This will save in manpower and security requirements and<br />
will be easy for monitoring.<br />
• All the Pharmacies in Public Health Department offices are now connected by web for<br />
inventory control. This system will be strengthened further.<br />
• Medicines will be purchased by E-tender system only.<br />
• Medicines required in very small quantity and of minimal cost (requirement less than<br />
Rs. 1000/institute in year) and medicines of short expiry (e.g. adrenaline) will only be<br />
purchased locally. All other medicines will be purchased from central level.<br />
• State level Procurement Cell, Regional and district stores, etc. will be supported under<br />
NRHM.
• Daily stock of important medicines is being monitored in the state.<br />
• One Procurement Verification Officer is appointed since 2009-10. This person visits all<br />
the stores at Districts and major blocks and verifies the stock register, assures whether<br />
the stock book is maintained, all NRHM purchases are entered in registers, etc.<br />
Budget requirement – 2011-12<br />
Budget requested in this PIP is for currently functioning system, i.e. for divisional and district<br />
warehouses. Considering the above plan, budget required for procurement plan of<br />
Maharashtra state is as given below:<br />
Table - : Procurement Plan of Maharashtra state : 2011-12<br />
Sr Particulars Unit cost<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
A State Level Activities<br />
Sr. Procurement Consultant (Medical<br />
1<br />
Postgraduate with at least 3 years experience in<br />
Procurement and trained at reputed agency in<br />
World Bank Procurement Procedure)<br />
Procurement Consultant (Pharmacy postgraduate<br />
5 1 5<br />
2<br />
with at least 3 years experience in procurement<br />
and Trained at reputed agency in World Bank<br />
Procurement procedure)<br />
Salary of Procurement Officer (medicines (2),<br />
3.6 1 3.6<br />
1 Equipment (2) and Other goods (1) at state<br />
procurement cell<br />
3.4 5 17<br />
2<br />
Salary of procurement assistant /Pharmacist at<br />
state procurement cell (6)<br />
1.26 8 10.08<br />
3 Quality Assurance Officer 2.6 1 2.6<br />
5 Contingency to Procurement Cell 15 1 15<br />
6<br />
Travel and Daily allowances to State Procurement<br />
Officers for pre-dispatch inspection and meetings<br />
20 1 20<br />
B Circle and District Level activities<br />
1<br />
Repairs and new construction of Circle<br />
warehouses<br />
12 8 96<br />
2<br />
Repairs and new construction of District<br />
Warehouses<br />
<strong>13</strong> 33 429<br />
3 Pharmacist to DHO/CS and Circle warehouses 1.26 74 93.24<br />
4 Contingency to circle and district warehouses 1.2 74 88.8<br />
5 Procurement Verification Officer (Rs. 25000/PM) 3.4 1 3.4<br />
Total 783.72<br />
<strong>13</strong>3
SECTION - B.19 : NEW INITIATIVES / STRATEGIC INTERVENTIONS / PROJECTS<br />
SUBSECTION - B.19.1 : MEDICAL SERVICE BACKUP FOR PALKHI SESSIONS<br />
(PUNE, SATARA AND SOLAPUR DISTRICTS)<br />
Activity deleted as per decision<br />
SUBSECTION - B.19.2 : BIOMETRIC ATTENDANCE FOR HEALTH STAFF<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2010-11 201.88 632.52 550.12 397.120<br />
<strong>13</strong>4<br />
Rs. in Lakhs<br />
Remarks<br />
Presence of <strong>health</strong> staff is important to provide <strong>health</strong> services. Many times serious patients<br />
get delayed treatment because concerned staff is not available. Therefore, it is essential to<br />
monitor the arrival and leaving of <strong>health</strong> staff in hospitals/PHCs and concerned<br />
establishments. Three districts in Maharashtra, Thane, Akola and Wardha have implemented<br />
biometric attendance system on pilot basis. Attendance and timeliness of <strong>health</strong> staff in these<br />
districts have improved significantly. Based on experience of these districts, it is proposed to<br />
extent this scheme to all the PHCs, RHs and District Hospitals of the state.<br />
Salient features of the scheme will be as follows:<br />
• Biometric attendance is being installed in all the offices and <strong>health</strong> facilities except<br />
THO office and PHCs this year. These places will be covered in 2011-12.<br />
• The staff including senior officers will be required to put thumb impression on the<br />
device at the time of arrival and at the time of leaving the hospital. The device will<br />
keep record of arrival and departure.<br />
• The biometric device will be connected online with central server at district level and<br />
state level.<br />
• District information will be available on line to CEO ZP, DHO and Civil Surgeon at<br />
district level and Director of Health services and ACS (PH & FW) at state level.<br />
• Special efforts with the help of experts will be made in PHCs where there is no<br />
internet connection available for submitting information. These PHCs are not more<br />
than 10% in state.<br />
• Central server for HMIS will be sued for this purpose.<br />
Compliance of remarks
• Biometric Attendance system is being used for basically two types of staff. One is office staff<br />
having fixed duty hours from 9.45 AM to 5.30 PM and <strong>health</strong> facility staff having changing<br />
duty system.<br />
• Regarding office staff, the system has started showing results within one month. As this<br />
system records impression of fingers, the person has to come to office in time. This is now<br />
being linked to salary software from 1.4.<strong>2012</strong>. After that every absentee will be treated as<br />
LWP unless certified by controlling officer.<br />
• Regarding clinical staff like doctors, nurses and support staff who have changing duties, there<br />
is some problem at operational level particularly in bigger hospitals. These problems are being<br />
sorted out with the help of IT experts.<br />
• Total data of the district is received at district, regional and state HQ. This data is reviewed.<br />
Even senior officers are called by Hon. ACS (PH) for their explanation if they are consistently<br />
late to office.<br />
• Except at 2 places in the state, the machine was well accepted by staff. No mischief was done<br />
bt staff to make the machine out of order.<br />
• We expect that because of timekeeping by doctors and nurses, accessibility will be improved<br />
which will finally improve quality of <strong>health</strong> care delivery. However, till today no systematic<br />
study is done for this.<br />
• For year <strong>2012</strong>-<strong>13</strong>, the expansion will be in PHC where problem of regular attendance is much<br />
more serious.<br />
Considering above fact, it is proposed to approve this scheme.<br />
Budget requirement<br />
Budget will be required for following purposes<br />
• Biometric device<br />
• Staff for monitoring<br />
Computers and internet facility is already available in PHC and all hospitals, therefore there is<br />
no request for budget for these items.<br />
Detailed budget requirement is as follows:<br />
Table -: Budget required for biometric attendance in <strong>health</strong> institutions<br />
Sr Activity Unit cost<br />
No.of<br />
units<br />
<strong>13</strong>5<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
1 Biometric equipment in PHCs and THO offices 0.3 1246 373.8<br />
2 One Computer Manager at DHS 3 1 3<br />
3 Computer Assistants one in each circle and 4 at DHS 1.26 12 15.12<br />
4 Contingency, internet stationary at circle HQ 0.5 8 4<br />
6 Contingency at state HQ 1.2 1 1.2<br />
Total 397.12
SUBSECTION - B.19.3 : PREVENTION OF SICKLE CELL DISEASE<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2010-11 1698.47 1914.33 1815.26 1815.250<br />
<strong>13</strong>6<br />
Rs. in Lakhs<br />
Remarks<br />
Sickle Cell Disease (SCD) is a hereditary disorder mostly found in tribal communities,<br />
scheduled castes & other backward communities. Prevalence is more in malaria prone areas.<br />
Although it is observed throughout the state, some of the geographical areas have high<br />
prevalence rate of carriers which is more than 8% and sufferers are found to be more than<br />
0.5%. According to various studies, 19 districts in Maharashtra are found to be high prevalent<br />
districts. These include Thane, Nashik, Nandurbar, Amaravati, Gondia, Gadchiroli, Nagpur,<br />
Chandrapur, Wardha, Bhandara, Yavatmal, Dhule, Nanded, Jalgaon, Washim, Akola,<br />
Aurangabad, Buldhana, Raigad & Hingoli is added as few patients are found there also.<br />
The disease is hereditary & there is no cure for the disease. SCD is one of the major<br />
reasons of recurrent episodes of infection, malnutrition and death in young children in high<br />
prevalence areas. Identification of carriers & sufferers is necessary in all high-risk districts<br />
giving emphasis on <strong>health</strong> education and marriage counseling. Therefore prevention &<br />
control program for SCD is implemented in all tribal & high prevalent districts.<br />
1. Objectives of the program<br />
Objectives of Sickle Cell Disease Control Program are as follows:<br />
• To create awareness in the community about the disease, diagnostic services,<br />
management & other aspects of SCA.<br />
• To identify carriers and counsel them for prevention of Sickle cell disease in next<br />
generation.<br />
• To improve the awareness of the government functionaries in these areas.<br />
• To establish laboratory facility for screening the disease at PHC& laboratory facilities<br />
for screening & conformation at RH, SDH & DH.<br />
• To make available treatment at various levels from PHC to DH.<br />
2. Progress during 2011 - 12<br />
Progress of SCD Program in state during year 2011-12 is as follows:<br />
• SCD Program is being implemented in 19 districts.<br />
• Training of <strong>health</strong> staff and laboratory technicians is completed in 19 districts.
• Solubility testing started in all the PHCs included in project. 73 Electrophoresis test<br />
centers are established in 19 districts.<br />
• Distribution of cards based on status of individual started in all project districts.<br />
• Marriage counseling started in all districts.<br />
• MIS in place for all project districts.<br />
• Procurement of solubility test kits for all project districts and electrophoresis machines<br />
for new districts.<br />
• NGOs selected and started working in 10 high prevalence districts under this project.<br />
• ASHA and Health workers like ANM, HA, MPW are involved in 9 districts having low<br />
prevalence of Sickle Cell Disease.<br />
• Capacity of RH/SDH improved to treat complicated cases.<br />
• 73 Electrophoresis testing centers are established.<br />
• Quality Control in screening test (Solubility test) and Electrophoresis test is monitored<br />
stringently.<br />
• Day care centers are established in <strong>13</strong> District Hospitals and 2 Women Hospitals.<br />
Year wise Physical Performance<br />
Physical Progress<br />
Year Total test performed Total Disease Total Carrier<br />
2007-08 15310 - -<br />
2008-09 68590 - -<br />
2009-10 421246 1120 11275<br />
2010-11 1181862 3191 24984<br />
April 2011 to<br />
January <strong>2012</strong><br />
2559863 28<strong>13</strong> 31656<br />
Total 4246871 7124 67915<br />
<strong>13</strong>7
Role of Government Medical Colleges<br />
• 8 Medical Colleges are identified in the project areas.<br />
• Each Medical Colleges is attached to two-three districts.<br />
• Each district is attached to the nearest medical college.<br />
• Medical colleges are helping in routine electrophoresis testing as well as<br />
training of medical officers & Lab Technicians.<br />
• Medical Colleges are also supporting for treating the complicated cases &<br />
providing specialized treatment like Hip replacement, Neonatal screening,<br />
Prenatal screening.<br />
• Role of Medical Colleges will be expanded for quality control in Sickle Cell<br />
testing.<br />
• Medical Colleges will routinely examine 5% of negative & positive samples<br />
quarterly.<br />
• They will also inspect the Electrophoresis centers in their districts at least once<br />
in a year.<br />
3. Plan of action <strong>2012</strong>-<strong>13</strong><br />
• Extinction of Sickle Cell Disease Control Program to a new districts i.e. Hingoli.<br />
• More focus on Quality Control issues.<br />
• Testing, card distribution and Marriage counseling of all boys and girls above<br />
15 years age in <strong>rural</strong> areas of project districts.<br />
• Liaison with Medical Colleges for training, research, treatment of complicated<br />
cases & quality control of Sickle Cell tests.<br />
• More emphasis on IEC with implementation of Sickle Cell Week in December.<br />
• Strengthen the Day Care Centre.<br />
• Establish well equipped Lab at District Hospital and Women Hospital.<br />
• Arrange regular camps for Sufferer patients.<br />
• ASHA sensitization work shop.<br />
• NGO evaluation.<br />
Health institutes involved in SCD Control Program during year <strong>2012</strong>-<strong>13</strong> are as follows:<br />
Table - : Institutes involved in SCD Control Program<br />
Sir Type of institutions Total in state<br />
No. included in<br />
SCD program<br />
1 PHC 1809 947<br />
2 RH/SDH 474 240<br />
<strong>13</strong>8
Sir Type of institutions Total in state<br />
No. included in<br />
SCD program<br />
3 District Hospitals 23 14<br />
4 Woman Hospital 10 4<br />
5 Medical Colleges 16 8<br />
Total 2332 12<strong>13</strong><br />
4. Budget requirement for year <strong>2012</strong>-<strong>13</strong><br />
Budget will be required for following activities:<br />
a. Peripheral <strong>health</strong> institutions<br />
Patients will come to peripheral <strong>health</strong> institutions for laboratory investigations and<br />
treatment. Medicines and equipment will be purchased at state level therefore not<br />
mentioned for peripheral <strong>health</strong> institutions.<br />
Table –: Budget required for peripheral <strong>health</strong> institutions<br />
Rs. In Lakhs<br />
Sir Particulars Unit cost<br />
No. of<br />
units<br />
<strong>13</strong>9<br />
Budget<br />
required<br />
1<br />
Laboratory consumables & Medicine to<br />
PHCs 0.15 947 140.85<br />
2<br />
Lab Consumables & Medicine<br />
Electrophoresis testing centre<br />
to<br />
0.15 75 11.25<br />
3 Lab consumables & Medicine to RH/SDH 0.05 165 08.25<br />
4 Contingency to PHC 0.10 947 94.70<br />
5<br />
Contingency to Electrophoresis testing<br />
centre 0.10 75 07.50<br />
6 Contingency to RH/SDH 0.10 165 16.50<br />
7 Contingency to Block level 0.10 209 20.90<br />
Total 299.95<br />
NGO Districts.<br />
Almost all people with Sickle Cell anemia have painful carises at some point in<br />
their lives. Some have a crisis less than once a year. Others may have fifteen or more<br />
crises in a year. Some of the complications of Sickle Cell Anemia are Splenic<br />
(Sequestration) Crisis, and Infections like Pneumonia, Meningitis, influenza, and<br />
hepatitis, Acute Chest Syndrome, Delayed Growth and Puberty in Children, Stroke, Eye<br />
Problems, Gallstones, Pulmonary Arterial Hypertension (High Blood Pressure) and<br />
Multiple Organ Failure.
Therefore the only alternative to control the diseases is frequent counseling<br />
for regular treatment to prevent crisis and counseling for marriage to prevent<br />
trans<strong>mission</strong> of gene to next generation which is the prime role of NGO.<br />
The Physical Performance of NGO districts.<br />
Sr.<br />
No.<br />
District<br />
Total<br />
Solubility<br />
Test<br />
performed<br />
Total IEC<br />
Done<br />
Total<br />
Carrier<br />
Total<br />
Sufferer<br />
1 Thane 463884 5563950 2848 235<br />
2 Nashik 300465 1864278 1146 30<br />
3 Nandurbar 601867 4447773 20993 1955<br />
4 Gondia 287901 739504 2142 396<br />
5 Gadchiroli 331238 382775 5958 1047<br />
6 Nagpur 308477 104743 2507 285<br />
7 Wardha 207749 842787 3081 250<br />
8 Chandrapur 317254 879574 6838 1095<br />
9 Bhandara 222567 2469205 4833 200<br />
10 Yavatmal 402049 1003785 <strong>13</strong>969 767<br />
11 Dhule 216292 118876 <strong>13</strong>84 606<br />
Total 3659743 18417250 65699 6866<br />
Considering high no. of Carrier and Sufferers in these districts it is very<br />
important to follow up these Carriers and Sufferers for regular treatment (monthly<br />
basis), frequent prenatal counseling, and early diagnosis and to adapt Healthy habits<br />
to prevent crisis etc.<br />
As the only way to prevent disease is only counseling Considering all above<br />
factor the NGO's were appointed in these high prevalence’s, tribal and LEA districts<br />
like Gadchiroli, Chandrapur, Gondia, Bhandara etc.<br />
Role of NGO in Sickle Cell Program<br />
To Create Awareness about Sickle Cell Disease in community.<br />
To prepare IEC in local language and distribute.<br />
Arrange meetings and testing camps in villages, Schools, Colleges and Ashram Schools<br />
etc.<br />
To motivate community for Solubility test.<br />
To distribute color coded cards after testing. (Red-Sufferer, Yellow-Carrier, White-<br />
Negative)<br />
To register Sickle cell Sufferer and Carrier.<br />
Home visits to Carriers for premarital counseling.<br />
Home Visits to Sufferers for regular treatment.<br />
140
To Counsel Sickle Cell Sufferer and Carrier (Sufferers to be counseled for regular<br />
treatment on monthly basis Premarital Counseling of Carriers and relatives every 2<br />
months.)<br />
To Counsel Pregnant mother for early registration and prenatal diagnosis.<br />
No. of NGO's appointed:-<br />
(Thane, Nashik, Nandurbar, Gondia, Gadchiroli, Nagpur, Chandrapur, Bhandara, Wardha,<br />
Yavatmal, Dhule district)<br />
Sr.<br />
No.<br />
1<br />
2<br />
Sr. Districts No. of NGO's<br />
appointed<br />
1 Thane 1<br />
2 Nashik 1<br />
3 Nandurbar 1<br />
4 Gondia 1<br />
Remarks<br />
5 Gadchiroli 2 As this is a total tribal high<br />
focus and LEA district<br />
6 Nagpur 1<br />
7 Wardha 1<br />
8 Bhandara 1<br />
9 Chandrapur 1<br />
10 Yavatmal 2 It is big, tribal district having<br />
16 blocks.<br />
11 Dhule 1<br />
Total <strong>13</strong><br />
NGO selections:<br />
On an average one NGO is selected per district by District Health Society depending<br />
upon the size of district.<br />
NGO are appointed by giving advertisement in local newspaper.<br />
JAT and TAC committees are formulated to scrutinizes to applications<br />
Budget for NGO (Total budget for <strong>13</strong> NGOs)<br />
NGO districts - Grant in AID to NGOs<br />
NGO districts - Grant in AID to NGOs Place of work No. of<br />
Unit<br />
Salary of Project Manager (Rs.9000+1000<br />
TA/DA) Rs. 10000*12 m)<br />
Salary of DEO cum Accountant (Rs.6000*12<br />
m)<br />
District Head<br />
quarter<br />
District Head<br />
quarter<br />
141<br />
Unit<br />
Cost<br />
Total<br />
<strong>13</strong> 1.20 14.10<br />
<strong>13</strong> 0.72 8.46
3<br />
4<br />
Salary and TA/DA of NGO Supervisor<br />
(Rs.7000+1500 TA/DA)Rs.8500*12 m *Block)<br />
Salary and TA/DA of Community Volunteer<br />
(Rs. 4000 + 500 TA/DA) Rs.4500*12* m)<br />
Block Head<br />
quarter<br />
PHC Head<br />
quarter<br />
109 1.02 104.38<br />
518 0.54 260.37<br />
7 MIS and TA/DA (Rs.10000) - <strong>13</strong> 0.10 1.30<br />
8 Overheads (Rs.3000*per PHC) - 518 0.03 15.54<br />
9<br />
IEC (Rs.5000*per PHC)(This budget is<br />
calculated in District level budget)<br />
NGO districts - Grant Total<br />
Role and responsibility of human resource provided to NGO.<br />
- 518 0.05 25.90<br />
• Role of PHC volunteer (Salary and TA/DA of Community Volunteer Rs.4500/- pm)<br />
1. Selected NGO has one community volunteer for each PHC.<br />
2. They create awareness of disease in the PHC area.<br />
3. These volunteers visits households and schools and motivate target population to get<br />
tested for Sickle Cell Disease.<br />
4. Tested persons are issued cards (White-normal, Yellow-Carrier and Red-Affected) by<br />
NGO after counseling.<br />
5. All Carriers and affected persons are registered at PHC, and counseled periodically for<br />
marriage and treatment by NGO volunteers.<br />
6. They give home visit to each Sufferer every month and Carriers every two months.<br />
7. Frequent visit to pregnant mothers.<br />
• Role of Taluka supervisor (Salary and TA/DA of Taluka Supervisor Rs.8500/- pm)<br />
1. Taluka Supervisor appointed at block level. He monitor 5/6 PHC in his each block.<br />
2. To monitor Electrophoresis centre in that Taluka.<br />
3. To plan the testing camps at village, schools and sub center level along with PHC, MO.<br />
4. He/She monitors availability of Cards, IEC materials, other consumables etc in all<br />
PHC’s in the block.<br />
5. He/She supervises the testing camps in the blocks.<br />
6. He/She ensures that all positive blood samples are sent to electrophoresis centers.<br />
7. He/She supervises white, yellow, red cards are distributed as per electrophoresis test<br />
results.<br />
8. He/She supervises for all Sufferer and Carrier are counseled for regular treatment and<br />
pre marriage counseling.<br />
9. He/She send Sickle Cell patients to speciality centers.<br />
10. He/She monitors training of PHC volunteers.<br />
• Role of Project Manager (Salary and TA/DA of Project Manager Rs. 10000/- pm)<br />
1. Project Manager appointed at district level. He/She monitor to each district.<br />
2. To monitor Electrophoresis centre, in district.<br />
3. He/She Collect and compiled data and send it to State level.<br />
142<br />
404.15
4. He/She monitors availability of Cards, IEC materials, other consumables etc. in all<br />
block’s He/She supervises the testing camps in the blocks.<br />
5. He/She ensures that all positive blood samples are sent to electrophoresis centers.<br />
6. He/She supervises white, yellow, red cards are distributed as per electrophoresis test<br />
results.<br />
7. He/She ensures that all Sufferer and Carrier are counseled for regular treatment and<br />
pre marriage counseling.<br />
8. He/She monitors training of all volunteers and block supervisors.<br />
9. Coordinate with district administration for training, funding and reporting.<br />
10. Attend monitoring meetings at PHC and State level.<br />
• Role of Data entry operator cum Accountant (Salary of DEO cum Accountant<br />
Rs.6000/- pm)<br />
1. To maintain the book of accounts.<br />
2. To maintain the vouchers, purchase bills.<br />
3. To maintain records all PHC level volunteers and block level supervisors.<br />
4. To compile data and prepare reports and submitted to district as well as State.<br />
5. To prepare line list of Sufferers and Carriers.<br />
b. NGO District level budget<br />
Sickle cell disease control program will be monitored from district level. The NGO supervision<br />
will also be done from district level. Budget required at district level include NGO charges, IEC,<br />
District Cell budget and contingency.<br />
Detailed budget requirement is shown in table below:<br />
Table: District level budget requirement for NGO districts<br />
Rs. In Lakhs<br />
Sir Particulars<br />
1<br />
2<br />
Unit<br />
cost<br />
No. of<br />
units<br />
143<br />
Budget<br />
required<br />
NGO involvement (Institutes covered in<br />
dist.) 0.8472 477 404.15<br />
Salary & TA, DA of Lab Technician in<br />
Electrophoresis testing centre 1.2 40 49.20<br />
3 Salary & TA, DA of SCD Coordinator<br />
Salary of Lab Tech. in DH/WH (Day Care<br />
1.86 10 20.46<br />
4 Centre)<br />
Salary of Counselor in District Hospital<br />
0.54 10 5.40<br />
5 (Day Care Centre)<br />
Lab Technicians for Peripheral institute<br />
0.60 10 6.00<br />
6 (PHC) 0.78 9 7.02<br />
7 Contingency to District 1 11 11.00<br />
8 Support to DH/WH (Lab consumables 1.50 10 15.00
Sir Particulars<br />
9<br />
10<br />
&Contingency/renovation of day care<br />
room )<br />
Unit<br />
cost<br />
No. of<br />
units<br />
144<br />
Budget<br />
required<br />
Procurement of test kits (Solubility &<br />
Electro & Medicine) 2 11 22.00<br />
Celebration of Sickle Cell Week in<br />
PHC/RH/SDH/DH/WH 0.042 661 27.87<br />
11 Health Camp for Sufferer 0.05 418 20.90<br />
Consumables to HPLC machine<br />
12 (Nandurbar, Wardha, Gadchiroli) 5 3 15.00<br />
<strong>13</strong> IEC (per PHC/RH/SDH/DH/WH) 0.05 477 33.05<br />
Total 637.05<br />
* Gadchiroli, Gondia and chandrapur districts are high prevalence for Sickle Cell Disease. They<br />
are also high focus LEA tribal population majority districts. The Model in these districts may<br />
change from NGO to additional support staff like one Taluka supervisor per two talukas and<br />
one lab. Technician and one volunteer per 4 to 5 PHCs depending upon the district demand.<br />
Non-NGO’s Districts<br />
(District covered Amravati, Jalgaon, Nanded, Washim, Akola, Bhuldhana, Aurangabad, Raigad<br />
and Hingoli)<br />
As these are low prevalence districts it was decided to implement program through<br />
existing <strong>health</strong> infrastructure by giving remuneration to them. Decision to implement Sickle<br />
Cell Disease Control Program either through NGOs or ASHA and Health functionaries is taken<br />
at State Health Society.<br />
ASHA’s are trained for community mobilization and creating awareness regarding<br />
Sickle Cell Disease. ANM/MPW is trained for basic Solubility testing and collecting samples for<br />
Electrophoresis during camp. HA from PHC will help in transporting Solubility test kits,<br />
sending samples for Electrophoresis and collecting reports of Electrophoresis testing. Record<br />
will be kept by ASHA, ANM and HA at sub center and PHC respectively.<br />
The Physical Performance of NGO districts.<br />
Sr.<br />
No.<br />
District<br />
Total Solubility<br />
Test performed<br />
1 Amravati <strong>13</strong>5318<br />
Total IEC Done Total Carrier<br />
399369<br />
Total<br />
Sufferer<br />
<strong>13</strong>42 166<br />
2 Jalgaon 147082 442427 239 16<br />
3 Nanded 34806 1244<strong>13</strong> 29 4<br />
4 Washim 49556 42402 99 12<br />
5 Akola 81962 22210 385 37
6 Buldana 42500 758697 105 16<br />
7 Aurangabad 67243 75738 2 4<br />
8 Raigad 28661 51770 15 3<br />
9 Hingoli Proposed in <strong>2012</strong>-<strong>13</strong><br />
Total 587128 1917026 2216 258<br />
Role of Health functionaries in Non-NGO's districts:<br />
• ASHA Compensation (Per test Rs. 5/-, Card distribution Rs. 20/-, Village<br />
meeting Rs.50/-, Group meeting Rs. 40/-, Follow up of patients Rs. 15/-)<br />
ASHA is trained for Sickle Cell Disease and is utilized for community<br />
mobilization for testing and creating awareness.<br />
ASHA is trained for distribution of Colour coded cards and counselling for<br />
marriage and regular treatment.<br />
ASHA gives home visits to Carriers and Sufferer for pre-marital counselling and<br />
follow up for regular treatment in order to prevent crisis.<br />
They arrange meeting with Self Health Group, adolescent’s age group<br />
minimum 6 meeting in a year and Gram sabha 4 in a year for giving<br />
information to community.<br />
Visit Sickle Cell pregnant mother for early registration and prenatal diagnosis<br />
counselling.<br />
ASHA ensures that the total population in her jurisdiction will get information<br />
on Sickle Cell.<br />
• ANM Remuneration (Per test Rs. 4/-, blood samples collection and Counseling<br />
Rs. 40/-,<br />
On Arogya Seva Satra day ANM will perform testing on patients mobilized by<br />
ASHA (minimum 25 patients per satra) after Quality Control of test kits.<br />
ANM will keep record of all tested for Solubility test and those who are found<br />
positive<br />
ANM will be help ASHA in distributing white cards.<br />
ANM will collect blood samples of all positive Solubility samples and 3%<br />
Negative samples.<br />
ANM will keep record of tests performed during satra and samples sent for<br />
Electrophoresis.<br />
She will keep follow up of samples sent to Electrophoresis centre.<br />
She will counsel the Sufferer and Carrier and distributes cards.<br />
She will visit Sufferer and Carrier in her sub centre area.<br />
• Health Assistant. (Transport of sample to PHC Rs.50/-, Transporting sample to<br />
Electrophoresis center Rs. 200/-, Monitoring at PHC level Rs. 100/- pm)<br />
HA will transport Solubility kits, Consumables and EDTA bulbs required for<br />
Sickle Cell testing from PHC to Arogya Seva Satra.<br />
HA will bring back samples of positive Solubility test and 3% Negative samples<br />
for Electrophoresis to PHC.<br />
145
Sr.<br />
No.<br />
1<br />
2<br />
3<br />
4<br />
5<br />
He will transport positive Solubility test samples from PHC to Electrophoresis<br />
testing centers and bring back the report of Electrophoresis.<br />
He will keep record of all Electrophoresis samples, Carriers and Sufferers.<br />
He will be responsible for reporting to THO.<br />
He will help the Medical Officers from PHC to examine each Sufferer once in a<br />
month and Carrier in marriage age group once in 6 months.<br />
The block Sickle Cell assistant will supervise all these activities and will be<br />
responsible for collecting data from PHC and submitting to Sickle Cell<br />
Coordinator. He should remain present for each Arogya Seva Satra.<br />
Health workers districts budget<br />
Non NGO districts<br />
ASHA Remuneration<br />
Non NGO districts<br />
Test compensation to ASHA<br />
(Rs.5/test)(Rs. 300*per ASHA)<br />
Monthly meetings with adolescents<br />
(Rs.240*per ASHA) (6 meeting in year)<br />
Gram Sabha<br />
Rs.50 for 4 sessions(Rs200*per ASHA)<br />
Card distribution<br />
(Rs.20*per ASHA)<br />
Follow up visits<br />
(Rs.15*per ASHA*3 m)<br />
Remuneration to ANM/HA<br />
No.<br />
of<br />
Unit<br />
Unit<br />
Cost<br />
146<br />
Total<br />
ASHA 14263 0.00300 42.79<br />
ASHA 14263 0.00240 34.23<br />
ASHA 14263 0.00200 28.53<br />
ASHA 14263 0.00020 2.85<br />
ASHA 14263 0.00045 6.42<br />
6 Testing for ANM Rs.4/test(Rs.240*ASHA) ASHA 14263 0.00240 34.23<br />
7<br />
Councelling and collection of sample (ANM)<br />
(Rs.40*ASHA)<br />
ASHA 14263 0.00040 5.71<br />
8<br />
9<br />
10<br />
Transport of sample to PHC (HA)<br />
(Rs.100*ASHA)<br />
Transporting sample to Electrophoresis center<br />
(per PHC*2000)<br />
Incentive to HA/LHV for monitoring<br />
(per PHC*1200)<br />
Non-NGO districts - Grant Total<br />
ASHA 14263 0.00100 14.26<br />
PHC 429 0.02000 08.58<br />
PHC 429 0.01200 5.00<br />
182.60
Sir Particulars<br />
Table - Non-NGO District level budget<br />
Unit<br />
cost<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget required<br />
1 Involvement of ASHA district 0.41534 470 182.60<br />
2<br />
Salary & TA, DA of Lab Technician in<br />
Electrophoresis testing centre 1.2 35 39.48<br />
3 Salary & TA, DA of SCD Coordinator 1.86 9 15.75<br />
4 Salary of Taluka Sickle Cell Assistant 0.90 105 99.03<br />
6<br />
Salary of Lab Tech. in DH/ WH (Day Care<br />
Centre) 0.54 8 4.32<br />
7<br />
Salary of Counselor in District Hospital<br />
(Day Care Centre) 0.60 8 4.80<br />
8 Contingency to District 1 9 8.50<br />
Support to DH/WH (Lab consumables &<br />
Contingency/renovation of day care<br />
9 room )<br />
Procurement of test kits (Solubility &<br />
1.50 8 11.00<br />
11 Electro & Medicine)<br />
Celebration of Sickle Cell Week in<br />
2 9 17.00<br />
12 PHC/RH/SDH/DH/WH 0.042 544 22.91<br />
<strong>13</strong> Health Camp for Sufferer 0.05 22 1.10<br />
14 ASHA Sensitization (1 camp in year) 0.001 14263 14.26<br />
15 IEC (per PHC/RH/SDH/DH/WH) 0.05 544 27.20<br />
c .State level<br />
Total 447.95<br />
SCD program implementation will be controlled from state level. Important activity to be<br />
done from state level is provision of Solubility & Electrophoresis test kits & Electrophoresis<br />
Machine to districts. Trainings will be carried out by regional training centers. Budget for<br />
training will be covered in training budget. Budget required for remaining activities at state<br />
level is as follows:<br />
Table: - Budget required at state level<br />
Sir Particulars Unit cost<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget required<br />
1<br />
Equipment (Electro., Centrifuge, HPLC<br />
machine), consumables 35 2 70.00<br />
2 IEC & Evaluation of NGO state level - - 119.30<br />
147
Sir Particulars Unit cost<br />
No. of<br />
units<br />
Budget required<br />
3<br />
Solubility test kit, Electrophoresis test kits<br />
& Consumables 0.08 1250 100.00<br />
4 Salary of Quality Control Officer 5.40 1 5.40<br />
5 Salary of Program Officer 3.445 2 6.89<br />
6 Salary of Program Assistant 1.36 2 2.71<br />
7 Contingency at state level 2 1 2.00<br />
9 State level Sickle Cell Week 0.01415 1414 20.00<br />
10<br />
Training for L.T., ANM, MPW, LHV, S.N &<br />
ASHA etc. in districts. 2 20 40.00<br />
11 Support to GMC 8 8 64.00<br />
Total 430.30<br />
a. Summary of SCDCP requirement<br />
Total requirement of SCD Control Program is mentioned in table below:<br />
Table- : Summary of Budget Requirement – SCD Program<br />
Rs. In Lakhs<br />
Sir Level Budget required<br />
1 Peripheral Health Institutions 299.95<br />
2 District level budget for NGO district 637.05<br />
3 District level budget for Non-NGO district 447.95<br />
4 State level budget requirement 430.30<br />
Total 1815.25<br />
SUBSECTION - B.19.4 : TELEMEDICINE PROJECT<br />
Year of<br />
starting the<br />
scheme/<br />
initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed for<br />
PIP <strong>2012</strong>-<strong>13</strong><br />
Budget<br />
proposed<br />
to NPCC<br />
2007-08 340.02 328.72 328.720<br />
Remarks<br />
148<br />
Rs. in Lakhs<br />
Installation of Telemedicine<br />
equipment in DH/SDH,<br />
Specialist facilities and no.<br />
of patients increased with<br />
Multivideo Conferencing<br />
Equipment.
Telemedicine is a rapidly developing application of clinical medicine where medical<br />
information is transferred via telephone, Internet or other networks for the purpose of<br />
consulting, and sometimes remote medical procedures or examinations. Telemedicine may<br />
be as simple as two <strong>health</strong> professionals discussing a case over the telephone, or as complex<br />
as using satellite technology,Internet with Static IP and video-conferencing equipment to<br />
conduct a real-time consultation between medical specialists in two different places.<br />
Telemedicine Centers in Maharashtra<br />
In Maharashtra, all the 23 District Hospitals, 4 Sub-District Hospitals are connected with<br />
telemedicine network since 2009-10. During 2010-11, telemedicine facility is extended to 30<br />
SDH/RH (one per district except Mumbai). These facilities are called patient node. Thus,<br />
currently there are 27 + 30 = 57 patient nodes in the state. These nodes seek expert services<br />
from 6 specialty nodes, out of which 3 are situated in Mumbai, and one each at Pune,<br />
Aurangabad and Nagpur.<br />
Plan of action for year <strong>2012</strong>-<strong>13</strong><br />
During year <strong>2012</strong>-<strong>13</strong>, new tele-opthalmaolgy telemedicine center will be opened. Existing<br />
centers will be strengthened and their utilization will be improved. Following actions are<br />
proposed during <strong>2012</strong>-<strong>13</strong>.<br />
• Further strengthening the existing Specialist and District patients nodes(Includes Multi<br />
Video Conferencing System)<br />
• Increasing the utilization of centers with the help of private practitioners.<br />
• Adding digital telemedicine equipment to existing centers to improve their quality of<br />
work<br />
• Strengthening the SDH nodes and making them functional.<br />
• Strengthening the management system of telemedicine project.<br />
• Increasing CME’s for Medical and Paramedical staff.<br />
• Innovative activity like including pilot project of teleopthalmology.<br />
Budget requirement for <strong>2012</strong>-<strong>13</strong><br />
Budget is required for following purposes:<br />
Table – Budget required for Telemedicine Centers<br />
(Rs. in lakhs)<br />
Sir No. Particulars<br />
Unit<br />
Cost<br />
No. of<br />
units<br />
Budget<br />
required<br />
1<br />
Salary & TA/DA of Telemedicine<br />
Consultant<br />
4.<strong>13</strong> 1 4.<strong>13</strong><br />
2 Salary & TA/DA of Project Coordinator 3.00 1 3.00<br />
3 Salary & TA/DA of Program Assistant 1.37 1 1.37<br />
4<br />
Salary & TA/DA of Facility Manager for<br />
Old Districts & Specialist Centre<br />
1.92 33 63.36<br />
149
Sir No. Particulars<br />
5<br />
Salary & TA/DA of Facility Manager for<br />
Sub- Districts<br />
Unit<br />
Cost<br />
No. of<br />
units<br />
Budget<br />
required<br />
1.92 30 57.60<br />
6 Accountant for Specialist Centre 1.152 1 1.15<br />
7 Honorarium to Doctors – Specialist node 0.003 14000 42.00<br />
8 Honorarium to Doctors – Patient node 0.001 14000 14.00<br />
9 AMC of Telemedicine equipment 0.20 33 6.60<br />
Contingency to Specialist & Patient nodes<br />
10 ( including Civil works & other<br />
maintenance)<br />
0.10 63 6.30<br />
11 Contingency to State Level<br />
Procurement of additional equipment to<br />
Specialist & patient nodes of<br />
2.50 1 2.50<br />
12 telemedicine centers (Equipments,<br />
Multivideo camera, pilot project teleopthalmalogy)<br />
21.67 3 65.01<br />
<strong>13</strong> Training to Patient node/Specialist node 5.00 1 5.00<br />
14 Connectivity expenses 0.90 63 56.70<br />
15 Total 328.72<br />
150
B.20 : HEALTH INSURANCE SCHEMES<br />
(No proposal submitted for year <strong>2012</strong>-<strong>13</strong>)<br />
151
B.21 : RESEARCH, STUDIES AND ANALYSIS<br />
Two operational research topics of operational research importance are submitted for<br />
approval. National Rural Health Mission, Directorate of Health Services and Senior Faculty of<br />
Medical Colleges are involved in these research projects. Detailed description of the projects<br />
is as follows :<br />
The research studies submitted in this chapter are proposed by the teams in which retired<br />
Vice Chansler of Maharashtra University of Health Sciences, retired Professors and Deans and<br />
also Directors of Research Institutes are included. Remarks on these researches were shown<br />
to the team. The team has opined that, these studies are Maharashtra specific and they will<br />
definitely benefit for identifying high risk infants and their management. Considering this, it is<br />
proposed to sanction these studies.<br />
SUBSECTION - B.21.1 : PACKAGE OF NEONATAL CARE BY ASHA (PNC BY ASHA)<br />
Year of starting<br />
the<br />
scheme/initiative<br />
Introduction:-<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
New 0 0 20.890 12.898<br />
152<br />
Rs. in Lakhs<br />
Remarks<br />
Nearly 27 million babies are born in India every year and 1 million of them die before<br />
they complete four weeks of life. The neonatal mortality in India is 44/1000 LB. It is higher in<br />
<strong>rural</strong> areas as compared to urban area (49 <strong>rural</strong> Vs 27urban/1000 live births 1 ) NFHS II Survey<br />
has shown that Maharashtra has a neonatal mortality rate 37/1000 live births with urban &<br />
<strong>rural</strong> distribution of NMR as 41 and 31 respectively for 1000 live births 2 .<br />
Infant mortality is decreasing but there is no significant reduction in neonatal<br />
mortality. 45% of the neonatal deaths occur by 48 hours of birth 3 , the causes being birth<br />
asphyxia, trauma, problems related to prematurity and LBW and congenital malformations.<br />
For prevention of mortality within first 48 hours, good ANC care and quality obstetrical<br />
services are essential. Early registration of pregnancies and provision of antenatal services<br />
through existing <strong>health</strong> care services is emphasized under RCH II. JSY is being implemented<br />
for encouraging women to accept institutional deliveries. At present it is estimated that 90%<br />
of the deliveries in Maharashtra are hospital/<strong>health</strong> center deliveries. NSSK is being<br />
implemented all over Maharashtra to improve and render standardized newborn care<br />
immediately after birth. UNICEF has been providing support and expertise for training of
irth attendants at all levels. All these initiatives are expected to reduce the mortality of the<br />
newborn within 48 hours of birth.<br />
Under RCH II program and IMNCI strategy, the <strong>health</strong> workers are expected to pay<br />
visits to Low Birth Weight (LBW) babies and Normal Birth Weight (NBW) babies at least 6 and<br />
3 visits respectively. But in practice these visits are not feasible for ‘Health Worker Female’<br />
(ANM) due to heavy work load. One ASHA worker is identified for 1000 population i.e. 200 to<br />
250 houses. Considering their level of education, ability to learn new skills, availability and<br />
acceptability these women activists can be entrusted with the neonatal care after 48 hours<br />
which is crucial for neonatal survival but not satisfactory in the existing <strong>rural</strong> <strong>health</strong> care<br />
practice.<br />
The causes of neonatal mortality after 48 hours are neonatal infections, feeding<br />
problems, hypothermia, hypoglycemia etc. in a preterm and LBW baby these problems are<br />
more common. ASHAs can identify a baby who is doing well and a baby who is not doing well<br />
(At Risk) with specific training such as signs and symptoms of infection, Kangaroo Mother<br />
Care for LBWs, correct technique of breast feeding, identification of inadequacy of breast<br />
feeds, helping &counseling mothers to acquire breast feeding skills.<br />
Growth monitoring is an objective parameter for knowing baby’s wellbeing. The<br />
pediatricians can find out expected weight of the baby on given day during neonatal period<br />
from the knowledge of birth weight and the mathematical formula based on birth weight of<br />
the baby. All babies initially lose weight, become equal to birth weight and then start gaining<br />
weight. Although these phases are dependent on genetic and environmental factors to some<br />
extent, birth weight is the most important determinant provided adequate feeding is<br />
ensured.<br />
Existing growth monitoring charts are based on monthly growth monitoring. Under<br />
IMNCI weekly charts are available for identifying babies with low and very low weight for<br />
age 5 .<br />
Weekly Chart under IMNCI<br />
153
These charts cannot be used for daily growth monitoring of the baby. Daily growth<br />
monitoring charts for neonatal period were prepared by past graduate students of preventive<br />
and social medicine of Pune University 6, 7 . Based on these growth curves and existing<br />
mathematical formula with used by paediatricians 8,9,10 , we have developed a colour coded,<br />
birth weight specific daily growth monitoring charts. Use of these charts do not require any<br />
complicated formulate for calculating expected weight of the baby provided the birth weight<br />
of the baby is known. Retrospective prediction of birth weight is possible with 80% accuracy<br />
by birth weight specific growth velocity curves during early neonatal period 11 . Since 90% of<br />
births will be available for these hospital born babies for remaining 10% babies born at home<br />
retrospective prediction of birth weight can be undertaken by ASHAs after training. Under<br />
field conditions, the visits although specified on specific day after birth, can actually take<br />
place on different day hence daily growth monitoring charts are useful.<br />
Four patterns of growth monitoring charts are developed, use of which can be taught<br />
to ASHAs for neonatal growth monitoring. Considering a Birth Rate of 15/1000 population,<br />
one ASHA will have 15 births in 1000 population covered by her. There will be 5 LBWs & 10<br />
NBWS. She will required to pay 5 visits to LBW on day 3,7,14, 21 and 28 and 3 visits to NBW<br />
on day 3,7 and 28 as per IMNCI guide lines 12 . Thus in one year the ASHAs will be required to<br />
undertake 25 visits for LBWs and 30 visits for NBWS totaling to 55 visits i.e. about once a<br />
week visit.<br />
Foot Length is related to Birth Weight. Colour Coded Foot Caliper can be used to<br />
access ‘At Risk’ baby comparison of readings by Foot Length Caliper and birth weight will be<br />
undertaken. Foot length can be taken on 3 rd day also as it remains unaffected till 7 th day.<br />
If identification of babies ‘At Risk’ can be done, domiciliary care is provided in relation<br />
to feeding of the baby and referral of ‘At Risk’ baby and monitoring of growth is done on<br />
colour coded birth weight specific growth monitoring charts, we would achieve more gain in<br />
weight of the baby, prevent future SAM & MAM and reduce the mortality in neonates after<br />
48 hours for which at present no specific measures are being available.<br />
With these objectives in mind a research is planned for provision of package of services for<br />
neonates after 48 hours with the help of ASHAs<br />
154
Goal – To improve survival and growth of neonates after 48 hours of birth.<br />
Specific Objectives –<br />
1) To train ASHAs in identification of ‘At Risk’ neonate.<br />
2) To train ASHAs in accurately weighing the baby on electronic weighing machines.<br />
3) To train ASHAs in using colour coded birth weight specific daily growth monitoring charts.<br />
4) To train ASHAs in using Colour Coded Foot Length Caliper<br />
5) To train ASHAs in providing domiciliary care to babies ‘At Risk’ and counsel the mothers.<br />
6) To train ASHAs in timely referral of ‘At Risk’ babies.<br />
Research Methodology –<br />
The study will be under taken by Krishna Institute of Medical Sciences, Deemed University,<br />
(KIMSDU) Karad. (KIMSDU is situated in Satara District) The study will be conducted in two<br />
adjacent districts of Western Maharashtra namely Satara and Kolhapur.<br />
The duration of study will be 18 months as follows –<br />
1) Preparatory phase – 3 months. During the three months procurement of equipment,<br />
developing and printing of formats, preparation of training material and training of ASHAs,<br />
their supervisors and concerned PHC Staff will be undertaken. Strategy will be developed for<br />
collection compilation and Analysis of the data.<br />
2) Implementation phase – 12 months Data Collection, Supervision and monitoring will be<br />
done.<br />
5% of babies included in the study will be cross checked by home visits and all entries in the<br />
proforma including weight of the baby will be verified.<br />
3) Analysis, Interpretation and report writing – 3 months.<br />
Study Design – Community Based Interventional Study.<br />
Study Area – Inclusion Criteria<br />
1) PHC situated in <strong>rural</strong> area with approachable roads.<br />
2) All ASHAs are identified and functioning.<br />
3) All posts of PHCs are filled in.<br />
Exclusion Criteria<br />
1) PHC in close vicinity of cities and periurban areas.<br />
Two randomly selected eligible PHCs from each District.<br />
Control Area – Matching PHCs from same Taluka for each selected PHCs for study.<br />
Matching will be done for following characteristics<br />
i) Socio cultural background.<br />
ii) Availability and accessibility to secondary and tertiary <strong>health</strong> care facilities.<br />
iii) Estimated proportion of LBW.<br />
Sample Size Calculation – It is assumed that babies receiving package of domiciliary neonatal<br />
care will weight on an average 50gm more than babies from control area.<br />
n = 2 (Zα/2 + Z1-β) x SD 2<br />
d<br />
155
= 2 (1.96+ 1.28) x 290 2<br />
50<br />
= 706.28 = 707<br />
Therefore at least 707 babies in control and 707 babies in study group together from both the<br />
Districts.<br />
Package of Services to be provided to study population.<br />
Over and above the routine care given to Mothers & babies under RCH II program and IMNCI<br />
strategy under NRHM following package of services will be rendered.<br />
I) Identification of ‘At Risk Baby’ criteria of ‘At Risk Baby’.<br />
1) Any baby with birth weight
2) Colour Coded Foot Length Caliper (Annexure 2)<br />
Package of Services to be provided to Control population.<br />
The routine care will be given to Mothers & babies under RCH II program and IMNCI strategy<br />
under NRHM.<br />
Assumption<br />
300 Electronic weighing machines were supplied by State Health Systems Resource Centre<br />
(SHSRC) Pune from the grants received under NRHM to Pune, Satara and Kolhapur districts<br />
for the Project conducted by Krishna Institute of Medical Sciences Deemed University,<br />
entitled “Field Testing of Appropriate Technology Tools for monitoring of slow progress of<br />
labour and growth of LBW Babies below 2500gm at PHC/RH Level”<br />
These weighing machine will be made available for this proposed project to Krishna Institute<br />
of Medical Sciences Deemed University which will be given to ASHA workers and field<br />
monitoring staff. The machines will be standardized and if found inaccurate will be replaced<br />
and repaired. Hence all the machines are requested to be made available.<br />
Gantt Chart showing Activities under Project<br />
Sir<br />
No<br />
Activities 1 2 3 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3<br />
1 Procurement of<br />
equipment<br />
2 Developing and<br />
printing of formats<br />
3 Preparation of<br />
training material<br />
and training of<br />
ASHAs<br />
4 Undertaken by<br />
supervisors and<br />
concerned PHC<br />
staffs<br />
5 Development of<br />
strategy for<br />
collection,<br />
compilation and<br />
analysis of the<br />
data<br />
6 Data collection of<br />
12 months<br />
7 Supervision and<br />
monitoring<br />
157
8 Cross check of 5%<br />
babies<br />
9 Analysis and<br />
interpretation<br />
10 Report writing<br />
Budget requirement<br />
Budget requirement for the project is as follows:<br />
BUDGET FOR PROJECT- PACKAGE OF NEONATAL CARE BY ASHAs<br />
Project Work<br />
500 AWWs in study area<br />
100 AWWs in control area<br />
Project Work<br />
Study Area<br />
1 lac population-100 ASHAs<br />
1500 Births - BR 15/1000 population<br />
LBW 500 births x 5 visits x Rs.25 = Rs. 62,500 (5 visits to LBW)<br />
NBW 1000 births x 3 visits x Rs.25 = Rs.75,000 (3 visits to NBW)<br />
Control Area<br />
1 lac population-100 ASHAs<br />
1500 Birthsx2=3000<br />
LBW 500 births x 2 visits x Rs.25 = Rs.25,000<br />
NBW 1000 births x 2 visits x Rs.25 = Rs.5,0000<br />
5% check total weighing episode (Sample checking)<br />
Study-275/5500<br />
Control- 150/3000<br />
Total weighing episode 425 x Rs.25=Rs.10,625<br />
Training<br />
KIMS Team<br />
3 trainees x 3 days x 2 dist x DA 500= Rs.9,000<br />
Local trainer<br />
DLO x DA 300 x 12 visits x 2 Dist =Rs.7,200<br />
Block/PHC Supervisors<br />
Sup 4 x Rs.150x 12visits x2 Dist=Rs.14,400<br />
TADA at trainers ASHAs/ Supervisors<br />
ASHAs /Sup 210x Rs.150x3days=Rs.94,500<br />
Working Lunch and snacks for participants<br />
210 x Rs.100x 3 days= Rs.63,000<br />
Training materials for trainees<br />
210 x Rs.100 = Rs.21,000<br />
POL for training 200km x Rs.10x 3 daysx2 Dist =Rs.12,000<br />
158
Field monitoring supervision & guidance<br />
POL considering 10 visits per month by SRO<br />
Average 150 km per visit travel distance<br />
150km x 10 visits x 12 months x 2 SRO x 10 per km charges= Rs.36,0000<br />
DA to SRO<br />
10 visits x 15 months xRs.1000x 2 dist = Rs.3,00,000<br />
PHC level ASHA supervisor forms checking<br />
Birth in study area 1500<br />
Birth in control area 1500<br />
Total births 3000 x Rs. 10 = Rs.30,000<br />
Material & Logistic supply<br />
1. Stationary files, proforma printing including weighing charts<br />
1500 x Rs. 25 = Rs. 37,500 for study area<br />
1500 x Rs. 10 =Rs. 15,000 for control area<br />
2. Foot length calipers<br />
225 x Rs. 100 = Rs.22,500<br />
3. Measuring scale, rubber, pencil, sharpener,etc<br />
210 x Rs. 15 = Rs.3,150<br />
4. Project kit bag for ASHAs/Sup/DLS/DLO<br />
225 x Rs. 100 = Rs. 22,500<br />
5. Contingency: Telephone, postage, courier, Xerox ,office stationary-<br />
Rs.15,000<br />
6. Statistical analysis - Rs.30,000<br />
7. Report Writing - Rs.10,000<br />
TOTAL BUDGET= Rs. 12,89,875<br />
SUBSECTION - B.21.2 : MULTICENTRIC BIRTH COHORT TO STUDY THE ANTHROPOMETRIC<br />
MEASUREMENTS OF CHILDREN IN MAHARASHTRA AND THEIR SOCIOEDMOGRAPHIC<br />
CORRELATES<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
New 0 0 39 39.000<br />
Principal investigator : Dr.Uday Bodhankar 1 , Dr Abhay Chowdhary 2<br />
159<br />
Rs. in Lakhs<br />
Remarks
Co- principal investigators : Dr. Satish Pawar 3 , Dr. Archana Patil 4 , Dr Pramila Menon 5 , Dr<br />
Leena Dhande 6<br />
Other investigators : Dr. Shanshank Dalvi 7 , Dr. Jayant Shah 8 , Dr. Yashwant Patil 9 , Dr.M.S.<br />
Rawat 10<br />
Dr. Nita Hatkar 11 , Dr. Sandeep Bavdekar 12 , Dr. Ashok Rathod <strong>13</strong><br />
Advisors : Rajalakshmi Nair 14 , Dr Mrudula Phadke 15<br />
A joint collaborative project from Directorate of Health Services, National Rural Health<br />
Mission, Medical Colleges & Maharashtra University of Health Sciences<br />
1, 5, 7 - Maharashtra University of Health Sciences, Nashik, 2 – Haffkine Research Institute,<br />
Mumbai , 3 – National Rural Health Mission, 4 – Directorate of Health Services, 6,10,11,12,<strong>13</strong><br />
– Government and Corporation Medical Colleges Maharashtra, , 8, 9 – Pediatricians, BPNI,<br />
Pvt. Medical Colleges, 14, 15 - Special Invitee and Experts.<br />
Introduction :<br />
WHO has conducted a multicentric multicounty study in which the anthropometric<br />
measurements of children reared in optimal conditions (non-smoking mothers, exclusive<br />
breast feeding…. ) in various countries like Ghana Oman, USA., India, Brazil, Norway have<br />
been pooled together to formulate new growth charts and then the z-scores with percentiles<br />
to classify malnutrition. As per these scores, 6.4%of Indian children get classified as having<br />
severe acute malnutrition (SAM ).<br />
Growth potential of children in developed and developing countries is likely to be different<br />
though the WHO new growth charts show that infants under optimum conditions grow<br />
similarly irrespective of country of origin or ethnic background. This difference in growth<br />
potential may be due to various factors like genetic potential, diet, family sizes and<br />
intrauterine influence. The question that arises is, is it appropriate to have the same growth<br />
standards for different countries? This question can be answered only when we have<br />
anthropometric measurements recorded for full term normal infants in the country under<br />
consideration and compare these with the corresponding measurements in those from<br />
developed nations. To begin with we are forming a birth cohort in Maharashtra, India and we<br />
propose to study their anthropometric measurements with a plan to do similar studies in<br />
various States of India.<br />
In addition to this ,it has been observed that two important anthropometric measurements<br />
i.e. wt for age and wt for ht. which have been operationally used in the field by ANM/AWW<br />
and Medical Officers respectively often create difficulty in accurate diagnosis of SAM. This is<br />
because ANM & AWW undertake wt. for age measurement. When the baby is referred on<br />
the basis of above as SAM or MAM, the situation with the Medical Officer who uses wt. for<br />
ht. as the criterion becomes ambiguous. Some babies classified as SAM may not be so while<br />
160
using wt. for ht. and vice-versa. Therefore, we also feel the need to validate these two<br />
indicators vis-à-vis the third one i.e. the midupper arm circumference (MUAC).<br />
Aims and Objectives :<br />
Primary -<br />
1)To obtain anthropometric data from infants and children from Maharashtra.<br />
2) To evaluate the utility and diagnostic efficacy of wt for age, wt for ht and MUAC in infants<br />
and children to detect SAM<br />
Secondary -<br />
3) To assess renal, immunological, biochemical and hepatic functions in babies detected to<br />
have malnutrition and correlate anthropometrically.<br />
Review of literature :<br />
Studies have been done in other developing and developed countries on anthropometry of<br />
children aged 0-5 years, WHO study, NFHS data, studies looking at factors influencing growth<br />
potential of children in different countries. What happens to growth of Indian kids reared in<br />
India initially and later in developed countries. Is the growth of children born to Indian<br />
parents in developing countries comparable to their native counterparts? Some studies done<br />
in India by Dr. Khadilkar show a different picture compared to WHO new growth charts.<br />
Methods :<br />
This is a multicentric study that will be conducted in Government Medical College hospitals<br />
and private nursing homes, primary <strong>health</strong> centers, <strong>rural</strong>, sub-district hospitals in various<br />
cities and towns of Maharashtra so as to cover families from varied socio-economic<br />
backgrounds. We shall recruit 10000 women from different wealth quintiles. We will form a<br />
birth cohort recruiting babies after due informed consent of the mothers taken in last<br />
trimester of pregnancy. Along with this longitudinal study a cross sectional study will be<br />
undertaken to study anthropometry of infants of various months as they attend the<br />
immunization clinics of the hospitals. Longitudinal study would be on 1000 infants and 9000<br />
infants from birth to 3 years of age will be studied cross sectionally.<br />
Duration of study :<br />
Data collection - 6 months for cross sectional study. 2 years for longitudinal study. Data<br />
analysis- 3 months, paper writing- 6 months, dissemination- 6 months<br />
Post funding Timeline<br />
Activity 3mths 6 9 12 18 24 36<br />
Meeting of all investigators and CRF development + + +<br />
161
workshop<br />
Recruitment of ROs and ANMs +<br />
Training of Ros and ANMs +<br />
Procurement of equipment +<br />
Piloting of CRF +<br />
Data collection- enrollment, follow-up + +<br />
Data analysis + +<br />
Paper writing +<br />
Dissemination of data +<br />
Sample size- per center and total. For each center, 1000 women from different wealth<br />
quintiles.<br />
Inclusion criteria will be as follows-<br />
1. Mother willing to deliver and follow up at study site for 3 years<br />
2. Mother not indulging in active smoking<br />
3. Mother willing to comply with IYCF principles i.e. initiate breast feeding within ½ hour<br />
of birth in normal and within 4 hrs of birth for caesarean section, breast feed<br />
exclusively for 6 months, introduce complementary foods at 6 months and continue<br />
breast feeding till 2 years.<br />
4. Mother willing not to formula feed the baby or bottle feed the baby<br />
5. However mothers who adapted different feeding practices will be included and put in<br />
a separate category while analysing.<br />
Exclusion criteria will be as follows :<br />
1. Babies born preterm.<br />
2. Babies with Genetic Syndromes congenital malformations.<br />
3. Babies with overt cardiac, respiratory, renal, neurological, gastrointestinal l,<br />
endocrinolocal or any other disease.<br />
The babies will be subjected to anthropometric measurements at birth, at 6,10,14 weeks,<br />
9 months, 12 months, 15-18 months, 24 months, 36 months. Those written in italics are<br />
home visits rest are immunization visits. In case a patient does not come for scheduled<br />
immunization visit, she will be given a reminder for the same. The following<br />
measurements will be recorded - weight, length till 2 years followed by height, MUAC,<br />
upper arm length, fore arm length, OFC, U/L segment ratio, triceps and infraspinatus skin<br />
fold thickness and chest circumference. In case a baby is found to be in the SAM or MAM<br />
category, immediate treatment will be given at nearby VCDC, CTC, Medical College OPD,<br />
indoor – Hospital. Blood will be collected for renal hepatic immunological (IgG, IgA, IgM<br />
interleukins etc.) and biochemical tests.<br />
Demographic data of family will be entered in Case report form. We will follow WHO<br />
definitions for exclusive breast feeding, TICF, TIBF, bottle feeding etc.<br />
162
Team- Pediatricians, anthropologists, trained research officers, social workers, ANMs,<br />
statistician, data entry operators<br />
Financial Implications –<br />
Non- recurring -<br />
Weighing balance, tapes (MUAC) caliper identical at all centers. Rs.15,000/- per center.<br />
Rs.1,50,000/- at 10 centers.<br />
Recurring –<br />
Travel Rs. 20,000/- per center every year.<br />
Rs. 2,00,000/- for 10 centers for 1 year.<br />
Stationery Rs.1,00,000/- for all the centers<br />
Staff- Research Assistant- (MBBS or MD) nurse or ancillary helper Rs. 20,000/- per month<br />
Rs.24,00,000/- per year.<br />
Cost for investigations (Chemicals, Lab kits) Rs.10,00,000/-<br />
Contingency Rs.50,000/-<br />
Total Expenditure -<br />
Rs.39,00,000/-<br />
163
Year of starting<br />
the<br />
scheme/initiative<br />
B.22 : ESTABLISHMENT AND FUNCTIONING OF SHSRC<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
164<br />
Rs. in Lakhs<br />
Remarks<br />
2008-09 100 100 100 100.000 No change<br />
NRHM is conceived as a decentralized district planning led sector program. Such programs<br />
require resource teams at sub district, district, state and <strong>national</strong> level, that are fully<br />
conversant with principles of decentralized planning and assessment of people’s needs. As a<br />
consequence, State Health Society needs technical and management support from<br />
established professionals in the field. This is required to drive change and reform in planning,<br />
implementation and monitoring of <strong>health</strong> sector programs in general and family welfare<br />
programs in particular.<br />
The State Health Resource Centre (SHRC) is conceived primarily as an agency/institution that<br />
is responsive to and available for providing technical assistance to Centre/States and districts<br />
for building their capacity in improving service delivery in the <strong>health</strong> sector.<br />
1. SHRC Units:<br />
The SHRC will have the following units:<br />
1. Public Health Unit, covering Public <strong>health</strong> activities for improvement in <strong>health</strong> care<br />
delivery<br />
2. Social Development Unit, covering civil society partnerships, gender empowerment,<br />
community mobilizations sub units.<br />
3. Financial Management Unit including procurement specialists, fiduciary reform<br />
specialists, <strong>health</strong> insurance specialists.<br />
4. Human resource management unit including training specialists in several areas.<br />
5. Planning, Research and Documentation Unit, including MIS and e-governance<br />
6. IEC, Social Marketing and Public Private Partnership Unit.<br />
It is proposed to appoint 6 Senior Consultants as head of each unit and one additional senior<br />
consultant as public <strong>health</strong> expert.<br />
1.1. Support Unit
Support staff of the SHRC will be headed by Resident Assistant Director or Resident<br />
Consultant. This person will look after day to day functioning of the SHRC. He/she will keep all<br />
the facilities of SHRC in working condition and arrange for all the administrative activities<br />
required for smooth functioning of the SHRC.<br />
2. Budget requirement <strong>2012</strong>-<strong>13</strong><br />
Budget Requirement for SHRC will be on following heads:<br />
3. Salary and daily allowances<br />
Budget required for salary and daily allowances is as follows:<br />
Table – : Budget requirement for salary and daily allowances<br />
165<br />
Rs. In Lakhs<br />
Sir Particulars Unit cost No. of Units Total cost<br />
1 Salary of Executive Director 9 1 9<br />
2 Salary of Sr. Consultants 6 4 24<br />
3 Remuneration<br />
consultant<br />
to Short term 6 1 6<br />
4 Salary of Asst. Director/R. Consultant 4.8 1 4.8<br />
5 Administrative Officer 2.4 1 2.4<br />
7 Librarian 1.2 1 1.2<br />
8 Statistician 1.2 1 1.2<br />
9 Data Entry Operator 1.2 2 2.4<br />
10 Steno 1.8 1 1.8<br />
<strong>13</strong> Travel cost for officers and staff 12 1 12<br />
Total 64.8<br />
4. Total budget requirement<br />
Total budget required for establishment and starting of functioning of SHSRC is mentioned in<br />
table below:<br />
Table – : Budget requirement for SHSRC : <strong>2012</strong>-<strong>13</strong><br />
Sir Particulars Unit cost No. of units<br />
Rs. In Lakhs<br />
Budget<br />
requirement<br />
1 Computer and other office equipment 0.5 4 2<br />
2 Salary of Staff 64.8 1 64.8<br />
3 Cleaning, sweeping, security 3.6 1 3.6<br />
4 Evaluation studies and reports 5 4 20<br />
5 Other expenses including renovations and<br />
repairs<br />
9.6 1 9.6<br />
Total 100
SECTION – B.23 : SUPPORT SERVICES<br />
SUBSECTION : B.23.1 : SUPPORT STRENGTHENING NPCB<br />
National Program for Control of Blindness is included in Component – D of the PIP. However,<br />
activities which are very important for the program and not permissible as per NPCB<br />
guidelines are included in this chapter. Following activities are proposed for year <strong>2012</strong>-<strong>13</strong><br />
ACTIVITY : B.23.1.1 : OPERATIONALIZATION OF SUPERSPECIALITY HOSPITAL FOR CHILD EYE<br />
CARE<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2011-12 120 29.88 29.880<br />
166<br />
Rs. in Lakhs<br />
Remarks<br />
GoI has approved Rs. 120.0 Lakh for Strengthening of Superspeciality Hospitals on the lines of<br />
Shankara Netralaya Chenni for the treatment of Neonatal, Infant and Child Eye Diseases.<br />
Accordingly, Superspeciality Hospital Amravati, Government Medical College Aurangabd and<br />
BJ Medical College Pune are selected for this purpose and equipment required for this<br />
purposes also being provided to these institutions.<br />
This facility being provided is being utilized for children with eye diseases identified by<br />
Medical Officers during Anganwadi visit and School Health Examination Program. Out of the<br />
three institutions above, two are functioning Medical Colleges. Trainee doctors for Child Eye<br />
Diseases are available at Aurangabad and Pune but not available at Amravati. Therefore, it is<br />
proposed to provide trained doctors and staff through NRHM for this purpose.<br />
Trained doctors and budget required for this activity is as follows:<br />
Table – : Budget requirement for operationalization of Superspeciality hospital Amravati<br />
Rs. In Lakhs<br />
Sir Activity Unit cost<br />
No. of<br />
units<br />
Budget<br />
required<br />
1 Per operation charges to Specialist 0.05 300 15<br />
2 Support staff for operations (2 persons) 1.44 2 2.88<br />
3 Consumables required per operation 0.03 300 9
3 Contingency 3 1 3<br />
Total 29.88<br />
ACTIVITY : B.23.1.2 : PROVISION OF HIRED VEHICLES TO OPHTHALMIC SURGEONS FOR<br />
CATARACT OPERATIONS<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
New 12.9 12.900<br />
167<br />
Rs. in Lakhs<br />
Remarks<br />
Cataract operations are most important activity for prevention of blindness. In Maharashtra,<br />
government agencies are performing about 1.4 lakh operations every year. The number of<br />
operations is not increasing significantly as compare to number of cases available and<br />
facilities being provided. Considering this, Cataract camps at designated SDH are being<br />
performed. For this, GoI – NPCB has provided vehicles to surgeons. As these vehicles are now<br />
very old, it is becoming very difficult for doctors to travel to peripheral institutions and<br />
conduct camps.<br />
GoI has provided Rs. 125/cataract operation for mobility support. But this budget is to be<br />
utilized for patient transport. Therefore there is no budget for travel to Surgeon and his / her<br />
team to SDH.<br />
Considering this, it is requested to provide budget for hiring of suitable vehicle to Ophthalmic<br />
Surgeons for operations.<br />
Budget required for this activity is as follows:<br />
Table – : Budget requirement for mobility support to Ophthalmic Surgeons<br />
Rs. In Lakhs<br />
Sir Activity Unit cost<br />
No. of<br />
units<br />
Budget<br />
required<br />
1<br />
Hiring of vehicles for Cataract operation<br />
camps for districts where government<br />
vehicles are condemned. (six camps per<br />
district for 27 districts)<br />
0.05 162 8.1<br />
2 POL for vehicles which are on road 1.2 4 4.8<br />
Total 12.9
ACTIVITY : B.23.1.3 : PROCUREMENT OF OPHTHALMIC EQUIPMENT FOR CATARACT<br />
OPERATIONS<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
New 0 00 4<strong>13</strong>.05 4<strong>13</strong>.050<br />
168<br />
Rs. in Lakhs<br />
Remarks<br />
Ophthalmic equipments being provided to hospitals under the NPCB. However, at many<br />
paces the microscopes are old and non-functional now. Budget available with the NPCB is not<br />
sufficient. In addition to this, Maharashtra has started ophthalmic operations at selected<br />
SDH/GH and Women Hospitals.<br />
Some ophthalmic equipment are important for treatment of eye diseases but are not being<br />
provided under NPCB. Therefore, it becomes very difficult to provide quality services to poor<br />
patients. These equipment need to be provided from other sources.<br />
Therefore it is requested to provide Ophthalmic Equipment in addition to NPCB provisions as<br />
follows:<br />
Sir Activity Unit cost<br />
No. of<br />
units<br />
Budget<br />
required<br />
A<br />
Equipment sanctioned under NPCB but<br />
needed for providing to new hospitals<br />
1 Pheco-Emulsification Machine 8 6 48<br />
2 Operating Microscope 10 8 80<br />
3 Keratorefractometer 3 8 24<br />
Total<br />
Equipment not in the list of NPCB budget<br />
152<br />
B requires for quality patient care for<br />
District Hospitals<br />
1 Ophthalmic OT table 0.85 23 19.55<br />
2 Air Purifier 0.5 23 11.5<br />
3 Non-contact Tonometer 4 23 92<br />
4 I-Chart 0.5 23 11.5<br />
5 Auto perimeter 5.5 23 126.5<br />
Total 261.05<br />
Grand Total 4<strong>13</strong>.05
SUBSECTION : B.23.2 : SUPPORT STRENGTHENINGMIDWIFERY SERVICES UNDER MEDICAL<br />
SERVICES<br />
(No Budget requested)<br />
SUBSECTION : B.23.3 : SUPPORT STRENGTHENING NVBDCP<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2011-12 0 306.99 169.470<br />
169<br />
Rs. in Lakhs<br />
Remarks<br />
Sr.<br />
No.<br />
Component Amt required in Lakh<br />
1 Malaria Link Volunteers 37.6<br />
2 Strengthening Of Research Cum Training Centre,<br />
Nagpur<br />
9.89<br />
3 strengthening of Zonal Office Nagpur 37.89<br />
4 Purchase of ACT & RDT for the year <strong>2012</strong> - <strong>13</strong> 84.09<br />
Total 169.47<br />
1. Malaria Link Volunteers (MLVs)<br />
To reduce time lag between blood smears collection & examination MLVs are<br />
proposed in the district Gadchiroli at sub-center. MLV will collect B.S. collected by MPWs<br />
every day & transport these collected B.S. to PHC same day. Report of B.S. examined at PHC<br />
will be handed over to MLVs. This activity will help to minimize time lag between collection<br />
of B.S , examination & treatment.<br />
Total No. of sub centers in Gadchroli district – 376<br />
MLVs will be appointed from June to March = 10 months<br />
Salary 1000/MLV = 376 X 1000 X 10 = 37.60 Lakh<br />
2. PROPOSAL FOR STRENGTHENING OF RESEARCH CUM TRAINING<br />
CENTRE, NAGPUR UNDER NVBDCP NRHM PIP <strong>2012</strong>-<strong>13</strong>.
The Research cum Training Centre, Nagpur is the only State Level Training Centre under<br />
NVBDCP Maharashtra State for filariasis. Filariasis is the main problem in all the districts in<br />
this zone. Training on Filariasis and Vector Borne Diseases is arranged regularly throughout<br />
the year for various cadres from all the districts in Maharashtra state. Strengthening is<br />
necessary for effective functioning of the Centre.<br />
At present, the center is situated in old building in Deputy Director's campus. Considering the<br />
load of various trainings, following are proposals to strengthen the training center.<br />
1) One post of Data Entry Operator on contractual basis.<br />
2) Renovation of the Training center.<br />
3) Provision of Classroom Furniture<br />
4) Provision of office material as Xerox machine, fax, computer, printer etc.<br />
5) Provision of training material as laptop, projector, exhibition models etc.<br />
1) Data Entry Operator on contractual basis:<br />
This office has to organize trainings of various cadres from different districts. A large<br />
database of training status of various cadres is to be maintained. For this purpose no separate<br />
Data Entry Operator or computer assistants available in this office. So it becomes difficult to<br />
collect data timely and arrange accurately and organize trainings. So it is suggested to sanction<br />
one post of DEO to Zonal office on contractual basis.<br />
Details of honorarium :<br />
Rs.8000pm x 8 months = 64000/-<br />
2) Renovation of the Training center.<br />
The classroom and Office is situated in old building which needs to be renovated. Approximate<br />
cost for classroom and Office renovation Rs. 5.00 lakhs.<br />
3) Provision of Classroom Furniture<br />
Comfortable sitting arrangement needs to be provided for trainees. Approximate cost for 30<br />
wooden table and chairs Rs. 1.5 lakhs.<br />
4) Provision of office material as xerox machine,fax, computer, printer etc.<br />
Provision of office material as xerox machine,fax, computer, printer etc.<br />
Cost of Rs. 1.50 lakhs<br />
.<br />
5) Provision of training material as laptop, projector, exhibition models etc.<br />
There are various trainings organized at this Training center. There are no training equipment<br />
and exhibition models with this training center. To organize various trainings, it is suggested to<br />
provide following training aids.<br />
Provision of training material & Equipment such as laptop, projector, exhibition models etc.<br />
Cost of Rs. 1.25 lakh<br />
………………………………………………………………………………………<br />
170
APPROXIMATE BUDGET REQUIRED FOR RESEARCH CUM TRAINING<br />
CENTRE, NAGPUR<br />
1) Data Entry Operator on contractual basis: = Rs. 0.64 lakh<br />
2) Renovation of the Training center = Rs.5.00 lakh<br />
3) Provision of Classroom Furniture = Rs.1.50 lakh<br />
4) Provision of office material as xerox machine, fax, computer, printer etc<br />
= Rs.1.50 lakh<br />
5) Provision of training material as laptop, projector, exhibition models etc<br />
= Rs.1.25 lakh<br />
TOTAL = Rs. 9.89 lakh<br />
3. PROPOSAL FOR STRENGTHENING OF ZONAL OFFICE NAGPUR UNDER<br />
NVBDCP NRHM PIP <strong>2012</strong>-<strong>13</strong><br />
Zonal Office, Nagpur (Assistant Director of Health Services, (Malaria), Nagpur) is<br />
monitoring & supervising the vector borne diseases in 6 districts viz. Bhandara, Chandrapur,<br />
Gadchiroli, Nagpur, Gondia &, Wardha.<br />
These districts are more prone for Malaria, Filaria, Dengue, Chandipura, Chikungunya<br />
& J.E. In Last 3 years malaria is in increasing trend in Gadchriloi, Chandrapur & Gondia<br />
districts. Remaining districts are also vulnerable for the disease.<br />
Since last 2 to 3 yrs. the cases of Chandipura Encephalitis are increasing in the district<br />
of Bhandara, Nagpur and Chandrapur. The mortality of Chindipura encephalitis was more in<br />
these districts.<br />
Filariasis is also prevalent in Chandrapur district. Maximum number of cases of filarial<br />
hydrocele & Lymphatic Filariasis are found in Chandrapur district which is highest in<br />
Maharashtra state. There are cases of filarisis in all other districts.<br />
The epidemics of Chikungunya were also notified in these districts and even today<br />
sporadic cses of Chikungunya are also occurring in these districts.<br />
Considering the load of above diseases it needs continuous monitoring and supervision<br />
form the zonal office. Following are proposals to strengthen the zonal office.<br />
1) One post of Data Entry Operator on contractual basis.<br />
2) Extension of the Zonal Office building<br />
3) Provision of warehouse.<br />
4) Provision of office material as computer printer etc.<br />
5) Provision of training material as laptop, projector etc.<br />
6) Entomological kits and material & equipment of the zonal entomologist.<br />
1) Data Entry Operator on contractual basis:<br />
This office is providing technical support to the districts. Data regarding various<br />
diseases from the DMOs/ FOs is being collected compiled and analyzed and need to be sent<br />
higher officers. As Jt.DHS Pune, NVBDCP HQ, ROH & FW Pune for this purpose no separate<br />
171
Data Entry Operator or computer assistants available in this office. So it becomes difficult to<br />
collect data timely and analyze accurately and send it in the HMIS Formats. So it is suggested<br />
to sanction one post of DEO to Zonal office on contractual basis.<br />
Details of honorarium :<br />
Rs.8000pm x 8 months = 64000/-<br />
2) Extension of the Zonal Office building There is no separate office building for zonal<br />
office. At present zonal office is occupying few small rooms in the building of Filaria Control<br />
Unit Office. Due to lack of space it is difficult to provide separate chamber for Zonal<br />
Entomologist. Even the room is not available for Laboratory. So it is suggested that budget<br />
may be provided for extension of the existing building.<br />
Approximate cost :<br />
Extension of Zonal Office …. Rs. 25.00 lakh<br />
3)Provision of warehouse :<br />
There is no separate warehouse for storage of medicine & insecticides which is<br />
supplied from state level. This may result in damage or theft of the material. So it is suggested<br />
that the separate warehouse may be provided.<br />
Construction of Warehouse …. Rs. 10.00 lakh<br />
4) Strengthening of office :<br />
Provision of material such as computer, Laser printer, UPS, etc.<br />
Cost Rs. 0.50 lakh<br />
5) Provision of training aids:<br />
There are various trainings organized at Zonal level. There are no training equipment<br />
with this office. To organize trainings at zonal as well as at district levels, it is suggested to<br />
provide following training aids.<br />
Provision of training material & Equipment such as laptop, projector etc.<br />
Cost of Rs. 0.75 lakh<br />
6) Entomological kits and material & equipment of the zonal entomologist :<br />
There are 2 posts of Zonal Entomologists in this region. The Entomological kits<br />
have not been provided. It is suggested to supply 2 entomological kits to this region.<br />
Approximate Cost Rs. 0.50 lakh each x 2 kits = 1.00 lakh<br />
APPROXIMATE BUDGET REQUIRED FOR ZONAL OFFICE, NAGPUR<br />
1) Data Entry Operator on contractual basis = Rs.0.64 lakh<br />
2) Extension of the Zonal Office building and = Rs.25.0 lakh<br />
3) Provision/construction of warehouse = Rs.10.0 lakh<br />
4) Provision of office equipment like computer printer etc. = Rs. 0.50 lakh<br />
5) Provision of training aids like laptop, projector etc. = Rs. 0.75 lakh<br />
6) Entomological kits for two zonal entomologists = Rs. 1.00 lakh<br />
Total 37.89<br />
172
4. CASH ASSISTANCE REQUIRED UNDER NRHM FLEXI FUND TO PURCHASE OF ACT & RDT<br />
FOR THE YEAR <strong>2012</strong> – <strong>13</strong><br />
Sr.<br />
No<br />
SUBSECTION : B.23.4 : SUPPORT STRENGTHENING RNTCP<br />
S.<br />
No<br />
.<br />
1<br />
2<br />
Name of the<br />
District<br />
Budget Head<br />
Civil works:-<br />
Establishment/Renova<br />
tion of DTCs in 8<br />
districts Akola,<br />
Nanded, Jalna, Hingoli,<br />
Sindhudurg, Washim,<br />
Akola corp and<br />
Amravati corp.<br />
Establishment or<br />
renovation of training<br />
facility with hall and<br />
hostel facility<br />
Artesunate 50 mg + Sulphadoxine<br />
Pyremethamine (500+25mg)<br />
Yearly<br />
Requiremen<br />
t<br />
Amount<br />
Propose<br />
d (Rs in<br />
Lakhs)<br />
25 %<br />
Requiremen<br />
t<br />
Amount<br />
Approve<br />
d<br />
(Rs.in<br />
Lakhs)<br />
280 280<br />
Cost Yearly<br />
Requiremen<br />
t<br />
Justification/R<br />
emarks<br />
Approved as<br />
the provision<br />
for<br />
maintenance is<br />
Rs 4500/<br />
annum per DTC<br />
for existing<br />
DTCs.<br />
Malaria Rapid Diagnostic Test<br />
25 %<br />
Requiremen<br />
t<br />
1 Gadchiroli 7395 1849 231094 84896 21224 938101<br />
2 Chandrapur 12789 3197 399656 97233 24308 1074425<br />
3 Thane 5142 1286 160688 192399 48100 2126009<br />
4 Raigad 3795 949 118594 69031 17258 762793<br />
5 Mumbai<br />
Municipal<br />
Corporation<br />
4800 1200 150000 221526 55382 2447862<br />
Total 33921 8480 106003<br />
1<br />
665085 166271 7349189<br />
Total Cost Rs.1060031 + 7349189 = 8409220/-<br />
Comments/Justificati<br />
on from the States (<br />
please also mention<br />
the amount with<br />
clear justification<br />
under each head)<br />
173<br />
Proposed<br />
Amount in<br />
Lakhs<br />
280<br />
200 200 Approved 200<br />
Cost
S.<br />
No<br />
.<br />
2<br />
3<br />
4<br />
Budget Head<br />
Laboratory<br />
strengthening:-<br />
Strengthening of IRL<br />
Pune for Liquid Culture<br />
Travel expenses to Coinfected<br />
to visit ART<br />
Centre<br />
Travel expenses to<br />
MDR TB suspect to<br />
DTC<br />
Amount<br />
Propose<br />
d (Rs in<br />
Lakhs)<br />
Amount<br />
Approve<br />
d<br />
(Rs.in<br />
Lakhs)<br />
40 0<br />
25 25<br />
30 30<br />
Justification/R<br />
emarks<br />
Not approved<br />
as the liquid<br />
culture<br />
strengthening<br />
of Pune IRL is<br />
already in<br />
RNTCP lab<br />
scale up plan.<br />
Comments/Justificati<br />
on from the States (<br />
please also mention<br />
the amount with<br />
clear justification<br />
under each head)<br />
11000 coinfected<br />
patients expected to<br />
travel to ART centre<br />
for treatment<br />
initiation; scheme<br />
already initiated this<br />
year and requires to<br />
be continued to pass<br />
the benefit of early<br />
ART treatment<br />
initiation and prevent<br />
mortality due to comorbidity.<br />
The Scheme is<br />
already initiated in<br />
this year and requires<br />
to be continued.<br />
Maharashtra with all<br />
districts under PMDT<br />
with Criteria B will<br />
have around<br />
estimated 20,000 TB<br />
suspects annually;<br />
with Rs. 150 average<br />
cost for each patient<br />
174<br />
Proposed<br />
Amount in<br />
Lakhs<br />
0<br />
25<br />
30
S.<br />
No<br />
.<br />
5<br />
6<br />
Budget Head<br />
Air-borne infection<br />
control<br />
Additional<br />
investigations -<br />
Thyroid function test,<br />
CT-Thorax etc.<br />
Amount<br />
Propose<br />
d (Rs in<br />
Lakhs)<br />
Amount<br />
Approve<br />
d<br />
(Rs.in<br />
Lakhs)<br />
110 110<br />
30 30<br />
Justification/R<br />
emarks<br />
Comments/Justificati<br />
on from the States (<br />
please also mention<br />
the amount with<br />
clear justification<br />
under each head)<br />
travelling to DTC will<br />
need around 30 lakh.<br />
Medical colleges /<br />
District hospitals with<br />
provision for MDR TB<br />
hospitalization and<br />
decentralized<br />
management of MDR<br />
TB patients will<br />
require up gradation<br />
and AIC measures -<br />
11 places @ Rs.10<br />
lakh per site; Similarly<br />
35 TB wards in district<br />
hospitals needs AIC<br />
measures @ 5 lakh<br />
per ward<br />
The Scheme is<br />
already initiated in<br />
this year and requires<br />
to be continued.<br />
Specialized<br />
investigations not<br />
available in the<br />
government hospital<br />
especially for the<br />
MDR patients needs<br />
to be done from<br />
private sector.<br />
Approximately 4000<br />
MDR TB patients<br />
requiring such<br />
investigations at an<br />
average cost of<br />
175<br />
Proposed<br />
Amount in<br />
Lakhs<br />
110<br />
30
S.<br />
No<br />
.<br />
7<br />
8<br />
Budget Head<br />
Strengthening of the<br />
Laboratory - C&DST<br />
Computer & Printer<br />
for 41 Medical<br />
Colleges<br />
Amount<br />
Propose<br />
d (Rs in<br />
Lakhs)<br />
Amount<br />
Approve<br />
d<br />
(Rs.in<br />
Lakhs)<br />
<strong>13</strong>5 <strong>13</strong>5<br />
20.50 20.50<br />
Justification/R<br />
emarks<br />
Comments/Justificati<br />
on from the States (<br />
please also mention<br />
the amount with<br />
clear justification<br />
under each head)<br />
Rs.750 per head<br />
C&DST labs up<br />
gradation for<br />
decentralized services<br />
at Sewri TB hospital,<br />
GMC Yeotmal, Dhule,<br />
Solapur, Sangli &<br />
Aurangabad - 6 labs<br />
@ 45 lakh per lab<br />
Already completed<br />
the procurement in<br />
the financial year<br />
2011-<strong>2012</strong><br />
176<br />
Proposed<br />
Amount in<br />
Lakhs<br />
Total 1460.5 1420.5 810.00<br />
SUBSECTION : B.23.5 : CONTINGENCY SUPPORT TO GOVERNMENT DISPENSARIES<br />
(Budget not requested)<br />
SUBSECTION : B.23.6 : OTHER NDCP SUPPORT PROGRAMS<br />
Following are the proposals submitted by other NDCP programs for support<br />
<strong>13</strong>5<br />
Nill
ACTIVITY : B.23.6.1 : RENOVATION OF OCCUPATIONAL THERAPY AND KITCHEN<br />
DEPARTMENT IN 4 REGIONAL MENTAL HOSPITALS – 2 nd PHASE<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2011-12 500 153 153.000<br />
177<br />
Rs. in Lakhs<br />
Remarks<br />
Introduction:-<br />
This project is approved by NRHM in 2011-12 and provided budget of Rs. 500.0 Lakh. This<br />
budget is being utilized as per the sanctioned proposal and budget required for year <strong>2012</strong>-<strong>13</strong><br />
is submitted for approval.<br />
Occupational therapy (O.T.) in Mental Hospitals play a key role in rehabilitation of the<br />
patients and is being widely recognized all over the world. This is an advanced way to<br />
prepare the mentally affected patient, psychologically and physically to meet the demands of<br />
his / her future occupational life in the society. This methodology particularly helps in case of<br />
chronically ill mental patient. Strengthening of Occupational therapy (O.T.) departments in<br />
Four Regional Mental Hospitals is being undertaken for rehabilitation of the patients<br />
recovering from mental disorders.<br />
Aims and Objectives<br />
1) To provide basic unskilled work to various types of mentally ill patients to keep them<br />
occupied in meaningful activities.<br />
2) To provide skilful work activities to the patients who are stable and have achieved some<br />
level of normalcy, so that they develop self - esteem, self- confidence and are well<br />
prepared for discharge from hospital.<br />
3) To Provide skilful activities through specific training to a selected group of patients to<br />
produce saleable products which will generate revenue so that patients can be given some<br />
incentives as an encouragement for their further progress in the society .<br />
4) To provide agro based activities to the selected ones which will help to utilize open<br />
cultivable land in the campus of RMHs, the product (crop or vegetable/ fruits) can generate<br />
revenue.<br />
5) To maintain innovative projects like bakery, cane baskets, carpentry, power loom,<br />
tailoring department, canteen facility for the patient by the patient assisted by staff<br />
members.
6) To maintain recreational activities, music therapy section, physical fitness section and<br />
others sports activities with the help of staff members so that patient - staff association and<br />
an emotional bond is created between them for an effective hospital management.<br />
7) To maintain “Day care centre” for continuation of rehab process in discharged as well as<br />
out patients to help them take part in various activities creating better job opportunities.<br />
Activities undertaken in 2011-12<br />
This task was achieved through up-gradation of occupation therapy department (for<br />
indoor patients), and establishment of Day care centers (for outdoor patients) through<br />
following activities.<br />
1. Appointment of skilled personnel<br />
Appointment of skilled personnel of following categories is being done at Pune, Thane,<br />
Ratnagiri & Nagpur Mental Hospitals on contractual basis by a committee under the<br />
chairmanship of Deputy Director Health Services, Pune, Thane & Nagpur Circle respectively.<br />
Table - Contractual skilled personnel for four Mental Hospitals<br />
Sr.No. Designation Pune Nagpur Thane R'giri<br />
Total man<br />
power<br />
1 Occupational Therapist 5 2 1 1 9<br />
2<br />
Tailor Cum Fashion Designer<br />
Instructor<br />
4 1 1 2 8<br />
3 Carpenter Instructor 1 1 2 1 5<br />
4 Weaver 3 1 4 8<br />
5 Screen printing Instructor 2 1 1 4<br />
6 Craft Teacher 4 3 1 8<br />
7 Yoga Teacher (Dance & Music) 2 2<br />
8 Marketing Coordinator/Executive 1 1 2<br />
9 Gardner 2 1 2 5<br />
10 Activity Bio product Data keeper 1 1 2<br />
11 Beauty parlor trainer 1 1<br />
12 Driver 1 1 2<br />
<strong>13</strong> Activity Assistance Staff 6 15 2 23<br />
14 Wielder 1 1<br />
15 Administration Manager 1 1<br />
16 Clinical Psychologist 1 1<br />
17 PSW 1 1<br />
18 Counselor 1 1<br />
19 Sales & Marketing Manager 1 1<br />
20 HR Manager 1 1<br />
178
Sr.No. Designation Pune Nagpur Thane R'giri<br />
Total man<br />
power<br />
21 Psychiatric Nurse 1 1<br />
22 Agriculture assistant 2 2<br />
23 Multi Purpose Vocational Instructor 1 21 1 23<br />
24 Rota Machine operator 1 1<br />
Total 33 15 54 11 1<strong>13</strong><br />
2. Procurement of Equipment<br />
Following Equipment are being procured centrally by procurement cell & by a committee at<br />
Regional Mental Hospitals following Government procurement guidelines.<br />
Sir<br />
No Name<br />
A Carpentry Section<br />
Table – Procurement of Equipment<br />
Quantity<br />
Pune N'pur Thane R'giri<br />
1 Wood Cutter 2 1 2 1<br />
2 Planner Machine (Randa Machine) 1 1 1 1<br />
3 Grinder Machine 1 1 2 1<br />
4 Drill machine 1 1 1 1<br />
5 Spray Painting machine 1 1 2 1<br />
6 Files(Flat & Round (50:50) 12 4 24 0<br />
7<br />
Files MARPHA (Flat & Round 6<br />
no.each)<br />
12 0 0 0<br />
8 Carpenter Table 0 0 2 2<br />
B Tailoring Section<br />
1 Sewing Machine, Heavy Duty 20 3 3 2<br />
2 Cloth cutter machine 4 2 2 0<br />
3 Storage Racks 4 0 0 0<br />
4 Pico machine 1 0 2 2<br />
5 Tailoring scissors 25 12 10 0<br />
6 Laundry Iron with Table 0 0 1 0<br />
7 Tailoring Cutting Table 0 0 2 2<br />
C Screen Printing<br />
1 Screen Printing machine 2 1 0 0<br />
D Craft Activities<br />
1 Paper Plate Making Machine 1 0 1 1<br />
2 Door Mat Making Machine(coir base) 1 0 0 0<br />
3 Envelope paper cutter 1 2 0 0<br />
E Physical Rehabilitation Unit<br />
179
Sir<br />
No Name<br />
Pune<br />
Quantity<br />
N'pur Thane R'giri<br />
1 Short wave Diathermy 2 1 1 0<br />
2 Shoulder Wheel 2 1 1 0<br />
3 Pedo cycle 4 1 1 0<br />
4 Static cycle with energy functions 6 1 1 0<br />
5 Lumbar traction 2 0 1 0<br />
6 wheel chairs 4 1 0 0<br />
7 walker 4 2 0 0<br />
8 Ultra Sonic 0 0 1 0<br />
9 Interferential Therapy 0 0 1 0<br />
10 Continuous Passive motion(U/L) 0 0 1 0<br />
11 Reaction Time 0 0 1 0<br />
12 Treadmills 0 0 1 0<br />
F Sports and Games Therapy<br />
1 Badminton Rackets 90 6 100 0<br />
2 Shuttle cocks 50 24 50Box 0<br />
3 Volleyball 40 6 40 0<br />
4 Carom boards 15 4 30 0<br />
5 Cricket bats 30 4 5 0<br />
6 Tennis ball 100 24 100 0<br />
G Library Facilities<br />
1 500 Books(on different Subjects) 500 500 0 0<br />
H Gardening Activity<br />
1 Water Jar 85 6 50 20<br />
2 Khurpya 85 24 0 20<br />
3 Fawada 34 4 30 10<br />
4 Kudal 40 4 30 10<br />
5 Tikaw 10 4 10 5<br />
6 Gardner Scissor 40 6 30 5<br />
7 Popat scissor 10 2 10 3<br />
8 Lawn machine 1 2 1 0<br />
9 Koyata 10 6 4<br />
10 Sarni/khurpi 10 12 10 3<br />
11 Water <strong>pip</strong>e 1000Ft. 6<br />
As<br />
required 100Ft.<br />
I Health Fitness Centre<br />
1 Roller Walker 6 0 0 0<br />
2 Lats Pully 2 0 0 0<br />
3 Twister 4 0 0 0<br />
180
Sir<br />
No Name<br />
Pune<br />
Quantity<br />
N'pur Thane R'giri<br />
4 Pect Deck 3 0 0 0<br />
5 Leg press 3 0 0 0<br />
6 Leg Ext./Curl 3 0 0 0<br />
7 Abking pro 4 0 0 0<br />
8 Dambells 20 0 20 0<br />
9 Cycle 4 0 0 0<br />
10 Yoga mats 125 0 0 0<br />
11 Stepper 2 0 0 0<br />
12 Theraballs 2 0 0 0<br />
<strong>13</strong> Bench Press 4 0 0 0<br />
14 Weight Cuffs 8 0 0 0<br />
J Day Care Centre<br />
1 Spiral Binding machine 1 0 1 0<br />
2 Lamination machine 1 0 1 0<br />
3 Comb binding machine 1 0 0 0<br />
K Leather Activity<br />
1 Leather Sewing machine 1 1 0 0<br />
2 Leather punching machine 1 1 0 0<br />
L Miscellaneous<br />
1 Computer with backup 10 4 15 3<br />
2 Printer and Scanner 4 4 0 0<br />
3 Printer and Scanner with Xerox 0 0 1 0<br />
4 Laser Jet Printer 0 0 2 0<br />
5 Computer Table 10 4 15 0<br />
6 Steel cupboard 22 10 25 3<br />
7 Digital Camera 1 0 0 0<br />
8 Handy cam 1 0 0 0<br />
9 DVD player with Speaker 3 0 1 1<br />
10 Speaker 0 0 10 0<br />
11 Television Set 6 3 1 1<br />
12 Water cooler 4 3 0 0<br />
<strong>13</strong> Showcase with Glass 2 3 3 1<br />
14 Notice Board 2 3 5 0<br />
15 Chair(Plastic) 120 120 100 20<br />
16 Activity Table 0 0 5 0<br />
17 Office Table 0 4 6 0<br />
18 Basic Musical Equipment set 0 0 1 Set 0<br />
19 Air Conditioner 0 0 3 0<br />
20 Assessment Bed() 0 0 4 0<br />
181
Sir<br />
No Name<br />
Pune<br />
Quantity<br />
N'pur Thane R'giri<br />
21 File Making Machine 0 1 0 1<br />
22 Welding Machine 0 1 0 0<br />
23 Rota Printing Machine 0 1 0 0<br />
24 Film making machine 0 0 0 1<br />
3. Provision of Raw material<br />
Raw material required for the Rehabilitation activities like handicrafts, screen printing,<br />
drawing, tailoring etc is being procured by the Regional Mental Hospitals following<br />
procurement guidelines and RKS approval<br />
4. Renovation and repairs of the existing structures<br />
Renovation and repairs to the Occupation Therapy department and Day care center of<br />
Regional Mental Hospitals is being undertaken by the public works department of<br />
Government of Maharashtra after technical approval by the engineering wing of State<br />
NRHM.<br />
5. Data automation with the help of hospital software.<br />
Computer software is being developed for updating the outdoor and indoor patients’<br />
record of Four Regional Mental Hospitals. This will help to track the patients for follow<br />
up.<br />
The project needs to be continued in <strong>2012</strong>-<strong>13</strong> for supporting the rehabilitation of indoor as<br />
well as outdoor patients recovering from mental disorders. Budget provision for following<br />
recurring activities will be required.<br />
1. Continuation of contractual staff<br />
2. Provision of Raw material<br />
3. Operational expenses for the State Mental Health Cell & 4 Regional Mental Hospitals<br />
4. Maintenance of Data Automation Software<br />
Budget Provision<br />
Sr.<br />
No<br />
Manpower on<br />
contractual basis<br />
Table – State level Monitoring Cell<br />
No. of<br />
staff<br />
Monthly salary Yearly Budget (Rs)<br />
1 Psychiatrist 1 Rs. 50,000/- 6,00,000/-<br />
2 Data Entry Operator 1 Rs. 10,000/- 1,20,000/-<br />
3 Office Stationery -- -- 50,000/-<br />
Sub Total 7,70,000/-<br />
182
Sr.No. Designation<br />
Table – Human resources for RHM Pune<br />
No of<br />
personne<br />
l<br />
Salary/person<br />
/month (in<br />
thousand Rs.)<br />
Rs. In Thousands<br />
Total<br />
salary for<br />
1 month<br />
183<br />
Budget<br />
for 1<br />
yrs.<br />
1 Occupational Therapist 5 15 75 900<br />
2<br />
Tailor Cum Fashion Designer<br />
Instructor<br />
4 5 20 240<br />
3 Carpenter Instructor 1 5 5 60<br />
4 Weaver 3 5 15 180<br />
5 Screen printing Instructor 2 5 10 120<br />
6 Craft Teacher 4 5 20 240<br />
7 Yoga Teacher (Dance & Music) 2 5 10 120<br />
8<br />
Marketing<br />
Coordinator/Executive<br />
1 15 15 180<br />
9 Gardner 2 5 10 120<br />
10 Activity Bio product Data keeper 1 5 5 60<br />
11 Beauty parlor trainer 1 5 5 60<br />
12 Driver 1 5 5 60<br />
<strong>13</strong> Activity Assistance Staff 6 5 30 360<br />
Sr.No. Designation<br />
Total 33 85 225 2700<br />
Table – Human Resource for RMH Thane<br />
No of<br />
personnel<br />
Salary/person<br />
/month<br />
Total<br />
salary<br />
for<br />
1 month<br />
Budget<br />
for 1<br />
yrs.<br />
1 Occupational Therapist 1 15 15 180<br />
2<br />
Tailor Cum Fashion Designer<br />
Instructor<br />
1 5 5 60<br />
3 Carpenter Instructor 2 5 10 120<br />
4 Weaver 4 5 20 240<br />
12 Driver 1 5 5 60<br />
<strong>13</strong> Activity Assistance Staff 15 5 75 900
Sr.No. Designation<br />
No of<br />
personnel<br />
Salary/person<br />
/month<br />
Total<br />
salary<br />
for<br />
1 month<br />
184<br />
Budget<br />
for 1<br />
yrs.<br />
15 Administration Manager 1 15 15 180<br />
16 Clinical Psychologist 1 15 15 180<br />
17 PSW 1 15 15 180<br />
18 Counselor 1 15 15 180<br />
19 Sales & Marketing Manager 1 15 15 180<br />
20 HR Manager 1 15 15 180<br />
21 Psychiatric Nurse 1 15 15 180<br />
22 Agriculture assistant 2 10 20 240<br />
23<br />
Multi Purpose Vocational<br />
Instructor<br />
21 5 105 1260<br />
Total 54 160 360 4320<br />
Sr.No. Designation<br />
Table – Human Resource for RMH Nagpur<br />
No of<br />
personnel<br />
Salary/person<br />
/month<br />
Total<br />
salary<br />
for<br />
1 month<br />
Budget<br />
for 1<br />
yrs.<br />
1 Occupational Therapist 2 15 30 360<br />
2<br />
Tailor Cum Fashion Designer<br />
Instructor<br />
1 5 5 60<br />
3 Carpenter Instructor 1 5 5 60<br />
4 Weaver 1 5 5 60<br />
5 Screen printing Instructor 1 5 5 60<br />
6 Craft Teacher 3 5 15 180<br />
7 Marketing Coordinator/Executive 1 15 15 180<br />
8 Gardner 1 5 5 60<br />
9 Activity Bio product Data keeper 1 5 5 60<br />
10 Wielder 1 5 5 60<br />
11<br />
Multi Purpose Vocational<br />
Instructor<br />
1 5 5 60<br />
12 Rota Machine operator 1 5 5 60<br />
Total 15 80 105 1260
Sr.No. Designation<br />
Table – Human Resource for RMH Ratnagiri<br />
No of<br />
personnel<br />
Salary/person<br />
/month<br />
Total<br />
salary<br />
for<br />
1 month<br />
185<br />
Budget<br />
for 1<br />
yrs.<br />
1 Occupational Therapist 1 15 15 180<br />
2<br />
Tailor Cum Fashion Designer<br />
Instructor<br />
2 5 10 120<br />
3 Carpenter Instructor 1 5 5 60<br />
4 Weaver 5 0 0<br />
5 Screen printing Instructor 1 5 5 60<br />
6 Craft Teacher 1 5 5 60<br />
7 Gardner 2 5 10 120<br />
8 Activity Assistance Staff 2 5 10 120<br />
9<br />
Multi Purpose Vocational<br />
Instructor<br />
1 5 5 60<br />
10 Rota Machine operator 5 0 0<br />
Total 7 60 65 780<br />
Sr. No.<br />
Name Of<br />
Material<br />
1 Envelop Paper<br />
2<br />
3<br />
4<br />
Seeds and<br />
Fertilizers<br />
Sanitary Napkin<br />
Raw Material<br />
Moti & Imitation<br />
Jewelry<br />
Raw Material for RMH Pune<br />
Quality Quantity Cost<br />
brown<br />
paper<br />
best seeds<br />
best<br />
cotton &<br />
paper<br />
workable<br />
5 Painting Material Durable<br />
6<br />
Utensil Washing<br />
Powder<br />
ISI Mark<br />
7 liquid Soap ISI Mark<br />
8 Shampoo ISI Mark<br />
9<br />
Cloth Washing<br />
Powder<br />
ISI Mark<br />
bundle as<br />
required<br />
as<br />
required<br />
as<br />
required<br />
as<br />
required<br />
as<br />
required<br />
as<br />
required<br />
as<br />
required<br />
as<br />
required<br />
as<br />
required<br />
Mode Of<br />
Procurement<br />
Time<br />
Line<br />
10000 Local market 1 mth<br />
10000 Local market 1 mth<br />
24000 Local market 1 mth<br />
36000 Local market 1 mth<br />
30000 Local market 1 mth<br />
250000 Local market 1 mth<br />
250000 Local market 1 mth<br />
100000 Local market 1 mth<br />
400000 Local market 1 mth
10<br />
11<br />
12<br />
Sr. No.<br />
Sr.<br />
No.<br />
1<br />
2<br />
3<br />
4<br />
Handkerchief<br />
and Scarves<br />
Embroidery Raw<br />
Material<br />
Tooth Powder<br />
Raw Material<br />
Name Of<br />
Material<br />
Drawing & Craft<br />
Material<br />
Raw Material for<br />
looms - Thread<br />
Agarbatti raw<br />
material<br />
Seasonal<br />
activities like<br />
Rangoli, Utane,<br />
workable<br />
coats<br />
material<br />
ISI Mark<br />
as<br />
required<br />
as<br />
required<br />
as<br />
required<br />
Total 1410000<br />
Raw Material for RMH Thane<br />
Quality Quantity Cost<br />
ISI Mark<br />
as<br />
required<br />
100000 Local market 1 mth<br />
100000 Local market 1 mth<br />
100000 Local market 1 mth<br />
Mode Of<br />
Procurement<br />
186<br />
Time<br />
Line<br />
200000 Local market 1 mth<br />
Std. 1000 kg 200000 Local market 1 mth<br />
Std.<br />
Std.<br />
5 Decorative laces Std.<br />
as<br />
required<br />
as<br />
required<br />
as<br />
required<br />
Raw Material for RMH Thane (continued)<br />
Name Of Material Quality Quantity Cost<br />
6 Electric welding rods Std.<br />
7<br />
8<br />
9<br />
10<br />
11<br />
Medicinal herbs and<br />
plants<br />
Sanitary napkin raw<br />
material<br />
Raw material for fabric<br />
and warli painting<br />
Raw material for<br />
decorative paper bags<br />
File making raw<br />
material<br />
Std.<br />
Std.<br />
Std.<br />
Std.<br />
coats<br />
material<br />
as<br />
required<br />
as<br />
required<br />
as<br />
required<br />
as<br />
required<br />
as<br />
required<br />
as<br />
required<br />
Total 1535000<br />
Raw Material for RMH Nagpur<br />
100000 Local market 1 mth<br />
500000 Local market 1 mth<br />
150000 Local market 1 mth<br />
Mode Of<br />
Procurement<br />
Time<br />
Line<br />
10000 Local market 1 mth<br />
25000 Local market 1 mth<br />
100000 Local market 1 mth<br />
100000 Local market 1 mth<br />
100000 Local market 1 mth<br />
50000 Local market 1 mth
Sr.<br />
No.<br />
1<br />
2<br />
3<br />
Name Of Material Quality Quantity Cost<br />
Screen printing<br />
material<br />
Basic material and<br />
threads for weaving<br />
dept.<br />
Raw material for<br />
Paper plate, door<br />
mats, envelop<br />
Std.<br />
Std.<br />
Std.<br />
4 Seeds and fertilizers Std.<br />
Sr.<br />
No.<br />
as<br />
required<br />
as<br />
required<br />
as<br />
required<br />
as<br />
required<br />
Total 800000<br />
Raw Material for RMH Ratnagiri<br />
Name Of Material Quality Quantity Cost<br />
Mode Of<br />
Procurement<br />
187<br />
Time<br />
Line<br />
20000 Local market 1 mth<br />
270000 Local market 1 mth<br />
450000 Local market 1 mth<br />
60000 Local market 1 mth<br />
Mode Of<br />
Procurement<br />
Time<br />
Line<br />
1 Electric welding rods Std. as required 10000 Local market 1 mth<br />
2 Decorative laces Std. as required 50000 1 mth<br />
3 Agarbatti raw material Std. as required 45000 Local market 1 mth<br />
4<br />
Seasonal activities like<br />
Rangoli, Utane, Rakhi<br />
Std. as required 175000 Local market 1 mth<br />
5 Drawing & Craft material Std. as required 150000 Local market 1 mth<br />
6<br />
7<br />
8<br />
File making raw material<br />
Raw material for<br />
Std. as required 50000 Local market 1 mth<br />
decorative paper bags<br />
Medicinal herbs and<br />
Std. as required 25000 Local market 1 mth<br />
other plantation Std. as required 20000 Local market 1 mth<br />
Budget requirement<br />
Total 525000<br />
Budget requirement for second phase of the project is as follows:
Table – Budget requirement for 2 nd Phase of Mental Health Project<br />
Implementing Unit<br />
HR<br />
Raw<br />
material<br />
Operational<br />
expenses<br />
Mental Health Cell DHS 7.20 0.00 0.50<br />
RMH Pune 27.00 14.10 0.50<br />
RMH Thane 43.20 15.35 0.50<br />
RMH Nagpur 12.60 8.00 0.50<br />
RMH Ratnagiri 7.80 5.25 0.50<br />
188<br />
Rs. In Lakhs<br />
Maintenance of<br />
Data<br />
Automation<br />
software<br />
A B<br />
10.00<br />
Sub-total 143.00 10.00<br />
Total (A+B) 153.00<br />
ACTIVITY : B.23.6.2 : LEPTOSPIROSIS PREVENTION AND CONTROL PROGRAM<br />
Introduction<br />
Due to rapid ecological changes during the past decade many zoonosis have emerged<br />
and resulted into epidemics causing significant morbidity and mortality in human beings.<br />
Leptospirosis is one of the diseases which predominantly occur in coastal region. The<br />
conditions that are required for maintenance and trans<strong>mission</strong> of the leptospirosis are the<br />
presence of saline soil, adequate moisture and reservoir / carrier hosts.<br />
Leptospirosis occurs as a result of amplification and trans<strong>mission</strong> of infectious agents.<br />
The severity of leptospirosis disease varies from mild to rapidly fatal. Mild forms are often<br />
misdiagnosed or ignored and severe forms are characterized by hepatic involvement, Acute<br />
Renal Failure and Hemorrhagic Syndrome. Early Case Detection, Accurate diagnosis,<br />
Appropriate and Timely treatment reduces the morbidity and mortality due to diseases.<br />
At present there is no control program for Leptospirosis in the country. As a New<br />
Initiative in the 11th five year plan a pilot project for prevention and control of Leptospirosis<br />
started in Gujarat, Kerala & Tamilnadu in 1st phase And Maharashtra &Karnataka in 2nd
Phase. In year 2011-12, The pilot project was implemented in Thane, Raigad, Ratnagiri and<br />
Sindhudurg costal districts of Maharashtra state.<br />
Govt. of India is not going to fund this project from year <strong>2012</strong>-<strong>13</strong>. Leptospirosis is one<br />
of the diseases that are monitored under IDSP program. As per the discussion in PIP Meeting<br />
held in Lonavala from year <strong>2012</strong>-<strong>13</strong> this project will be funded by NRHM.<br />
Problem statement -<br />
Thane, Raigad, Ratnagiri and Sindhudurg are the costal districts of Maharashtra state.<br />
Leptospirosis , zoonotic disease is endemic in this region but in the sporadic form. The cases<br />
previously diagnosed of leptospirosis in this region were seen of hepatic involvement. But in<br />
year 2010-11, the cases appeared in outbreak form with clinical course of disease changed<br />
showing the pulmonary involvement in patients leading to rapid death due to fast<br />
deterioration of patient.<br />
So Leptospirosis is the one of the major public <strong>health</strong> problem in these districts which<br />
has to be deal urgently.<br />
STATEMENT SHOWING INFORMATION OF LEPTOSPIROSIS CASES<br />
Year<br />
Sr.<br />
No.<br />
Districts / Corporation 2009- 10 2010- 11<br />
2011- 12<br />
(up to 4.02.12)<br />
A D A D A D<br />
1 Gr. Mumbai Corp. 448 38 271 17 125 6<br />
2 Thane 0 0 3 0 54 3<br />
3 Thane Corp. 0 0 0 0 2 0<br />
4 Mira-Bhayandar Corp. 5 0 0 0 2 1<br />
5 Navi Mumbai Corp. 0 0 0 0 5 0<br />
6 Kalyan Corp. 0 0 0 0 3 0<br />
7 Raigad 0 0 252 24 28 5<br />
8 Ratnagiri 14 0 26 6 <strong>13</strong>8 9<br />
9 Pune 10 1 10 0 0 0<br />
10 Kolhapur 5 0 0 0 0 0<br />
11 Sindhudurg 9 1 181 25 92 4<br />
12 Nagpur 0 0 3 1 0 0<br />
Total 491 40 746 73 449 28<br />
Note:- A = Attack, D =Death.<br />
189
Epidemiological Data for 2010-11 & 2011-12<br />
Sl.<br />
No<br />
.<br />
Name of<br />
district<br />
Suspecte<br />
d cases<br />
2010-11 2011-12<br />
Blood<br />
sample<br />
s<br />
tested<br />
Positiv<br />
e cases<br />
Death<br />
s<br />
Suspecte<br />
d cases<br />
Blood<br />
sample<br />
s<br />
tested<br />
Positiv<br />
e cases<br />
1 Thane 5 5 3 0 109 115 54 3<br />
2 Raigad 495 495 252 24 88 78 28 5<br />
190<br />
Death<br />
s<br />
3 Ratnagiri 124 124 25 6 <strong>13</strong>8 <strong>13</strong>9 <strong>13</strong>8 9<br />
4 Sindhudur<br />
g<br />
2029 1156 179 25 4101 4100 92 4<br />
Total 2653 1780 459 55 4436 4432 312 21<br />
Objectives:-<br />
To reduce morbidity and mortality due to leptospirosis.<br />
Strategies :-<br />
1) Early detection of Cases and identification & Strengthening of diagnostic laboratories<br />
• Identification of<br />
diagnosis services<br />
laboratories for strengthening leptospirosis<br />
• Training of Doctors,lab-technicians and paramedical staff in<br />
laboratory diagnostic technique.<br />
• Procurement of Kits.<br />
• Diagnostic facilities to make available up to PHCs with Eliza test<br />
facility at district hospital.<br />
2) Strengthening of patient management facilities.<br />
a) Development of trained manpower<br />
- Training of Medical and Paramedical personnel on various aspects on control of<br />
leptospirosis.<br />
b) Development of uniform guidelines.<br />
- Uniform guidelines to be formulated , printed and distributed to pilot areas.<br />
3) Intersectoral coordination<br />
- Intersectoral coordination meeting of Health, veterinary and Agriculture.<br />
4) IEC -to create awareness in the general public.<br />
- IEC material to developed and provided to create awareness in the general public in<br />
the form of posters, banners, board etc.
Financial Requirement for Leptospirosis:<br />
Sr. No.<br />
Financial Proposal for prevention & control of Leptospirosis (<strong>2012</strong>-<strong>13</strong>)<br />
Cash assistance required under NRHM Flexi fund<br />
Component<br />
(Sub- Component)<br />
Financial<br />
Requirement (Rs.<br />
in Lakhs)<br />
Functional head<br />
as per NRHM<br />
1 Training of MO and Staff 8.00 Flexi Fund<br />
2<br />
Laboratory Strengthening Activity<br />
1. leptospirosis diagnostic kits<br />
( Rapid test + Eliza kits)<br />
33.40<br />
2. Eliza reader and Washer<br />
25<br />
3 Medicine 43.50 Flexi Fund<br />
4 IEC 9.00 Flexi Fund<br />
5<br />
191<br />
Flexi Fund<br />
Referral transport by Ambulance- POL<br />
6.00<br />
Flexi Fund<br />
Total 124.90 Flexi Fund<br />
Statement showing the Budget requirement District-wise for year <strong>2012</strong>-<strong>13</strong><br />
for Leptospirosis Prevention And Control<br />
Sr.N<br />
o<br />
Name of<br />
District<br />
Component (Sub- Component )<br />
Laboratory<br />
Strengthening<br />
Traini<br />
ng of<br />
MO<br />
and<br />
Staff<br />
leptospir<br />
osis<br />
diagnosti<br />
c kits<br />
( Rapid<br />
test kits<br />
+<br />
Eliza<br />
Read<br />
er<br />
and<br />
Wash<br />
er<br />
Medici<br />
ne<br />
IEC Referral<br />
transport<br />
by<br />
Ambulan<br />
ce- POL<br />
Tot<br />
al<br />
(Rs in Lakhs)<br />
Allocati<br />
on<br />
from<br />
NRHM<br />
Flexi<br />
Fund<br />
Stat<br />
e<br />
Fun<br />
d
Eliza kits)<br />
1 Thane 2.00 11.90 10.00 11.75 0 0 35.6<br />
5<br />
2 Raigad 2.00 6.80 5.00 8.00 3.0<br />
0<br />
3 Ratnagiri 2.00 8.80 5.00 6.75 3.0<br />
0<br />
4 Sindhud<br />
urg<br />
2.00 5.90 5.00 17.00 3.0<br />
0<br />
192<br />
35.65 0<br />
0 24.8 24.8 0<br />
0 25.5<br />
5<br />
25.55 0<br />
6.00 38.9 38.9 0<br />
Total 8 33.4 25 43.5 9 6 124.<br />
9<br />
ACTIVITY : B.23.6.3 : PIP FOR STATE BUREAU OF HEALTH INTELLIGENCE AND VITAL<br />
STATISTICS<br />
124.9 0<br />
To strengthen all activities under this bureau, strong monitoring and evaluation is essential.<br />
Considering this aspect PIP for the year <strong>2012</strong>-<strong>13</strong> has been prepared. In this plan emphasis has<br />
been given on training, monitoring and evaluation, publication of various annual reports and<br />
printing of Birth and Death forms, conduction of statistical evaluation studies and building<br />
construction/renovation. Detailed plan of action is furnished below.<br />
1 Printing<br />
1.1 State Level<br />
1.1.1 For printing of annual reports: Civil Registration System , Survey<br />
of Causes of Death and Medical Certification of Causes of Death,<br />
expected expenditure Rs 1 ,00,000 has been proposed.<br />
1.1.2 Survey of causes of Death (Rural) Scheme is being implemented<br />
in one selected village of every primary <strong>health</strong> center. For the<br />
training of MO,ANM,MPW working under this scheme, printing<br />
of training modules and guidelines of the scheme Rs 2,00,000/- is<br />
proposed.<br />
1.1.3 Printing of Registration of Birth and Death Act 1969 booklet is<br />
proposed. Expenditure of Rs 25,000 is expected.<br />
1.2 District Level<br />
1.2.1 Printing of Birth and Death formats, form No 1 Birth reporting<br />
form, form no 2 Death reporting form, form no 3 Still birth
2 Monitoring and Evaluation<br />
reporting form, monthly summary report of Birth, Death and Still<br />
birth form no 11, 12 and <strong>13</strong> Rs. 32,41,200/- expenditure is<br />
needed.<br />
1.2.2 According to the directives from Government of India,<br />
Standardized birth and death certificates are to be issued to all<br />
<strong>rural</strong> units. For this printing of form no 5 (birth certificate) and<br />
form no 6 (death certificate) RS. 7, 18,880/- is proposed.<br />
1.2.3 Printing of Form no 4 and 4a under Medical Certification of<br />
Causes of Death to be provided to districts is essential for which<br />
Rs. 3,16,680/- is proposed.<br />
1.2.4 SCD scheme is implemented in all the Primary Health Centers.<br />
One village from each Primary Health Centre is selected under<br />
this scheme. Out of 1818 PHCs in the State 18<strong>13</strong> are working<br />
under this scheme. The information on Births, Deaths, Still Births<br />
and Causes of Deaths is collected every month by this office. It is<br />
the responsibility of this office to provide prescribed formats of<br />
reporting to the PHCs. For printing of these forms funds required<br />
budget is Rs. 11, 02,500/-.<br />
2.1.1 The data entry of Block level is expected to be done in newly<br />
developed software by NIC Pune. For this purpose new Server for<br />
HIVS Bureau is required. Rs. 5, 00,000/- is the expected<br />
expenditure.<br />
2.1.2 a) Under Survey of causes of Death scheme®, for ascertaining<br />
cause of death, two physician per district will be authorized and<br />
they will be expected to ascertain every cause of death under<br />
this scheme in their district. An honorarium of Rs. 25/- per<br />
physician per death is planned. For this RS. 11, 50,000/-<br />
expenditure is expected.<br />
b) Under SCD scheme Health worker (M/F) are required to visit<br />
fortnightly to the selected village for collecting sign and<br />
symptoms of deceased before death from their relative. Hon. Of<br />
Rs 25/- per death to <strong>health</strong> worker is proposed. For 2300 deaths<br />
under SCD scheme Rs. 5, 75,000 are proposed.<br />
2.1.3 a) Appointment of one programmer is need for NIC developed<br />
software for taking output of various combinations of variables<br />
under civil registration system. Estimated expenditure of Rs 1,<br />
193
3 IEC<br />
4 Training<br />
2.1.4 Deleted<br />
80,000 /- is needed for contractual appointment of one<br />
Computer (software) programmer in the financial year <strong>2012</strong>-<strong>13</strong><br />
for a period of nine months.<br />
b) Data entry of Birth and death registration of urban units is<br />
done at State level at HIVS bureau. On an average data entry of<br />
10 lakh urban births and 3.5 lakh urban deaths are expected per<br />
year. As existing staff is not able to complete the data entry in<br />
stipulated additional manpower is required. Hence, appointment<br />
of 10 data entry operators is proposed. For this financial<br />
assistance of Rs. 8, 64,000/- is required for a period of<br />
nine months.<br />
2.1.5 For statistical analysis of Medical Certification of Causes of<br />
Death, software needs to be developed. Rs. 1, 00,000/- is<br />
expected for this purpose.<br />
2.1.6 Deleted<br />
3.1.1 IEC plays an important role in giving information to various<br />
provisions under this act to public at large. Coverage of Death<br />
registration appears to be low due to non registration of deaths<br />
under 6 years of age. Focus of IEC on registration of deaths under<br />
6 years of age is the need of hour. Rs. 6, 60,000/- expenditure is<br />
required for this publicity.<br />
4.1.1 Under civil registration events like Births, Deaths and Still Births<br />
that occur are filled in prescribed forms. On the basis of this<br />
forms various statistical tables are generated which are used for<br />
future planning purpose. NIC, Pune has developed software for<br />
data entry of these forms. Training at block level is proposed for<br />
which an amount of Rs. 3, 76,000/- is required.<br />
4.1.2 To ascertain the causes of death under SCD scheme, training of<br />
three selected / authorized physicians per district is proposed.<br />
For these 4 batches, State level TOT will be conducted. 100<br />
participants will be trained. This will require budget of Rs. 1,<br />
194
40,000/-.<br />
Total budget required for HIVS is Rs. 102.5 Lakhs<br />
ACTIVITY : B.23.6.4 : IDSP ADDITIONAL BUDGET FROM NRHM MISSION FLEXIPOOL<br />
1. Procurement of Lab equipment for District Priority Lab Nashik/Beed –<br />
(Proposed in District PIP)<br />
Under IDSP, GoI has planned to develop 50 District Priority Labs in entire country.<br />
Two of these DPL labs are from the State, District Hospital Lab Nashik & Beed. Though under<br />
IDSP these labs have received some of important lab equipment, as per district’s request there<br />
is requirement of other deficient equipment which should be procured on priority to develop<br />
these labs as Public Health Labs. DPL Nasik has proposed Rs. 20 Lakhs under additionalities<br />
in its' District PIP.<br />
3. Developing State IDSP Cell:-<br />
At present, State IDSP Cell is situated at Joint Director of Health Services<br />
Office, New Central Building, Pune -1. As per the norm, six contractual staff positions are<br />
approved at State IDSP Cell but the present accommodation of the Cell is inadequate &<br />
congested. New State IDSP Cell can be developed at Vishrantwadi Office. For new proposed<br />
office infrastructure, project requires Rs. 10.00 Lakhs from NRHM <strong>flexipool</strong>.<br />
4. EPIDEMIC PREPAREDNESS:- Workshop for Rapid Response<br />
Teams:-<br />
• Aim :- Capacity building of concerned officers regarding epidemic<br />
Preparedness & outbreak investigation.<br />
Table( N):-<br />
• Training Load:-<br />
State RRT 6 Officers 06<br />
DSO 1 /District 033<br />
RRT 4 /District <strong>13</strong>2<br />
DMO 1/ District 33<br />
195
Surveillance Officers of<br />
municipal Corporations<br />
In charge of District<br />
Public Health Lab<br />
1/ corporation 23<br />
1/ DPHL 30<br />
Total 247<br />
• Technical Committee For Workshop:-<br />
Jt.Director, of Health Services (MF&WBD)<br />
Jt.Director of Health Services (TB/Leprosy)<br />
Deputy Director, State Public Health Lab<br />
Faculties from PSM, Medicine, Pediatrics & Microbiology department.<br />
Principal HFWTC<br />
Epidemiologists HFWTC<br />
Senior Training Consultant, NRHM<br />
State Surveillance Officer, IDSP<br />
• Topics to be covered:-<br />
1. Fundamentals Disease surveillance<br />
2. Case Definitions of epidemic prone diseases<br />
3. Role of laboratories in disease Surveillance<br />
4. Lab sample collection & Transportation.<br />
5. Generating early warning signals (EWS)<br />
6. Outbreak - Definition, Triggers, management, investigation<br />
7. Epidemic preparedness<br />
8. Analysis of disease surveillance & outbreak data.(Data management)<br />
9. Community involvement & media management<br />
• Duration of Workshop -- 3 days<br />
• One Workshop at every division (Total 8 Workshops) 30 participants /<br />
Workshop.<br />
Table( O):-<br />
• Estimate of Expenditure:-<br />
Sr.No. Particulars Amount<br />
1 TA of participants Rs.1000/participants Rs.30,000/-<br />
2 DA Rs 500/day/participant Rs.45,000/-<br />
3<br />
Rs.1500/participants<br />
Tea & Food Rs 300/participant/day Rs.27,000/-<br />
196
4 Training material Rs 200/participant Rs.6,000/-<br />
5 Honorium to Faculties Rs 1000/Lecture x Rs.12,000/-<br />
12<br />
6 Miscellaneous Expenses Rs.10,000/-<br />
Total Rs.1,30,000 X 8 Rs.10,40,000/-<br />
Total budget required for IDSP support is Rs. 40.40 Lakh<br />
ACTIVITY : B.23.6.6: SUPPORT REQUIRED FOR ROUTINE IMMUNIZATION<br />
1) Construction of Regional / District Vaccine & Cold Chain Store (RVS)/(DVS) –<br />
As per EVM Suggestions there must be standard RVS / DVS for proper storing of<br />
vaccines & suitable working room for cold chain technician at regional & district / MC<br />
level. GOI has approved the model plan for RVS/DVS as per WHO norms. Post of cold<br />
chain technician is sanctioned to every district but there is no provision for office and<br />
the space required for keeping the tools, spare parts etc. and creating environment for<br />
suitable working place. Construction of one room for cold chain technician will solve the<br />
problem of inadequate space and will facilitate the functioning of cold chain. It is<br />
therefore proposed to sanction Rs. 80,27,523/- (Received proposals of district Nasik @<br />
Rs 3377523/- & Bhandara @ Rs 4650000/- from district infrastructure NRHM section. )<br />
2) Contractual appointments of Cold- Chain Technicians - Presently 34 cold chain<br />
technicians’ posts are sanctioned at district level. Out of 35 districts 12 districts are<br />
geographically large and having large number of institutions having ILR/DF facility.<br />
It is very difficult for 1 cold chain technician to attend all the calls within time. Also<br />
fourteen districts are having corporation area within them. For this purpose the<br />
identified districts need additional cold chain technician on contract basis for smooth<br />
functioning EVM assessment recommendation. To fill the vacant post , the districts<br />
identified are BMC(2), Thane, Aurangabad, Nasik, Pune, Ahmadnagar, Nagpur,<br />
Solapur, Nanded, Kolhapur, Amravati, Jalgaon (Total - <strong>13</strong>).Also 12 posts of cold chain<br />
technicians are vacant. Hence it is proposed to sanction 25 posts of cold chain<br />
technicians for next year. The proposed honorarium is Rs. 12000 per month on<br />
contract basis. Proposed essential qualification for these posts is ITI & NCTVT<br />
Refrigeration/Air Conditioning. The proposed activity is new & may take 2 months<br />
for sanction and appoint of these technicians Hence the honorarium is proposed for<br />
197
only 10 months. The expenditure required for this activity Rs. 30.00 lakh<br />
(12000x10x25). The activity was proposed under NRHM additional ties in last year but was<br />
not sanctioned.<br />
3) Contractual appointment of Pharmacist - In the State WIC and WIF facility is<br />
available at State head quarters and at present handling of vaccines & distribution is<br />
done by Health Supervisor/Health Assistant.. EVM assessment has recommended<br />
appointment of pharmacist at state vaccine store. Presently the post of pharmacist at<br />
State head quarter is not sanctioned. The pharmacist is required for handling vaccine,<br />
distribution and keeping inventory control. For this purpose appointment of 1<br />
Pharmacist on contract basis @ Rs. 15,000 per month is proposed on contract basis.<br />
Proposed essential qualification for this post is B-Pharmacy with computer literacy .<br />
The budget required will be Rs 1.80 Lakhs (15000x12x1). The activity was proposed under<br />
NRHM additionailties in last year but was not sanctioned.<br />
WIC/ 5, [[<br />
4) WIC/WIF Maintenance - There are 16 WIC & 5 WIF working in the State at<br />
various 11 places like State/Divisional/District headquarters. These places<br />
require budget for maintenance which is not available under RI PIP. Generator<br />
repairs, POL for generator and minor repair is needed at these places to maintain<br />
cold chain for 24 Hrs. There is Load shedding at regional level 5 to 10 Hrs approx<br />
at regional level. It is proposed to sanction Rs. 1 lakh per year for WIC/WIF<br />
maintenance at 11 places. The budget proposed Rs. 1.00 x 11 = 11.00 lakhs. The<br />
activity is newly proposed under RI PIP in last year but was not sanctioned.<br />
5) Spare parts for cold chain maintenance - The supply for spare parts required for<br />
maintaining cold chain equipments is not regular. As per Govt. of India guidelines<br />
cold chain sickness rate should be less than 2%. The budget is proposed to procure<br />
essential and fast moving spare parts at State level and to distribute in time to<br />
regional and district level to repair breakdown equipments. It will help state to<br />
reduce breakdown percentage and reduce down time. Ultimately it will maintain<br />
potency of vaccine. For this activity proposed budget is Rs. 20 lakhs. The activity<br />
was proposed under RI PIP in last year but was not sanctioned. Hence this year proposed<br />
under NRHM additionalities .<br />
6) Wireless data logger- (State Hq vaccine store )<br />
Maharashtra is among 10 states which have been recommended by MOHFW and<br />
UNICEF where the loggers are introduced. For installation of this system dedicated<br />
198
oad band internet connection with STATIC / fixed Global IP address is required.<br />
BSNL offers this type of connection ( Fi Bro 1 (1 MBPS Speed, unlimited download,<br />
one static IP) costs 2999 /- per month as fixed monthly charges.) Hence the operational<br />
cost is Rs. 2999 X 12 = 35988. The activity is implemented in last year and the<br />
wireless data loggers started working online from 27 th Nov. 2011 onwards. The data<br />
logger is monitoring temperature of cold room on 24X7 basis with readings every 30<br />
minutes. This will help in improving cold chain capacity of the state. The activity was<br />
proposed under RI PIP in last year but was not sanctioned. Hence this year proposed under<br />
NRHM additional ties.<br />
7) Wireless data logger- (Regional Hq vaccine stores )<br />
At 8 regional level & 2 district level e.g. Chandrapur & Parbhani there are 14<br />
WIC & 3WIFavailable, EVM assessment recommendation / suggestion is that provide<br />
wireless data loggers facility to all WIC/WIF The outcome of the activity will be<br />
monitoring of the temperature of cold room on 24X7 basis with readings every 30<br />
minutes. This will help in improving cold chain capacity of the state For installation of<br />
this system dedicated broad band internet connection with STATIC/ fixed Global IP<br />
address is required. BSNL offers this type of connection (FiBro 1 (1 MBPS Speed,<br />
unlimited download, one static IP) costs 2999 /- per month as fixed monthly charges.)<br />
Hence the operational cost is Rs. 2999 X 12X17 =Rs. 611796/-,<br />
Also requires (one dedicated computer, printer, UPS, Internet connection etc.)<br />
approx cost @Rs. 50000/-X10 V.S.=Total approx cost Rs.5.00 Lakh.<br />
Approx. cost of (each Data logger, Software, Receiver, Router etc)@Rs50000/- X17<br />
WIC/WIF.=Total approx cost Rs.8.50Lakh.<br />
Total budget proposed is activity Rs. 1961796/- i.e. approximately 20.00 lakhs.<br />
8) Retrofitting of CFC WIC into Non CFC- (Regional /District Hq vaccine stores )<br />
At 4 regional level e.g. Nasik, Aurangabad, Akola, Kolhapur & 2 district level<br />
e.g. Chandrapur & Parbhani there are 6 WIC working on CFC units, EVM assessment<br />
recommendation / suggestion is that retrofit CFC units into Non CFC units The<br />
outcome of the activity will be replacement of CFC units. Approx. cost of retrofitting is<br />
@Rs. 100000/- X 6WIC X 2Units = Total Cost Rs 12 Lakh.<br />
9) Alarm & Hooter System for WIC/WIF - (State/Regional /Dist. Hq vaccine store )<br />
There are 16 WIC & 5 WIF working in the State at various 11 places like<br />
State/Divisional/District HQ,EVM assessment recommendation / suggestion is that these<br />
199
WIC/WIF requires Alarm & Hooter System. The outcome of the activity will be extra<br />
attention for handlers & safety of vaccines. Approx. cost of retrofitting is @Rs. 25000 X 16 WIC<br />
X 5 WIF= Total Cost Rs 5.25 Lakh.<br />
Total Budget: 180.33<br />
ACTIVITY : B.23.7: Hematology Program<br />
Hemophilia and Thalassemia are inherited blood disorders and have no cure, hence<br />
they are included together in this program.<br />
Hemophilia is a group of genetic bleeding disorders in which the body’s ability to<br />
control coagulation is impaired. It is caused by the absence of certain clotting factors in the<br />
blood. Prolonged bleeding may occur after trauma or sometimes spontaneously. Prolonged<br />
bleeding in the brain or inside joints can be fatal or permanently debilitating. It affects almost<br />
only males. Hemophilia is a lifelong incurable disorder but it can be managed by repeated<br />
blood component therapy. Hemophilia cannot be prevented. Genetic counseling,<br />
identification of carriers through molecular genetic testing, and prenatal diagnosis are<br />
available to help individuals understand their risk of having a child with hemophilia. Education<br />
and timely treatment is essential for this disease.<br />
Hemoglobin is the protein that enables red blood cells to carry oxygen. Thalassemia is<br />
a hereditary hemoglobin disorder. In Thalassemia reduced quantities of hemoglobin is<br />
produced. This is associated with severe anemia with rupture of the red blood cells.<br />
Thalassemia major is a serious disease in which the child becomes dependent on blood<br />
transfusions. Since there are no detailed epidemiological studies; it is not possible to predict<br />
the prevalence of Thalassemia in Maharashtra. Identification of carriers and sufferers is<br />
necessary, giving emphasis on <strong>health</strong> education and marriage counseling to prevent this<br />
disease in the next generation.<br />
Objectives of the hematology program<br />
Objectives of the hematology program are as follows:<br />
• Capacity building of all <strong>health</strong> functionaries for example MO, ANM, MPW, ASHA etc.<br />
• Strengthening of diagnostic and treatment centers<br />
• Strengthening supportive departments like blood bank and establishment of<br />
physiotherapy center<br />
• Provision of technical manpower<br />
• To create awareness in the community about these diseases<br />
200
The program will be implemented through the establishment of Hematology Centers at 4<br />
districts. Diagnosis, treatment and support services will be provided and the centers will be<br />
integrated with Rajiv Gandhi Jeevandayee Arogya Yojana for further specialized treatment.<br />
Activities planned for <strong>2012</strong>-<strong>13</strong><br />
Activities planned for the year <strong>2012</strong>-<strong>13</strong>are as follows:<br />
• It is proposed to establish 4 Hematology Centers:<br />
Table - Centers identified<br />
Sr. District Center<br />
1 Nagpur Women’s Hospital<br />
2 Amravati District Hospital<br />
3 Pune Sassoon General<br />
Hospital, B.J.M.C.<br />
4 Nashik District Hospital<br />
• However these districts are tentative and may be changed depending on availability of<br />
technical manpower.<br />
• Existing <strong>health</strong> infrastructure in 4 districts:<br />
Sir District PHC RH/SDH MO ASHA<br />
1 Nagpur 58 11 122 1688<br />
2 Nashik 103 28 115 3532<br />
3 Amravati 56 <strong>13</strong> 87 2068<br />
4 Pune 96 24 204 3293<br />
Total 3<strong>13</strong> 76 528 10581<br />
• Provision of trained technical manpower to all 4 centers as well as manpower at<br />
district and state level for monitoring and evaluation.<br />
Physician, Pediatrician and Pathologist should be taken from existing staff.<br />
This is a new initiative which is to be implemented for the first time in<br />
Maharashtra with the help of the Government of India. As this is a new initiative it is<br />
strongly recommended to appoint Hematology co-ordinators in the districts to<br />
monitor the program. Monitoring will include data collection as per the population,<br />
the patients as well as Hematology Program personnel. In the initial stages coordinators<br />
will implement and manage the program as a separate entity in the district.<br />
They will also be responsible for monitoring the effective training of all the personnel<br />
in this program.<br />
201
Medical officer may not be appointed at state level. However, one<br />
program officer and one program assistant should be appointed at state level.<br />
State level personnel will be responsible for monthly reporting and effective program<br />
implementation. New patients of Thalassemia and Hemophilia will be issued ID cards<br />
prepared in co-ordination with district and State level and central data base will be<br />
maintained. They will also be responsible for forwarding names of beneficiaries with<br />
income less than Rs. 150000/- per annum to Rajiv Gandhi Jivandai Arogya Yojana.<br />
These responsibilities cannot be given to the existing staff. Budget has been adjusted<br />
accordingly including TA/DA of state level personnel.<br />
Table - Manpower required for Hematology Center<br />
Sr. Center Sr. Post No. of<br />
Unit<br />
1 Hematology<br />
Center<br />
Unit<br />
cost<br />
202<br />
Rs. In Lakhs<br />
Amount<br />
1 Physician 4<br />
2 Pediatrician 4<br />
3 Pathologist 4<br />
4 Medical Officer (MBBS) 8 1.80 14.40<br />
5 Hematology Technician 4 0.60 2.40<br />
6 Counselor 4 0.60 2.40<br />
7 Staff Nurse 4 0.60 2.40<br />
8 Physiotherapist 4 1.20 4.80<br />
Total 26.40<br />
2 District level 1 Salary and TA/DA of Hematology<br />
Coordinator<br />
4 0.87 3.48<br />
Total 3.48<br />
3 State level 1 Salary of Hematology Program<br />
Officers<br />
1 1.44 1.44<br />
2 Salary of Hematology Program<br />
Assistants<br />
1 0.58 0.58<br />
3 Contingency for TA/DA of<br />
Medical Officer and Hematology<br />
Program Officers<br />
- 0.20 0.20<br />
4 Total 2.22<br />
Grant Total 32.10<br />
• Services to be offered at the Hematology center are as follows:<br />
1. Laboratory services for diagnosis of all three diseases<br />
2. Treatment of these diseases
3. Day care facilities including investigation, examination by all specialists, blood<br />
transfusion etc.<br />
4. Supportive services such as dentist, physiotherapy etc.<br />
5. Health education and counseling including genetic counseling for those in the<br />
marriage and reproductive age group<br />
• Investigations to be offered at Hematology Centre Laboratory are as follows:<br />
Table – Test to be performed<br />
Sr. Test<br />
1 Hb, CBC with RBC indices<br />
2 Peripheral Smear<br />
3 Hemolytic profile 1 NESTROFT for Thalassemia<br />
2 Reticulocyte Count<br />
4 Hb. Electrophoresis for Thalassemia<br />
5 HPLC<br />
6 Coagulation profile for Hemophilia 1 PT-INR<br />
2 aPTT<br />
3 Mixing studies-for inhibitor<br />
patients.<br />
4 Factor assay<br />
• Equipment and budget required is as follows:<br />
Table –: Equipment and Budget required for routine Hematological workup<br />
Sir Equipment Unit cost No. of units<br />
Rs. In Lakhs<br />
Budget required<br />
1 Cell Counter - 3 part 3.50 2 7.00<br />
2 Microscope binocular 0.30 4 1.20<br />
3 Electrophoresis machine 0.60 4 2.40<br />
4 Purchase of Reagents for 1.00 4 4.00<br />
above tests<br />
Total 14.60<br />
203
Table –: Equipment Budget required for diagnosis of Hemophilia<br />
Rs. In Lakhs<br />
Sir Equipment Unit cost No. of units Budget required<br />
1 Semi-automated coagulometer 5.00 4 20.00<br />
2 Centrifuge Machine 0.20 4 0.80<br />
3 Water bath for incubation 0.50 4 2.00<br />
4 Reagents 0.50 4 2.00<br />
Total 24.80<br />
Table –:Budget required for diagnosis of Thalassemia<br />
Rs. In Lakhs<br />
Sir Equipment Unit cost No. of units Budget required<br />
1 HPLC Machine only Nashik (to be<br />
purchased at State level)<br />
35.00 1 35.00<br />
2 Reagent 2.00 4 8.00<br />
Total 43.00<br />
Table –: Additional Budget required<br />
Sir Particulars Unit cost No. of<br />
Rs. In Lakhs<br />
Budget<br />
units required<br />
1 Laboratory consumables 0.50 4 2.00<br />
2 Laboratory renovation 1.0 4 4.00<br />
3 Essential Medicines 0.50 4 2.00<br />
4 Support to Blood Bank 1.00 4 4.00<br />
5 Establishment of Physiotherapy Centre 1.50 4 6.00<br />
6 Establishment for Day Care Centre/up<br />
gradation (min 4 beds)<br />
1.00 4 4.00<br />
7 Contingency for equipment, stationery,<br />
consumables, up gradation, repair etc<br />
1.50 4 6.00<br />
Total 28.00<br />
• Hemophilia is treated by replacement of coagulation factors<br />
204
Sr. Factor<br />
Table –: Annual budget required for Factors for Hemophilia patients<br />
No. of<br />
patients<br />
Annual<br />
requirement of<br />
factor/patient<br />
(Units)<br />
1 VIII 200 10000<br />
2 IX 60 10000<br />
3 FEIBA 12 10000<br />
Total<br />
requirement<br />
factor/annum<br />
(Units)<br />
2000000<br />
600000<br />
120000<br />
Price or<br />
unit of<br />
Factor<br />
(Rs.)<br />
205<br />
Rs. In Lakhs<br />
Total<br />
Amount<br />
(Rs.)<br />
9 180.0<br />
16 96.00<br />
40 48.00<br />
Total 324.00<br />
Sr.<br />
No.<br />
• Training will be provided to <strong>health</strong> functionaries in all 4 districts and intensive training<br />
will be provided to hematology center staff<br />
Category of<br />
OFFICERS/STAFF<br />
1 Specialist<br />
(Physician,<br />
pediatrician,<br />
pathologist<br />
2 MBBS MOs at<br />
Hematology<br />
center/<br />
3 Support staff of<br />
Hematology<br />
center<br />
4 Medical officers of<br />
PHC/RH/SDH<br />
5 ASHA(Workshop)<br />
Total<br />
training<br />
load<br />
No. of<br />
days<br />
Total<br />
batches( Per<br />
batch 30<br />
participants)<br />
Rs. In Lakhs<br />
Expected<br />
Budget for<br />
one batch<br />
Total<br />
expected<br />
budget<br />
12 10 1 2.07 2.07<br />
9 10 1 2.07 2.07<br />
16 5 1 1.03 1.03<br />
528 1 18 0.21 3.73<br />
10581 1 0 0.00 10.58
Total Budget<br />
• IEC materials will be provided at all PHC/RH/SDH/DH and Hematology Centers<br />
Table –: IEC<br />
20.6 19.47<br />
Sir IEC<br />
Unit cost No. of units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
1 IEC 0.03 393 11.79<br />
Total 11.79<br />
ASHAs will provided IEC to Gram Sabha, 4 sessions per year. For this ASHA will be given<br />
incentive at the rate of Rs. 50/- per session which has been budgeted under General incentive<br />
for ASHAs.<br />
As this is a combined program for Hemophilia and Thalassemia, depending on the number of<br />
patients for each disease, the budget may be interchanged and utilized from different heads<br />
for diagnosis, treatment and IEC as required.<br />
Table- : Summary of Budget Requirement – HEMATOLOGY Program<br />
206<br />
Rs. In Lakhs<br />
Sir Level Budget required<br />
1 Manpower required for Hematology Center 32.10<br />
2<br />
Equipment and Budget required for routine<br />
Hematological workup<br />
Equipment Budget required for diagnosis of<br />
14.60<br />
3 Hemophilia 24.80<br />
4 Budget required for diagnosis of Thalassemia 43.00<br />
5 Additional Budget required<br />
Annual budget required for Factors for Hemophilia<br />
28.00<br />
6 patients 324.00<br />
7 Training 19.47<br />
8 IEC 11.79<br />
Total 497.76
B.23.8 SHORT TERM CERTIFICATE COURSES FOR MEDICAL OFFICERS IN PUBLIC<br />
HEALTH DEPARTEMENT<br />
INTRODUCTION<br />
Public Health Department has a good network of <strong>health</strong> institutions which delivers basically primary &<br />
secondary <strong>health</strong> care. Primary <strong>health</strong> care is provided by sub centers & primary <strong>health</strong> centers. For<br />
secondary care there are Rural Hospitals which have 30 beds & are expected to provide specialty<br />
services in three specialties. There are 50 bedded & 100 bedded Sub District Hospitals with<br />
respectively five and eight specialties. At district level there are District Hospitals with fourteen<br />
specialties.<br />
To provide specialty care at these hospitals specialist posts are created. In addition to these regular<br />
posts there is provision of appointing specialists on contractual basis with laid down terms &<br />
conditions.<br />
OBJECTIVE<br />
At the end of training course Medical Officer should be able to deliver effective medical care following<br />
appropriate current medical practices in defined specialilty like Medicine, Pediatrics, Anesthesia,<br />
Psychiatry etc.<br />
NEED FOR SHORT TERM TRAINING COURSES<br />
• Presently proportion of vacancies in the specialities like Pediatrics, Medicine & Anesthesia is<br />
about 60%<br />
• Specialists are not willing to join <strong>rural</strong> areas although appointed by the department due to<br />
various reasons like payment, basic amenities, lack of education facilities etc.<br />
• Those who join the department are not continuing & proportion of leaving the job is<br />
significant.<br />
• Necessary infrastructure has been developed at hospital level however it is not optimally<br />
utilized due to shortage of specialists.<br />
• Requirement & availability of specialists is as below:<br />
o Total posts of specialists sanctioned: 511<br />
o Out of that posts filled: 144<br />
o Total number of vacancies: 367<br />
Therefore to fulfill the requirement of department of providing appropriate specialty services it is<br />
proposed to start short term training courses in all required specialties initially this will cover<br />
Pediatrics & Medicine & in due course other subjects will be included as per need. In addition to this<br />
training will also be imparted to MOs & some paramedical staff in disciplines like Bio chemistry,<br />
Microbiology & Radiology.<br />
METHODOLOGY<br />
• It is proposed to appoint Dr Mrudula Phadke as a Training Consultant (Chairperson) for<br />
planning, implementation of these training courses.<br />
207
• It will be a certificate course & the certificate will be given by the Directorate of Health<br />
Services & this will be only for working in the <strong>health</strong> facilities of <strong>health</strong> department & not for<br />
general practice outside the department.<br />
• Trainees: These will be identified MBBS Medical Officers who are already working in the<br />
department & are willing to work at least for five years in the department after completion of<br />
training course. MOs will be deputed for this training course either at identified Medical<br />
College or District Hospital for 6 months. These identified MOs need to be given incentive in<br />
the form of priority for PG diploma or degree courses & also preference in posting.<br />
• Duration: It will be six months.<br />
• Curriculum: This will be prepared as per the requirement of the department based on the<br />
clinical services expected to be delivered at the respective hospital level. This will be<br />
developed by the experts in the corresponding field.<br />
• Training methodology: this will cover.<br />
o Training lectures to cover theoretical aspects by videoconference.<br />
o Theory of practical<br />
o Hands on training in the wards of Medical Colleges & DHs<br />
o Journal club, clinics, case presentation, seminars & etc<br />
o Theory & practical examination during the training the training period & at the end of<br />
course.<br />
o MOs will attend theory lectures in morning session by videoconference method & in the<br />
afternoon will work in wards, will attend journal/ case presentation/ seminars etc. either<br />
in Medical College or in DHs as orders given.<br />
o In addition to this, there will be three contact programs in which all trainees will have<br />
class room lecture session.<br />
• Training place: Training will be given at following sites depending on the availability of trainers<br />
and also clinical cases:<br />
o Medical Colleges both government & private as per willingness. Consent of Medical<br />
Education department needs to be taken for the same.<br />
o District hospitals: Initially few DHs like Nasik, Ahmad nager will be included as training<br />
places & after evaluating their usefulness additional DHs will be covered.<br />
o Private hospitals<br />
• Trainers: Trainers & resource persons will be identified by the consultant, form Medical<br />
Colleges and also private practitioners. They will be identified based on their experience,<br />
expertise & most important will be willingness to work.<br />
• Training material: Training Material will be developed by experienced teaching faculties/<br />
experts in that field & will be distributed to all the trainee Medical Officers.<br />
BUDGET<br />
Budget for each will be required for various activities as below:<br />
208
A. Training expenditure<br />
No Activity Rate Budget<br />
in lac<br />
1. Preparation of training curriculum, listing of essential Rs. 1 lac per training Rs. 1.0<br />
skills, time table etc<br />
course<br />
2. Remuneration for trainers<br />
a. For theory sessions (there will be about 5-10 trainers. Rs. 5000 for each Rs. 12.0<br />
They will take one session per week. Total 24 sessions session* 24 sessions* 10<br />
of each trainer)<br />
trainers<br />
b. For practical & hands on training (There will be about 5- Rs. 10,000 per month* Rs. 7.20<br />
12 trainers from local district.)<br />
12 trainers* 6 months<br />
3. Contingency funds for printing training material,<br />
conduct of examination etc.<br />
- Rs. 5.0<br />
4. Office expenses for consultant Rs. 50,000 per month Rs. 3.0<br />
TOTAL Rs. 30.20<br />
B. Video Conferencing expenditure<br />
No Activity Rate Budget in lac<br />
1 Facility of video conferencing - Rs. 10.0<br />
TOTAL Rs. 10.0<br />
ACTION EXPECTED TO BE TAKEN<br />
• Approval of the proposal by Government & appointing Chairperson Dr. Mrudula Phadke<br />
& also designate one senior officer from the Directorate as Chief coordinator.<br />
• Development of videoconference facility in Mumbai at Directorate of <strong>health</strong> services.<br />
• Technical aspects :<br />
o Development of curriculum, training calendar & preparation of training material.<br />
o Identification of training sites.<br />
o Finalisation of trainers.<br />
• Sanction of budget<br />
• Identification of Medical Officers<br />
• Consent of Medical Education department for involvement of Medical Colleges as well as<br />
their faculty members.<br />
It is expected to start the training course from 1 st April 2011 by completing all the official<br />
procedures.<br />
Total Budget: 40.20<br />
209
SECTION – B.24 : SPECIAL SCHEMES FOR TRIBAL AND LEFTIST EXTREMISM AFFECTED AREAS<br />
Maharashtra has 15 tribal districts out of which 5 are sensitive and six are leftist<br />
extremism affected districts. Considering the <strong>health</strong> problems of these areas and nonavailability<br />
of trained staff to provide the <strong>health</strong> services, specific schemes are proposed for<br />
these areas. Schemes in Part –A are related to all the tribal areas of the State. However more<br />
focus is given to districts with remote tribal areas. Part – B of this Section is related to special<br />
schemes and activities proposed for high focus districts namely: Nandurbar, Gondia and<br />
Gadchiroli.<br />
Following schemes are proposed for tribal and leftist extremism areas.<br />
PART – A : SCHEMES FOR ALL TRIBAL AREAS OF THE STATE<br />
SUB-SECTION – B.24.2 :MAHER SCHEME<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2008-09 66 66 76 76.000<br />
210<br />
Rs. in Lakhs<br />
Remarks<br />
Tribal areas have hilly terrain. Many of the tribal padas do not have pukka roads. Even if<br />
pukka roads are available, there is no reliable transportation system for transferring pregnant<br />
women in labour to nearby PHC. This is important cause of high maternal and neonatal<br />
mortality. It is not economical to provide vehicles at each tribal pada, nor it is feasible to<br />
develop emergency vehicle system as there is no mobile phone coverage in remote tribal<br />
areas and landlines are out of order for prolonged time.<br />
In such situation, if one room is build in PHC premises where pregnant woman will get<br />
admitted one week before her due date, all abovementioned problems will be solved. She<br />
can be daily checked by Doctor of PHC and can be transported to suitable referral center if<br />
any complications are detected during waiting period or during labour. Following facilities are<br />
being provided in ‘Maher Scheme’<br />
• One room of 5×5 meters<br />
• One sanitary block (Toilet and bathroom)<br />
• One kitchen ota with smokeless chulha<br />
• One solar water heater system on roof of the room
‘Maher’ will be maintained by local Self Help Group. When mother is admitted, mother, her<br />
young child and one relative will be provided food three times a day. It is proposed to provide<br />
Rs. 125/- per mother per day to SHG for this purpose. Currently Maher rooms are being<br />
constructed in 30 PHCs in the state, mostly in tribal and leftist extremism affected areas of<br />
Vidharbha region.<br />
Currently the scheme is being implemented in 60 PHCs OF Leftist Extremism affected and<br />
tribal areas. It is proposed to continue the program in same PHCs.<br />
Compliance of remarks<br />
Currently Maher is established at 60 places out of which it is functional at 37 places.<br />
Remaining places will be functional within next three months. In functional 37 places, total<br />
1859 mothers have benefited from this scheme. Once other centers are functional, the<br />
number of beneficiaries will increase.<br />
c. Budget requirement <strong>2012</strong>-<strong>13</strong><br />
Budget required for 2010-11 is for existing centers as well as new centers. Detailed budget<br />
required is as follows:<br />
Table – : Budget distribution for Maher Scheme<br />
Sir Particulars Unit cost<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
1 Construction of Maher room (spillover) 2 23 46<br />
2 Maintenance cost to SHG per delivery 0.005 6000 30<br />
Total 76<br />
SUB-SECTION – B.24.4 : VOLUNTEER TO TRIBAL AND LEFTIST EXTREMISM AFFECTED PHCS<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2008-09 24.6 24.6 24.6 12.240<br />
211<br />
Rs. in Lakhs<br />
Remarks<br />
Tribal population does not accept the <strong>health</strong> services from institutions as expected. Different<br />
language, different culture and different understanding about various diseases, etc. are<br />
important reasons for this. Considering this, it is proposed that one local volunteer, who
knows the local language and can understand the concept of positive <strong>health</strong> can be appointed<br />
as Volunteer in tribal PHC. This volunteer will welcome the patients, direct them for case<br />
papers, and inform them about the instructions given by doctor and nurses and give simple<br />
public <strong>health</strong> messages.<br />
Based on experience of the state, volunteer scheme is modified and now requested only for<br />
Melghat region as it was existing in this area since last 4 years through local funds. Under this<br />
scheme, 34 volunteers are appointed 2/<strong>health</strong> facility in all PHCs and Hospitals of Melghat.<br />
These Volunteers help the doctors and nurses to provide treatment, inform patient about<br />
importance of treatment, minimize LAMA, accompany the patient to higher center in case of<br />
referral. Currently these Volunteers are paid Rs. 3000/PM from local / volunteer funds.<br />
District has requested the honorarium to be increased to Rs. 5000/PM, however, this increase<br />
will be considered after evaluation of the scheme by Public Health Department. Therefore,<br />
presently Rs. 3000/PM is reqested for the Volunteer. If the evaluation comes to be positive<br />
then honorarium will be increased to Rs. 5000/PM.<br />
Budget requirement<br />
Budget required per Volunteer will be Rs. 36000/volunteer/year and for 34 volunteers the<br />
budget is 34×0.36 = 12.24 Lakh.<br />
Table – : Budget required for Volunteer to tribal PHCs of Melghat region – <strong>2012</strong>-<strong>13</strong><br />
Rs. In Lakhs<br />
Sir Particulars Unit cost No. of units<br />
Budget<br />
required<br />
2 Honorarium (Rs. 3000/ PM) 0.36 34 12.24<br />
Total 12.24<br />
Honorarium to Volunteer will be increased to Rs. 5000/PM once the evaluation is received<br />
SUB-SECTION – B.24.5. : MOBILITY SUPPORT<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2008-09 728.3 496.6 670.3 670.300<br />
212<br />
Rs. in Lakhs<br />
Remarks<br />
Transport is required to transfer emergency patients and women in labor in <strong>health</strong><br />
institutions. Transport of delivery patients from village to <strong>health</strong> institutions for scheduled or<br />
emergency transfer is available with support of RCH funds. Referral plan of all the villages are<br />
being made.
Mobility support is also required to officers for supervision in tribal areas of the state. There<br />
are 70 tribal blocks in state to supervise the tribal PHCs. The Block Health Officers require<br />
vehicles to supervise the work of tribal PHCs.<br />
Compliance of remarks<br />
Supervisory work of the officers supervising NRHM works has increased many fold. As each<br />
<strong>health</strong> facility is being monitored from district and state level, lot of information is being<br />
collected and officers are also travelling to <strong>health</strong> facilities to go through the discrepancies.<br />
We have submitted proposal for hiring of vehicles to district officials through RCH. This costs<br />
about Rs. 3.0 Lakh per officer in one year. Currently cheaper supervisory vehicles available on<br />
RC costs about 4.5 Lakh. Thus, this cost will be cleared within one and half year. Considering<br />
life of vehicle for 12 years, this will be really beneficial to the SHS. Cost on driver and POL will<br />
be borne from regular budget of State Government. It will not have any impact on the NRHM<br />
budget. Considering this, it is requested to sanction this proposal along with the supervisory<br />
vehicles.<br />
Budget for repairs is required almost every year to ambulances. Currently available state<br />
government budget is inadequate and is not sufficient to fulfill the increase in demand. In<br />
tribal areas, roads are not good so that increases the maintenance. Other maintenance<br />
activities required routinely include, preventive maintenance, tyre, batteries, etc.<br />
Considering the situation above, budget as requested below is proposed for tribal and LEA<br />
areas:<br />
Budget requirement 2011-12<br />
Budget proposed for providing mobility support is as follows:<br />
Table – : Budget required for ambulance service in PHC/RH/SDH - 2009-10<br />
Rs. In Lakhs<br />
Total<br />
Sir Institution No. of units Unit price budget<br />
required<br />
1 New PHC ambulances 32 5.4 172.8<br />
2 New RH/SDH/DH Ambulances 16 7.6 121.6<br />
3 Repairs of existing ambulances 315 0.5 157.5<br />
4 Supervisory vehicles 42 5.2 218.4<br />
Total 670.3<br />
2<strong>13</strong>
SUB-SECTION – B.24.6 : SOLAR BACK-UP SYSTEM FOR TRIBAL AREAS<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2008-09 622.5 595.5 595.5 192.000<br />
214<br />
Rs. in Lakhs<br />
Remarks<br />
There is severe electricity problem in state. IPHS <strong>health</strong> institutions require continuous power<br />
supply. Therefore solar backup system is proposed for all the IPHS <strong>health</strong> institutions in tribal<br />
areas.<br />
Special system has been developed in the state with the help of Government College of<br />
Engineering Pune for <strong>health</strong> facilities. This system can provide power to all the equipment in<br />
PHC for 24 hours.<br />
Same system will be used for tribal areas. This year, it is proposed to try solar back up system<br />
for selected Rural Hospitals. Budget required for this system is as follows:<br />
Compliance of remarks<br />
All the PHCs in tribal areas are covered now so there is no need of grants for tribal PHCs.<br />
However, this year, grant is requested for hospitals which fulfill criteria of delivery point.<br />
List of hospitals included is submitted in Annexure.<br />
Budget required for solar power backup<br />
Budget required for solar power backup is mentioned below:<br />
Table – :Budget required for solar power backup<br />
Sir Type of institute Cost per unit No. of units<br />
Rs. In Lakhs<br />
Total cost<br />
2 Solar Backup – RH 32 16 192<br />
Total 16 192<br />
Considering the importance of un-interrupted power supply, it is proposed to add new <strong>health</strong><br />
institutes for solar power if there is saving in other activities.
SUBSECION B.24.7 : MOBILE MEDICAL UNITS FOR TRIBAL DISTRICTS<br />
Activity deleted as per remarks.<br />
SUBSECTION - B.24.8 : ORGANIZATION OF SPECIALIST MEDICAL & DENTAL CAMPS<br />
THROUGH MEDICAL COLLEGES IN TRIBAL HOSPITALS<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2008-09 127.44 231 250.2 250.200<br />
215<br />
Rs. in Lakhs<br />
Remarks<br />
Maharashtra has 455 hospitals of various bed strengths. Almost all of these hospitals are well<br />
equipped with wards. Operation theater, labour rooms and equipment. However, because of<br />
shortage of specialist by almost 50%, these hospitals are not in positions to provide specialists<br />
care. Considering this situations, it is proposed to arrange specialist camps in sub-district<br />
hospitals particularly the SDH/ Rural Hospital in tribal areas. Specialists of at least 8 specialties<br />
will be visiting the hospitals and provide specialist services.<br />
Specialists involved in the camps: Medicine, surgery, pediatrics, OBGY, ENT, Orthopedic, Skin<br />
& V.D , Anesthesia and Dental faculty.<br />
Sixty Specialty Medical & Dental Camps were organized during 2011-12. Patients<br />
referred by Primary Health Center were examined, diagnosed & given the treatment. Average<br />
2000 patients examined in each camp & more than average 50 major surgeries were done in<br />
each camp. The patients detected in School Health Examinations, sickle cell program,<br />
malnourished children, gynecological & pregnant mother with BOH were examined & given<br />
proper treatment.<br />
During <strong>2012</strong>-<strong>13</strong>, Sixty Medical & Dental Camps are proposed in tribal Sub- District/<br />
Rural hospital with the help of medical colleges/multi-specialty hospitals<br />
Organization of the camps will be done as follows:<br />
1. All the PHCs and hospitals in areas will be informed in advanced regarding the camp<br />
date & places where camp to be organized.<br />
2. PHCs /CHCs will screen the patients and send them to SDH on the day of camp.<br />
3. SDH will be selected on following criteria:<br />
a) Tribal SDH<br />
b) Well-constructed OT with all necessary equipment<br />
c) Laboratory with facility of all basis investigations<br />
d) Blood storage centre<br />
e) adequate nursing staff
4. Medical college & Dental College in the region will be identified for Specialist services<br />
in the camps.<br />
5. Medical College specialists will halt at SDH for 4 days on first day screening of Patients<br />
will be done on second and third day operations and surgeries will be conducted. On<br />
the fourth day post-operative care will be provided.<br />
Proposed Budget<br />
Budget will be required for following activities<br />
• Transportation of the specialists<br />
• Incentive to specialists<br />
• Staying arrangements for specialists<br />
• Incidental charges for the camp arrangement<br />
• Medicines, consumables, etc.<br />
It is proposed to organize 60 specialty camps in the state. Camp wise expenditure may change<br />
depending upon number of patients attended & Surgeries performed in the camps.<br />
Table -: Budget required for specialists camps through Medical colleges in tribal areas<br />
(Rs. In Lakhs)<br />
SR Activity<br />
1 Honorarium to Senior specialists @ Rs. 2000/<br />
day & Rs.1500/- for Jr. Specialist<br />
2 Hiring of vehicles to transport 16 specialists to<br />
SDH and back (4 day)<br />
Unit cost<br />
(single<br />
camp)<br />
No. of.<br />
units<br />
(Total 60<br />
camps)<br />
216<br />
Budget<br />
required<br />
1.12 60 67.20<br />
0.30 60 18.00<br />
3 Staying arrangements for specialists 0.30 60 18.00<br />
4 Arrangements of camps & office expenses 0.45 60 27.00<br />
5 Medicines and consumables for camps 1.50 60 90.00<br />
6 Transportation of patients 0.25 60 15.00<br />
7 IEC 0.25 60 15.00<br />
Total 4.17 250.2
SUBSECTION - B.24.9 : PILOT PROJECT TO REDUCE IMR IN MELGHAT REGION (DIST.<br />
AMARAWATI) OF MAHARASHTRA<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2008-09 115.81 96.72 81.92 81.920<br />
217<br />
Rs. in Lakhs<br />
Remarks<br />
As per SRS, IMR of Maharashtra is 33/1000 live births. However, it not equally distributed<br />
throughout the state. There are some pockets which indicate almost double the IMR of state<br />
average. One of such pockets is Melghat. Currently, estimated IMR of Melghat is around<br />
60/1000 live births which is highest in the state. Lot of measures have been carried out since<br />
last 10 years. However after initial reduction, IMR is not going down since last 3-4 years.<br />
Considering this situation, a pilot project is being submitted for this area to reduce IMR.<br />
1. Peculiarities of Melghat region<br />
• Reserve forest (Tiger reserve), very dense with very low population density.<br />
• Communication facility underdeveloped.<br />
• Because of low density of population, geographical distance from PHC is very long. For<br />
example, 6 villages of one PHC are situated 150 KM from PHC HQ. This leads to very<br />
difficult situation in contacting the families.<br />
• People do not prefer to go to <strong>health</strong> institutions. Instead they go to local quacks.<br />
• Language of local tribes is different (Korku). Very few Tribes can understand Marathi<br />
language.<br />
2. Findings of infant deaths<br />
• Causes of infant mortality are same : LBW/immaturity, diarrhea, ARI.<br />
• Almost all infant deaths are within first 6 months of life.<br />
• Family members ignore the <strong>health</strong> of child very often. They do not take ill child<br />
immediately to doctor for treatment.<br />
• Proportion of home delivery is 90%, which is slowly increasing because of active<br />
intervention of ASHA.<br />
• All the PHCs in Melghat are well equipped to treat the children but very few families<br />
take the benefits of these facilities.<br />
3. Positive findings in recent times<br />
• People have accepted ASHAs very well. ASHAs are now bringing mothers for ANC<br />
check-up and delivery. ANC check-up has increased but delivery is taking some time to<br />
increase.
• Local volunteer appointed has proved very useful. He/she can talk to patients to<br />
consume medicines given in PHC and also convince mothers in local language and<br />
persuade them to stay in PHC for 2 days after delivery.<br />
• PHCs in the area are provided all required equipment in neonatal care and MOs are<br />
trained.<br />
• There is one CHC and one SDH in area. One pediatrician is available in these centers.<br />
Considering the above situation and development in recent times, project as mentioned<br />
below is submitted for approval:<br />
4. Pilot Project<br />
Following activities will be carried out in this project<br />
• ASHA will monitor nutrition of mother particularly anemia by colour coded finger caps<br />
provided to her. If mother is anemic then FS will be provided to mother. These tablets<br />
will be consumed by mother in front of ASHA.<br />
• ASHA will motivate the mothers to get delivered in PHC or hospital. If not possible<br />
then ASHA will arrange for delivery by trained person, will judge the risk of new born<br />
by measuring the foot length of child and classify the child based on the foot length<br />
equipment.<br />
• ASHA will be trained to monitor daily the <strong>health</strong> of child for up to 6 months of life. She<br />
will check following five parameters:<br />
o Whether child is breast feeding?<br />
o Do the child have fever?<br />
o Do the child have diarrhea?<br />
o Do the child have running nose?<br />
o Respiratory rate of child is normal or not?<br />
• This volunteer will monitor 7-8 children per day.<br />
• After child birth, one card will be issued in the name of child. Volunteer will daily<br />
record her findings in the card. At the end of 6 months, the card will be deposited in<br />
PHC. In case of referral, Volunteer will take card to PHC.<br />
• In case answer to any of the above question is yes, Volunteer will immediately inform<br />
the Special Squad MO about <strong>health</strong> of child. Special Squad will arrive in village, check<br />
the child and if required bring the child to nearest PHC or CHC for further treatment.<br />
• Volunteer will be given one Mobile Phone (in 50% area there is coverage) or wireless<br />
devise to contact the MO.<br />
• Special squad will consist of MO of PHC one nurse from PHC and one local volunteer<br />
(to be appointed). Special squad will be provided one ambulance.<br />
• As there are very long distances between <strong>health</strong> institutes, ambulance will be<br />
equipped with baby warmer, oxygen cylinder, neonatal resuscitation kit, IV facility,<br />
etc.<br />
5. Extent of the project<br />
218
Total Melghat area having 11 PHCs, 2 CHCs and one SDH.<br />
Compliance of remarks<br />
• In this project, 10 important signs/symptoms that can be verified by ASHA are included. ASHA<br />
has to check these with child daily and inform the doctor in case of any danger sign. As all<br />
these signs and symptoms are already existing in Module – VI of ASHA, it was decided to hold<br />
till training of this module is complete. There was delay because of this decision.<br />
• This project was shown to UNICEF consultants. They suggested addition of pediatrician to the<br />
project. However, as this is very interior area, no pediatrician applied for the post in spite of<br />
advertisement twice. Therefore post of pediatrician is dropped in PIP <strong>2012</strong>-<strong>13</strong>. Now it has<br />
been planned to appoint experienced doctor (MBBS/BAMS) with salary ranging from Rs.<br />
20000 to 40000/PM)<br />
• Till date, 347 children (0-6 months) are registered for the project. Special two day meeting is<br />
organized for this project in first week of May. Implementation is expected to improve after<br />
the meeting.<br />
6. Budget requirement<br />
Considering the present experience of local Block Medical Officers, there will be 5-6 calls per<br />
PHC for sick children to be examined. Thus, ambulance will travel for approximately 150 KM<br />
in a day.<br />
Budget will be required for following purposes:<br />
• Remuneration to ASHA for each visit to child (Rs. 3/visit) considering she will spend<br />
about 1 hour for this work.<br />
• Remuneration to ASHA to accompany the child to hospital – Rs. 75/day – minimum<br />
one day<br />
• Honorarium to local volunteer who accompanies the ambulance to convince the<br />
family to accept treatment<br />
• Ambulances with equipment<br />
• Driver, POL, maintenance for ambulance.<br />
Services of MO, medicine and PHC level treatment will be provided under regular finds.<br />
Total budget required is submitted in table below:<br />
Table -: Budget required for Special IMR reduction project<br />
Sir Activity Unit cost<br />
1<br />
Remuneration to ASHA @ Rs. 5/visit. ASHA will<br />
make average 6 visits daily (approx 2100 visits in<br />
one year) for 350 ASHA<br />
No. of<br />
units<br />
219<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
0.054 350 18.9
Sir Activity Unit cost<br />
2<br />
ASHA to accompany child to hospital @ Rs.<br />
100/day. 5000 visits<br />
No. of<br />
units<br />
220<br />
Budget<br />
required<br />
0.001 5000 5<br />
3<br />
Provision of important gadgets such as<br />
communication device, thermometer, foot length<br />
caliper, finger caps, etc. to ASHA<br />
1 11 11<br />
4<br />
Honorarium to local volunteer cum driver @ Rs.<br />
6000/Driver/month in 11 PHCs<br />
0.72 11 7.92<br />
5<br />
POL and maintenance of ambulance considering<br />
100 KM run/day<br />
2.4 11 26.4<br />
6<br />
Contingency including travel and other allowances<br />
to experts<br />
0.3 11 3.3<br />
7 Important medicines to ASHA 0.02 350 7<br />
8<br />
Appointment of one experienced person as<br />
supervisor for implementation of the program<br />
2.4 1 2.4<br />
Total 81.92<br />
SUBSECTION - B.24.10 : COORDINATION CELL FOR TRIBES IN SELECTED LEA & TRIBAL<br />
DISTRICTS HOSPITALS<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2008-09 28.8 29.52 24.600<br />
Rs. in Lakhs<br />
Remarks<br />
Peripheral <strong>health</strong> institutions (SCs, PHCs, CHCs, etc.) have to refer patients to District<br />
Hospitals in emergency. Majority of the District Hospitals are 300 bedded and above. These<br />
hospitals have different sections for registration, laboratory checkup, X-ray, medicines, etc.<br />
Tribal patients do not understand the language and there is delay in getting all the formalities<br />
done. Because of such environment, patients are not willing to stay in hospital and many of<br />
the times insist for discharge even if the condition of patient is critical.<br />
Considering such situation, one pilot project was organized in District Hospital Amravati for<br />
patients from Melghat tribal areas. Six persons from hospital were pooled to form one cell<br />
with one telephone line. All the doctors in Melghat were informed about the Cell and<br />
telephone number. Now the doctors call the Melghat Cell in District Hospital at the time of
eferral. Patients <strong>health</strong> condition, required treatment and expected time of arrival is<br />
communicated. One Cell member takes the responsibility and informs the Casualty MO to call<br />
concerned specialists. When patient arrives, the Coordinator of Cell accompanies the patient<br />
till emergency is over from registration to laboratory and report collection. After emergency<br />
is over, the patients are asked to contact the cell in case of any difficulty in hospital. During<br />
the stay in hospital ell member visits the patient twice daily for any difficulty. Transport<br />
arrangement is also made if required after discharge.<br />
The cell in Melghat has increased the inflow of tribal patients from 38 per month to 73 per<br />
month. Proportion of referred patients actually arriving the hospital has increased from 58%<br />
to 81% and AMA discharge has reduced to only 2 patients in December 2010 as against 10-12<br />
patients per month during last year. Because of this response, Coordination Cell is now<br />
established in all the 6 Sensitive tribal districts which also include two LEA districts of state.<br />
Same activity will continue this year.<br />
Compliance of remarks<br />
One pilot project at DH Amravati has shown that if tribal patients are provided support then<br />
their stay in hospital improves. This project is based on the findings of this pilot study.<br />
This project was started in 6 districts : Amravati, Gadchiroli, Gondia, Thane, Nashik and<br />
Nandurbar. Out of these, this did not start in Gondia and started very late in Thane. District<br />
wise performance of the project is as follows:<br />
Table – Performance of Coordination cell at DH<br />
Sir Name of district Performance Remarks<br />
1 Thane 620 Started in December<br />
2011<br />
2 Nashik 17694<br />
3 Nandurbar 878<br />
4 Amravati 921 From Melghat area<br />
only<br />
5 Gondia 0 Not started. Dropped<br />
in year <strong>2012</strong>-<strong>13</strong><br />
6 Gadchiroli 7149<br />
Considering above performance, Gondia is discontinued from the scheme. Budget required<br />
for remaining centers is mentioned below.<br />
No new centers is proposed in <strong>2012</strong>-<strong>13</strong>.<br />
Budget requirement<br />
Budget will be required for following purposes<br />
221
• Salary of supervisor and coordinators<br />
• Furniture for the desk<br />
• Telephone line<br />
• Mobile charges for the supervisor and coordinators<br />
• Incidental charges<br />
Detailed budget requirement will be as follows:<br />
Table -: Budget required for tribal cell in District Hospital<br />
Sir Activity Unit cost No. of units<br />
222<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
1<br />
Salary of Tribal Cell Supervisor @ Rs. 8000/PM<br />
for 10 months<br />
0.96 5 4.8<br />
2<br />
Salary of Coordinators (4) @ Rs. 6000/PM for 10<br />
months<br />
2.88 5 14.4<br />
3 Telephone line for help desk 0.36 5 1.8<br />
4<br />
Mobile charges to all desk members @ Rs.<br />
200/PM for 10 months (no instrument charges)<br />
0.12 5 0.6<br />
5 Contingency 0.6 5 3<br />
Total 24.6<br />
SUBSECTION - B.24.11 : INTEGRATION OF PALLIATIVE CARE IN JAWHAR TRIBAL BLOCK DIST<br />
THANE<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2008-09 <strong>13</strong>.5 <strong>13</strong>.5 <strong>13</strong>.500<br />
Rs. in Lakhs<br />
Remarks<br />
Palliative Care is a multi disciplinary approach to alleviate the suffering of patients<br />
with chronic life limiting illnesses, and their families. It is aimed at improving the quality of life<br />
through relief of physical, psychosocial and spiritual suffering. The palliative care is required<br />
in terminal period of cancer, neurological and cardio respiratory discusses.<br />
For year 2011-12, the project is being implemented in a Jawhar tribal block of Thane district<br />
with the technical support and help from Tata Memorial Hospital and Research Centre,<br />
Mumbai.
Goal<br />
To integrate palliative care into the exciting <strong>health</strong> care system in the jawhar block of<br />
Thane district.<br />
Objectives:<br />
• Training <strong>health</strong> care professional including physicians, nurses and medical and<br />
social workers (at the block and the primary <strong>health</strong> centre level) in palliative care<br />
so that they are able to identify patients requiring palliative care and are able to<br />
deliver appropriate holistic care to such patients.<br />
• Training the outreach <strong>health</strong> workers such as ASHA workers, ANMs etc, in basic<br />
palliative care principles and practice, so that they can identify patients in the<br />
community who require palliative care and deliver basic care in the patients home<br />
or in the community.<br />
• Ensure the availability of morphine and other opioids at the block level.<br />
• Increase the awareness in the community about palliative care.<br />
• Ensure access of children with life limiting conditions to appropriate pediatrician<br />
Palliative care facilities.<br />
Performance in 2011-12<br />
• The training of Health Care Provider in Palliative Care is as follows<br />
Medical officers – 38, Nurses- 51,<br />
ASHA- 223, Medical Social worker – 1 &<br />
Paramedics – 3<br />
• Total patients under Palliative Care - 271<br />
Cancer Patients - 18, HIV Patients- 5, Resp. diseases & T.B patients-43, Cardio<br />
vascular diseases- 4, Mental retardation & cerebral palsy- 24 , leprosy- 11,<br />
Others- 171<br />
• Palliative Care diagnostic Camps conducted - 6<br />
Action plan<br />
• Establishment of Palliative Care Cell at the Sub-district hospital / Rural Hospital<br />
containing one Medical Officer, one Nurse and one Medical Social Worker.<br />
• Training of <strong>health</strong> care professionals including physicians, nurses and medical<br />
social workers at the block and the primary <strong>health</strong> centre level in palliative care.<br />
The training will be delivered by the palliative care team at Tata Memorial Centre<br />
(TMC), Mumbai. Training will be conducted at Tata Memorial Centre as this will<br />
give the trainees an opportunity to observe the working of the palliative care team<br />
at TMC. The duration of each training session will be two weeks.<br />
• Training the outreach <strong>health</strong> workers such as ASHA workers, ANMs etc. The<br />
palliative care team at Tata Memorials Centers (TMC), Mumbai, will carry out the<br />
training. Besides the palliative care team from TMC may also conduct training on<br />
223
site so as to reinforce appropriate knowledge, skills and attitudes and to identify<br />
and gaps.<br />
• Data collection and monitoring will be carried out throughout the project so as to<br />
capture the numbers of patients accessing palliative care services and the follow<br />
up, use of opioids and care in the terminal phase.<br />
• Evaluation of the program at baseline and on a monthly basis.<br />
Expected outcomes<br />
• Improved care for patients with life limiting diseases and their families.<br />
• Access to appropriate pain relief medications, including morphine.<br />
• Developing a model program for palliative care which can be applied across other<br />
districts in the state.<br />
Future Plans<br />
• Activities:-<br />
Expand the project activity in Tribal Block of Nashik District.<br />
Establishment of Palliative Care Cell at the Sub-district hospital/ Rural<br />
Hospital containing one Medical Officer, one Nurse and one Medical<br />
Social Worker to provide palliative care.<br />
The Palliative care team will make frequent visits to PHCs and<br />
households of patients registered under palliative care.<br />
Budget proposed for <strong>2012</strong>-<strong>13</strong><br />
Table – Budget requirement for palliative care Project<br />
( Rs. in Lakhs)<br />
SR. NO Activity Total Cost<br />
1 Training of Health Care professional & Training Material 1<br />
2 Support to faculty member from Tata Memorial Centre<br />
for travel & DA<br />
3 Medicines & Logistics 3<br />
4 Incentives for ASHA workers & other Health Care<br />
Provider<br />
5 Referral of Patients 1<br />
7 Salary of Contractual medical social worker & Medical<br />
officer<br />
9 TA of Palliative care Cell 1<br />
224<br />
1<br />
2<br />
3.50
10 IEC 1<br />
Total <strong>13</strong>.5<br />
The Total Budget required for the project is <strong>13</strong>.5 lacs. The project will be implemented in<br />
collaboration with Palliative care department Tata memorial centre, Mumbai.<br />
SUBSECTION – B.24.12 : ESTABLISHMENT OF NUTRITIONAL REHABILITATION CENTERS IN<br />
TRIBAL AND LEA BLOCKS<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
2008-09 41.4 92.16 92.160<br />
225<br />
Rs. in Lakhs<br />
Remarks<br />
Introduction –<br />
A Nutrition Rehabilitation Centre (NRC) is a facility based care center, for the<br />
management of Severely Malnourished Children. In NRC malnourished Children are admitted<br />
with defined ad<strong>mission</strong> criteria. They are kept under observation and provided with medical<br />
and therapeutic care. In addition focus is on improving the skills of mothers on complete care<br />
and feeding. Training of Nutrition Rehabilitation to Health and ICDS Functionaries is also<br />
undertaken in NRC.<br />
In Maharashtra 6 NRCs have been established at Gondia, Gadchiroli, Dharni<br />
(Amravati), Thane Nandurbar and Nashik.<br />
A) Objectives<br />
- To function as apex institute for malnutrition.<br />
- To provide institutional care for children with severe malnutrition.<br />
- To promote physical, mental & social development of children with severe<br />
malnutrition.<br />
- To build capacity of primary care givers in the home based management of<br />
malnourished children.<br />
- To train the medical and paramedical staff regarding management of malnourished<br />
children in the facilities and their household care after discharge<br />
B) Situation Analysis<br />
NRC Weekly Report for week ending 26.12.2011
Sr.<br />
No.<br />
1<br />
Name of NRC No.of<br />
children<br />
admitted<br />
in the<br />
week<br />
GH<br />
Gadchiroli<br />
Progressive<br />
No.of<br />
children<br />
admitted<br />
No.of<br />
children<br />
admitted<br />
at the end<br />
of week<br />
No.of<br />
children<br />
cured since<br />
beginning<br />
of NRC<br />
(Aug 2011)<br />
2 29 4 18<br />
2 WH Gondia 3 53 8 45<br />
3 SDH Dharni 5 23 9 14<br />
4 GH Nashik 0 20 1 17<br />
5<br />
GH<br />
Nandurbar<br />
5 5 5 0<br />
6 GH Thane 8 15 9 6<br />
Total 23 145 36 100<br />
C) Proposed Budget for <strong>2012</strong><br />
Remarks<br />
(LAMA -5,<br />
Medical<br />
Transfer 2<br />
Table - Nutrition Rehabilitation Centres Budget Estimates for One NRC<br />
Rs in Lakhs<br />
Sr.<br />
Item<br />
No.<br />
A Human resources<br />
Contractual ANM<br />
@ Rs<br />
9000/each/pm<br />
Part time Sweeper<br />
@ Rs. 1500/pm<br />
Number<br />
required<br />
Cost<br />
estimate/month<br />
Annual Remark & Justification<br />
2 0.18 2.16 Newly Proposed - 1) As<br />
proposed in expert<br />
committee meeting on<br />
30th April 2011 at<br />
Nagpur 2) During<br />
monitoring visits to the<br />
NRCs it was observed<br />
that separate ANMs are<br />
necessary for NRC<br />
1 0.015 0.18 Rs 500/- increase in the<br />
payment proposed in<br />
expert committee<br />
meeting on 30th April<br />
2011 at Nagpur as it is<br />
difficult to get sweeper<br />
at Rs 1000/-<br />
226
Sr.<br />
No.<br />
Item<br />
Contractual Cook<br />
@ Rs<br />
3500/each/pm<br />
Contractual<br />
Attendant @ Rs<br />
3500/each/pm<br />
Contractual NRC<br />
Coordinator @ Rs<br />
7000/each/pm<br />
B Medicines<br />
Medicines<br />
Electrolytes &<br />
Minerals<br />
(Potassium,<br />
Magnesium, Zinc<br />
& Copper<br />
supplement), Iron<br />
& Folic Acid,<br />
Albendzole, Anti<br />
Amoebic drugs,<br />
Multi Vitamin<br />
syrup, K-ReSoMal,<br />
Syrup Kesol-20 by<br />
EISEN etc.<br />
C Diet of Children<br />
@Rs. 25/Day &<br />
Parents @ Rs<br />
60/Day (Per day<br />
10 Children<br />
D Wages Lost @ Rs<br />
60/Day<br />
E AWW Honorarium<br />
@ Rs 150/ Child x<br />
20 Children/pm<br />
for bringing child<br />
for ad<strong>mission</strong> into<br />
NRC<br />
Number<br />
required<br />
Cost<br />
estimate/month<br />
1 0.035 0.42<br />
2 0.07 0.84<br />
1 0.07 0.84<br />
Annual Remark & Justification<br />
0.01 0.12 Routine medicines<br />
should be used from<br />
hospital store.<br />
Medicine not available<br />
in store ,only that<br />
medicines should be<br />
purchased<br />
0.255 3.06<br />
0.18 2.16<br />
0.03 0.36 *Annual 240 Children<br />
As proposed in expert<br />
committee meeting on<br />
30th April 2011 at<br />
Nagpur<br />
227
Sr.<br />
No.<br />
Item<br />
Transportation<br />
cost to AWW for<br />
bringing child @<br />
Rs.200X10<br />
children<br />
Transportation<br />
cost to mother @<br />
Rs.200X10<br />
children<br />
Number<br />
required<br />
Cost<br />
estimate/month<br />
Annual Remark & Justification<br />
0.02 0.24 *Annual 120 Children<br />
As proposed in expert<br />
committee meeting on<br />
30th April 2011 at<br />
Nagpur. If Govt. vehicle<br />
is used for<br />
transportation, charges<br />
for transportation will<br />
not be admissible<br />
0.02 0.24 *Annual 120 Children<br />
As proposed in expert<br />
committee meeting on<br />
30th April 2011 at<br />
Nagpur. If Govt. vehicle<br />
is used for<br />
transportation, charges<br />
for transportation will<br />
not be admissible<br />
F Stationary 0.06<br />
G Event<br />
Management<br />
(Celebration of<br />
Health days etc)<br />
0.06<br />
H Printing, Xeroxing,<br />
Photo etc.<br />
0.06<br />
I AWW Honorarium<br />
@ Rs 200/ Child<br />
for follow up of<br />
the child<br />
discharged from<br />
NRC program for 1<br />
year, admissible<br />
only if child does<br />
not become SAM<br />
and certified by<br />
concerned MO<br />
PHC<br />
0.04 0.48 Annual 240 Children<br />
AWW Honorarium<br />
@ Rs 100 x 4<br />
0.08 0.96 Annual 240 Children<br />
228
Sr.<br />
No.<br />
Item<br />
follow up x 20<br />
Children/month<br />
Transportation<br />
charges for<br />
AWW@Rs<br />
200/visit x 4 visits<br />
x 10<br />
children/month<br />
Transportation<br />
charges for<br />
mother@Rs<br />
200/visit x 4 visits<br />
x 10<br />
children/month<br />
Diet of Child,<br />
mother and AWW<br />
@Rs. 75 for 3<br />
persons 4 follow<br />
up visits/ childx20<br />
children/month<br />
diet to be<br />
provided from<br />
NRC<br />
J Training Cost<br />
J Training Cost -<br />
One day trg of Dist<br />
hospital, Rural<br />
hospital & PHC<br />
Mos & Staff Nurse<br />
regarding NRC<br />
(resource persons-<br />
Pediatrician and<br />
NRC coordinator<br />
Number<br />
required<br />
One<br />
batch<br />
per<br />
month (<br />
Batch<br />
size 30)<br />
Cost<br />
estimate/month<br />
Annual Remark & Justification<br />
0.08 0.96 Annual 120 Children As<br />
proposed in expert<br />
committee meeting on<br />
30th April 2011 at<br />
Nagpur If Govt. vehicle<br />
is used for<br />
transportation, charges<br />
for transportation will<br />
not be admissible<br />
0.08 0.96 Annual 120 Children As<br />
proposed in expert<br />
committee meeting on<br />
30th April 2011 at<br />
Nagpur If Govt. vehicle<br />
is used for<br />
transportation, charges<br />
for transportation will<br />
not be admissible<br />
0.06 0.72 Annual 240 Children. As<br />
proposed in expert<br />
committee meeting on<br />
30th April 2011 at<br />
Nagpur<br />
0.03 0.36 360 trainees annually<br />
229
Sr.<br />
No.<br />
Item<br />
working in NRC)<br />
. One day Trg of<br />
AWWs, ANMs<br />
regarding home<br />
management of<br />
SAM children to<br />
be conducted at<br />
PHC level during<br />
meeting)<br />
k Soap, hair oil and<br />
contingent<br />
expenses<br />
Total Recurring<br />
Cost<br />
Number<br />
required<br />
Cost<br />
estimate/month<br />
Annual Remark & Justification<br />
0.12 As proposed in expert<br />
committee meeting on<br />
30th April 2011 at<br />
Nagpur<br />
15.36<br />
Note- If Govt. vehicle is used for transportation, charges for transportation will not be<br />
admissible<br />
Total Budgetary Requirements for 6 NRCs = 15.36 x 6 = Rs 92.16 Lakhs<br />
SUBSECTION – B.24.<strong>13</strong> : ESTABLISHMENT OF MEDICINE WAREHOUSE AT SELECTED PLACES<br />
IN TRIBAL AREAS<br />
Year of starting<br />
the<br />
scheme/initiative<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Budget<br />
sanctioned<br />
for year<br />
2010-11<br />
Budget<br />
sanctioned<br />
for year<br />
2011-12<br />
Budget<br />
proposed<br />
in PIP<br />
<strong>2012</strong>-<strong>13</strong><br />
Budget<br />
Proposed<br />
in NPCC<br />
0 1742.23 150 150.000<br />
230<br />
Rs. in Lakhs<br />
Remarks<br />
Warehouse are required for storage of medicines. Some tribal areas of the state are far away<br />
from the district HQ. It requires almost a day to reach these places because of distance and<br />
condition of roads. In Mansoon it becomes very difficult to reach these places in most of the<br />
July and August month.<br />
Considering above problem; it is prepared to build good quality warehouse one each at<br />
Semadoh (Melghat), Adivasi (Gadchiroli) & Dhadgaon (Nandurbar)
Each of the warehouse will be 100 Sq. feet with modern storage of system. Budget<br />
required for warehouse is Rs. 50.0 Lakhs/warehouse. Total budget required is Rs. 1.5 Cr.<br />
SUB-SECTION –B.24.14: TELEMEDICINE IN TRIBAL AREAS<br />
SUMMARY INFORMATION OF THE SCHEME/INITIATIVE<br />
Telemedicine are being provided to all the districts in the Maharashtra state. However as<br />
Nandurbar and Gadchiroli districts, being leftist extremism affected, more number of<br />
Telemedicine Centre are proposed for their districts. Therefore it is proposed to provide 1<br />
centre for Nandurbar districts and 3 centers for Gadchiroli districts.<br />
Considering the underserved area, backwardness and difficult terrain, it is proposed to<br />
provide additional 4 Rural/Sub -districts –Taloda Dist. Nandurbar, Sironcha Dist. Gadchiroli,<br />
Dhanora Dist. gadchiroli and Jawhar Dist Thane for telemedicine over and above the<br />
sanctions under NRHM.<br />
Considering the proposal above, total budget required will be as follows:<br />
Year of starting<br />
the scheme/<br />
initiative<br />
Budget proposed for<br />
PIP <strong>2012</strong>-<strong>13</strong> to Preappraisal<br />
committee<br />
Final budget<br />
proposed to<br />
NPCC<br />
<strong>2012</strong>-<strong>13</strong> 32.45 32.450<br />
Remarks<br />
231<br />
Rs. in Lakhs<br />
Budget revised as per need of<br />
program<br />
Telemedicine is a rapidly developing application of clinical medicine where medical<br />
information is transferred via telephone, Internet or other networks for the purpose of<br />
consulting, and sometimes remote medical procedures or examinations. Telemedicine may<br />
be as simple as two <strong>health</strong> professionals discussing a case over the telephone, or as complex<br />
as using satellite technology,Internet with Static IP and video-conferencing equipment to<br />
conduct a real-time consultation between medical specialists in two different places.<br />
Telemedicine Centers in Maharashtra<br />
These nodes seek expert services from 6 specialty nodes, out of which 3 are situated in<br />
Mumbai, and one each at Pune, Aurangabad and Nagpur.<br />
Performance of telemedicine centers in Maharashtra<br />
In Maharashtra, fourteen specialties are started for opinion under telemedicine. So far 22456<br />
patients (Up to Feb <strong>2012</strong>) have been referred to Medical College Hospital sand opinion<br />
received for 22325 patients.<br />
Total 14 CME organized through telemedicine center for specific issues like sickle cell disease,<br />
epilepsy, school <strong>health</strong> patients, etc.<br />
Plan of action for year <strong>2012</strong>-<strong>13</strong>
During year <strong>2012</strong>-<strong>13</strong>, new telemedicine center will be opened. Following actions are<br />
proposed during <strong>2012</strong>-<strong>13</strong>.<br />
• Increasing the utilization of centers.<br />
• Adding digital telemedicine equipment to new proposed centers to improve their<br />
quality of work<br />
• Expansion RH/SDH nodes and making them functional.<br />
• Strengthening the management system of telemedicine project.<br />
• CME’s for Medical and Paramedical staff.<br />
Budget requirement for <strong>2012</strong>-<strong>13</strong><br />
Budget is required for following purposes:<br />
Table – Budget required for Tribal Telemedicine Centers<br />
(Rs. in Lakhs)<br />
Sir<br />
No.<br />
Particulars Unit Cost<br />
No. of<br />
units<br />
232<br />
Budget<br />
required<br />
1 Construction & renovation of room 3 4 12<br />
2<br />
Salary & TA/DA of Facility Manager for<br />
New tribal <strong>rural</strong>/Sub - district hospitals<br />
0.86 4 3.45<br />
3 Honorarium to Doctors – Patient node<br />
Contingency to Patient nodes<br />
0.001 1000 1<br />
4 ( including Civil works & other<br />
maintenance)<br />
0.1 4 0.4<br />
5<br />
Procurement of additional equipment to<br />
tribal patient nodes of telemedicine<br />
centers (Telemedicine Equipments, video<br />
Conferencing camera, Software, etc)<br />
3 4 12<br />
6 Connectivity expenses 0.9 4 3.6<br />
Total 32.45
Chapter 25<br />
SCHEMES FOR HIGH FOCUS DISTRICTS<br />
Schemes under this chapter are all specific for three high focus districts. They are different<br />
from schemes of tribal areas of other districts or schemes for other LEA districts.<br />
Drawings and primary estimates of all the construction works will be submitted before NPCC.<br />
This is because PWD is busy with year end works and response from High Focus districts<br />
requires some time.<br />
1. NANDURBAR DISTRICT<br />
Nandurbar district is 100% tribal district in North Maharashtra. High ranges of Satpuda<br />
Mountain ranges and Narmada river along with backwaters of Sardar Sarovar has made more<br />
than 30% of the villages very remote and not accessible by road. This is one of the important<br />
reasons for poor performance of the districts in <strong>health</strong> indicators. Considering the situation of<br />
the district, following activities / schemes are proposed for Nandurbar district.<br />
a. Health Shelter<br />
In blocks of Dhadgaon and Akkalkuwa, many of the <strong>health</strong> facilities and also villages are at<br />
such a remote place that <strong>health</strong> worker need to travel up to 45 Kilometers on foot to reach<br />
remote villages from his/her HQ. This makes extremely difficult for them to travel to these<br />
remote villages. There are no homes, schools or other places to stay overnight for the staff.<br />
Considering this peculiar situation, it is proposed to build pre-fabricated shelter homes at<br />
places where the villages are more than 25 KM from HQ of the <strong>health</strong> worker. Ten places in<br />
these blocks have been identified for such shelter homes.<br />
Shelter will be two rooms of 150 sq. feed one for male staff and one for female staff, one<br />
kitchen of 50 sq. feet and one toilet block of 50 sq. feet. Total shelter will be of 400 sq. feet.<br />
Local SHG or ASHA will be given responsibility to maintain the shelter. She will be paid Rs.<br />
3000/PM towards maintenance and provision of food. Food charges will be borne by<br />
concerned <strong>health</strong> worker.<br />
List of facilities where <strong>health</strong> shelter is required is submitted in annexure<br />
Budget requirement<br />
Budget required for shelter is for construction of shelter, maintenance and contingency for<br />
keeping drinking water, etc.Detailed budget requirement is as follows:<br />
233
Table – Budget requirement for Health Shelter<br />
Sir Activity Unit cost<br />
1<br />
Construction of Health Shelter including one<br />
borewell for water supply (one time)<br />
No.of<br />
units<br />
234<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
12 10 120<br />
2 Maintenance by SHG/ASHA 0.36 10 3.6<br />
3<br />
Other maintenance charges (Drinking water,<br />
electricity, drainage, etc.)<br />
0.36 10 3.6<br />
4 Furniture grant (one time) 0.5 10 5<br />
Total <strong>13</strong>2.2<br />
b. Wireless contact<br />
Major part of interior areas in the district is not approachable by any means of<br />
communication including mobile phones and BSNL wireless network. Therefore it is proposed<br />
to provide one wireless set to each of the SC in interior areas. The base of the wireless<br />
network will be at district level. Message for ambulance to shift mother in labour, critically ill<br />
child and epidemics are expected from this system. System will be procured by following<br />
procurement procedure. Budget required for this activity will be as follows<br />
Table – Budget requirement for Wireless contact system<br />
Sir Activity Unit cost<br />
No.of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
1 Wireless set 0.5 56 28<br />
2 Base station at Nandurbar 5 1 5<br />
3 Salary of operator at Nandurbar 1.2 1 1.2<br />
4 Contingency including civil works, stationary, etc. 0.5 1 0.5<br />
Total 34.7<br />
c. Floating Dispensaries and Floating ambulances<br />
About 50 villages of Nandurbar district are completely isolated due to Backwaters of Sardar<br />
Sarovar. These villages have mountain on one side and back water on other side. Government<br />
of Maharashtra is providing <strong>health</strong> services to theses villages by floating dispensaries. These<br />
dispensaries visit all the villages on fixed days and provide services. Only the post of Medical<br />
Officer and Driver are approved by Government. These dispensaries are providing good<br />
services, however, in case of emergency, particularly the delivery case or critically sick child,
they have to discontinue the service and take the patient back to Health Facility for<br />
treatment. This leads to major disruption of services to remaining villages and irregularity in<br />
service provision.<br />
Distance between floating dispensary and bank of river changes every time and patients need<br />
to travel in water to reach dispensary. This becomes very difficult for the patients particularly<br />
the pregnant women. In addition there is no place for patients to wait till the Floating<br />
dispensary approaches the villages. Therefore, one clinic room is proposed at each stop of the<br />
dispensary.<br />
Considering the above condition, it is proposed to provide additional essential staff and space<br />
to Floating Dispensary and three Floating Ambulances to this areas so that these ambulances<br />
can be called to shift pregnant women, critically ill neonates and other sick persons. The<br />
ambulance will be called through wireless contact system.<br />
Budget required for this activity is as mentioned in table below:<br />
Table – Budget requirement for Floating dispensaries and Ambulances<br />
Sir Activity Unit cost<br />
No.of<br />
units<br />
235<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
A Floating dispensary<br />
1 Pharmacist (one per dispensary) 1.2 2 2.4<br />
2 ANM 1.44 2 2.88<br />
3 Laboratory Technician 1.2 2 2.4<br />
4 Construction of clinic (Fibre - 400 sq. feet) 12 16 192<br />
5 Maintenance of clinic by local ASHA 0.36 16 5.76<br />
6 Solar light system and water supply 3 16 48<br />
4 Assistant 0.96 2 1.92<br />
5 Medicine 0.5 2 1<br />
6 Additional POL 0.5 2 1<br />
Total Floating dispensary 257.36<br />
B Floating Ambulance<br />
1 Procurement of Floating Ambulance 20 3 60<br />
2 One Driver 0.48 3 1.44<br />
3 One ANM in ambulance 0.72 3 2.16<br />
4 One Assistant 0.36 3 1.08<br />
5 Total Floating Ambulance 64.68<br />
Grand Total 322.04<br />
Considering the time required for procurement, salary of staff for Floating ambulance is<br />
requested for six months only.
d. New Construction / repairs of quarters of RH/SDH and PHCs in remote areas<br />
Areas in Nandurbar are so interior that there is no facility for staying of the <strong>health</strong> staff in the<br />
village. Presently provided quarters require large repairs and also not adequate. It is proposed<br />
to repair the existing quarters and to build quarters for one driver, two nurses and one<br />
attendant in each of the hospital and PHCs.<br />
Budget required for this activity is as follows:<br />
Sir Activity<br />
Table – Budget requirement for Civil Works<br />
Unit<br />
cost<br />
units<br />
236<br />
Budget<br />
required<br />
A Repairs of the quarters<br />
1 PHC quarters 17 14 238<br />
2 RH Quarters 52 4 208<br />
Total Repairs 446<br />
B New Construction of quarters<br />
1 PHC quarters 55 6 330<br />
2 RH quarters 55 4 220<br />
Total new construction 550<br />
Grand Total 996<br />
Summary Part B: Nandurbar District Schemes:<br />
Rs. In Lakhs<br />
Sr.No. Activity Budget required<br />
1 Health Shelter <strong>13</strong>2.2<br />
2 Wireless contact 34.7<br />
3 Floating Dispensaries and Floating ambulances 322.04<br />
4 New Construction / repairs of quarters of RH/SDH and<br />
PHCs in remote areas<br />
2. GONDIA DISTRICT:<br />
Construction under Health Facility:<br />
996<br />
Total 1484.94
Construction of Separate LAB Room in Rural Hospital<br />
Laboratory services are one of the major services required to cater prompt <strong>health</strong>care<br />
services. The present laboratory room in RH is not spacious. it is needed to construct<br />
there separate Laboratory room at each RH.<br />
Construction Of NICU in RH<br />
Stabilization of Newborn is to be started at RH. There are no separate wards for<br />
Newborn care at some RH. Thus construction of NICE for proper management of<br />
Newborn illness is required.<br />
Construction of Dharamshala Building at RH<br />
Gondia has poor road connectivity so easy transport services are available all the<br />
time. Relatives of patients prefers to stay close to their sick relative. Thus, for<br />
convenience to stay of such relatives coming from different localities is essential.<br />
Herewith proposed budget is for construction of DHARMSHALAS for relatives at 10<br />
<strong>health</strong> facilities.<br />
Construction of nursing school building in BGW hospital campus<br />
There is no separate nursing school building in Gondia District Hospital. Thus a<br />
building of Nursing school for proper operationalization of school is proposed for<br />
Gondia at BGW Women Hospital Campus.<br />
Quarters:<br />
Construction of MPW quarter in sub center building in highly naxal affected blocks<br />
(Deori, Salekasa, Arjuni/ Mor.)<br />
MPW and ANM works at sub centre to cater <strong>health</strong> services .In the difficult and naxal<br />
affected area there is always scarcity of transportation. Thus to cater the services<br />
round the clock one of the MPW/ANM is expected to reside at Sub centre premises.<br />
Thus construction of MPW quarter is required at such area.<br />
Construction of Staff Quarter in RH<br />
There is no staff quarters available at RH,Amgaon of Gondia district .To cater the<br />
services round the clock staff should reside in the campus of Hospital. Thus quarters<br />
for these staff at Hospital vicinity is proposed.<br />
Construction of Staff Quarters in WH,DH & RH<br />
237
Residential Quarter for Hospital employees. With a view to provide 24 hour <strong>health</strong><br />
services to the patients attending RH . The <strong>health</strong> staff need to available in hospital<br />
premises because of non availability of residential quarter most of the employees in 3<br />
RH stay outside the premises and they are not in position to render quick services to<br />
the needy patients.<br />
Construction of Staff Quarters in PHC<br />
With a view to provide 24 hour <strong>health</strong> services to the patients attending PHC . The<br />
<strong>health</strong> staff need to available in hospital premises. But because of non availability of<br />
residential quarter most of the employees in 4 PHCS stay outside the premises and<br />
they are not in position to render quick services to the needy patients.<br />
Compound Walls for Health Facility<br />
Construction of Compound Wall At S.C.<br />
Compound wall having height 1.5mtr with grill work on top constructed from bricks &<br />
RCC Structure. Most of the SC’s in Gondia district are located in difficult, forest,<br />
remote & naxal affected area. So for the protection from stray animals and antisocial<br />
elements it is essential to construct compound wall to each SC in the district.<br />
Construction of Compound Wall At PHC<br />
Most of the PHC’s in Gondia district are located in difficult, forest , remote & naxal<br />
affected area. So for the protection from stray animals and antisocial elements it is<br />
essential to construct compound wall to each PHC in the district.<br />
Construction of Compound Wall At PHU<br />
Most of the PHU in Gondia district are located at difficult places , forest ,remote and<br />
naxal affected area. So for the protection from stray animals and antisocial elements it<br />
is essential to construct compound wall to each PHU in the district.<br />
Preliminary estimates and drawings are requested to district. Will be submitted before<br />
NPCC meeting.<br />
Table: Budget required for Gondia under Special Action Plan<br />
Section Activities No. Of Unit<br />
Cost per<br />
Unit<br />
238<br />
Total<br />
Budget<br />
1 Construction of Separate LAB Room in RH 5 9 45<br />
2 Construction Of NICE in RH 10 10 100<br />
3 Construction of Dharamshala Building at RH 15 10 150
Section Activities No. Of Unit<br />
Cost per<br />
Unit<br />
239<br />
Total<br />
Budget<br />
5<br />
Construction of MPW quarter in sub center<br />
building in highly naxal affected blocks (Deori,<br />
Salekasa, Arjuni/ Mor.)<br />
39 9 351<br />
6 Construction of Staff Quarter in RH 1 100 100<br />
7 Construction of Staff Quarters in WH,DH& RH 3 60 180<br />
8 Construction of Staff Quarter in PHC 4 22.35 89.4<br />
10 Construction of Compound Wall At PHC 4 7.5 30<br />
1 .Gadchiroli District:<br />
Compliance of remarks<br />
Total 1045.4<br />
Mobile unties proposed here are not regular MMU. These units have been procured by<br />
District Collector Gadchiroli from LEA funds provided by GoI as per the decision during<br />
meeting of Hon. Union Home Minister. There are six vehicles, two dental units, two<br />
ophthalmic units and two pathology units. Response of the community is also very good.<br />
However, now it has been informed by Collector that there is no budget for continuation of<br />
the scheme so this can be budgeted from NRHM. These vehicle worth over Rs. 1.0 cry with<br />
equipment are currently lying unused. If this budget is provided then services can be stated<br />
with these vehicles. In entire LEA area of Gadchiroli, there is no pathology lab or dentist<br />
available except for DH Gadchroli and SDH Aheri.<br />
Considering above fact, this proposal may be approved.<br />
A. Operationalization of Mobile Units<br />
Gadchiroli district is completely LEA area and length of the district is about 350 KM. Except for<br />
DH Gadchiroli and SDH Aheri, there is no availability of dentist, pathology unit or the<br />
Ophthalmological unit. Considering this, six mobile units have been supplied under IAP to<br />
Gadchiroli districts. These include 2 Dental Units, 2 Pathology Units and 2 Ophthalmologist<br />
units. However, these units are not functional due to non-availability of funds for manpower<br />
and operational expenses. As no such services are available in periphery, these units are<br />
extremely essential for the district. Considering this, it is proposed to support these units<br />
from Mission Flexi Pool. Budget required for these units is as follows:<br />
Table – Budget required for operationalization of Mobile Units<br />
Sir Particulars<br />
Unit<br />
rate<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
A Mobile Dental Unit (2)<br />
1 Salary of Dentist (Rs. 20000/PM) 2.4 2 4.8
Sir Particulars<br />
Unit<br />
rate<br />
No. of<br />
units<br />
240<br />
Budget<br />
required<br />
2 Salary of Dental Technician (Rs. 12000/PM) 1.44 2 2.88<br />
3 Salary of Attendant (Rs. 6000/PM) 0.72 2 1.44<br />
4 Salary of driver (Rs. 8000/PM) 0.96 2 1.92<br />
5 Medicines and consumables (Rs. 1.2 L/year) 1.2 2 2.4<br />
6 POL 1.2 2 2.4<br />
7 Overheads 1 2 2<br />
Total 17.84<br />
B Mobile Ophthalmic Unit (2)<br />
1 Salary of Ophthalmic Officer (Rs. 14000/PM) 1.68 2 3.36<br />
3 Salary of Attendant (Rs. 6000/PM) 0.72 2 1.44<br />
4 Salary of driver (Rs. 8000/PM) 0.96 2 1.92<br />
5 Medicines and consumables 0.6 2 1.2<br />
6 POL 1.2 2 2.4<br />
7 Overheads 1 2 2<br />
Total 12.32<br />
A Mobile Pathology Unit (2)<br />
1 Salary of Doctor (Rs. 25000/PM) 3 2 6<br />
2 Salary of Laboratory Technician (Rs. 12000/PM) 1.44 2 2.88<br />
3 Salary of Attendant (Rs. 6000/PM) 0.72 2 1.44<br />
4 Salary of driver (Rs. 8000/PM) 0.96 2 1.92<br />
5 Lab consumables 6 2 12<br />
6 POL 1.2 2 2.4<br />
7 Overheads 1 2 2<br />
Total 28.64<br />
Grand Total 58.8<br />
B. Construction<br />
Construction of Women Hospital at Gadchiroli is required.<br />
District Hospital bed occupying rate is around 120 to 140, There is no private Health<br />
Facility in this District & Hence People in this district solely Dependent on the District<br />
Hospital for Health Care, Patient also coming from adjacent District like Chandrapur,<br />
Bhandara & Chhattisgarh State. Considering<br />
In the total patient load of this district the no. of Women coming for delivery is high<br />
for that Separate Women Hospital required.
New construction of Ware House<br />
A large quantity of medicine is supplied to PHCs and Hospitals as this is special focus<br />
district. At present there is no sufficient and convenient storage facility available for<br />
storage of this huge quantity of medicines and consumable. It is proposed to construct<br />
one Warehouse in the premises of District Hospital for both the DHO and Civil<br />
Surgeon. Thus construction of new warehouse at District level is proposed for safe<br />
storage and distribution of Medicine and consumables.<br />
Construction of Dharmashala at DH<br />
As DH is the only place to receive specialty care in district, large number of tribal<br />
patients attends the DH and SDH Aheri daily. These poor patients do not have any<br />
facility to stay. As monsoon of this area is very strong, patients are at very much<br />
hardship. Therefore it is proposed to construct shelter (Dharmashala) for poor<br />
patients one each at Gadchiroli and Aheri. This will consist of two halls one kitchen<br />
room with platform and two sanitary blocks (separate for men and women).<br />
New construction of MPW Quarter at Sub Centre<br />
One ANM and a MPW are appointed at sub centre to cater basic <strong>health</strong> care at village<br />
level. One of these is supposed to be available on 24 hrs. basis for serving the<br />
population. Thus construction of MPW quarters at well-performing subcentres are<br />
proposed in the special action plan.<br />
New construction of Medicine store Room at Primary Health Centre<br />
PHCs are catering <strong>health</strong> services in the form of OPD as well as IPD(6 beds or<br />
more).Availability and storage of medicine is very important at the PHC itself. At<br />
present 32 PHCs in the district haven’t their medicine store. Therefore, construction of<br />
32 medicine store rooms are required in these PHCs.<br />
New construction of 20 Bedded EYE Ward at District Hospital<br />
Gadchiroli District hospital caters various specialty services to <strong>rural</strong> population. There<br />
is no separate ward for ophthalmology patients in this hospital. Ophthalmology<br />
patients need to stay in the hospital for cataract surgeries and in case of ophthalmic<br />
emergencies. Separate 20 bedded eye ward is proposed for this purpose.<br />
New construction of Trauma Ward at District Hospital<br />
Gadhchiroli is tribal and naxalite affected area. Naxalite activities used to occur in this<br />
district which leads to large no. of trauma emergencies . To handle these emergencies<br />
241
at present no separate trauma ward in DH. All these emergencies comes to DH ,hence<br />
trauma ward construction is proposed.<br />
New construction of Nursing School & Hostel Building at District Hospital<br />
At present ANM schools is running in the campus of DH but haven’t separate building<br />
.There is a requirement of construction of Nursing school building as well as Hostel for<br />
the students of this school in campus of DH.<br />
New construction of Type- IV Quarter at District Hospital<br />
DH Gadhchiroli is a big <strong>health</strong> facility and a large no. of Class IV employees works for<br />
the hospital. Residence quarters for these employees are less as compare to no. of<br />
employees .So to accommodate all class IV employees additional 18 quarters are<br />
needed.<br />
Table: Budget required for Gadchiroli under Special Action Plan<br />
Sir Name of Activities/initiative Unit cost<br />
1<br />
2<br />
3<br />
5<br />
6<br />
7<br />
8<br />
9<br />
14<br />
No. of<br />
units<br />
242<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
New Construction of Women Hospital at<br />
Gadchiroli (partial cost)<br />
500 1 500<br />
New construction Hospital Training Center<br />
(Partial grant)<br />
100 1 100<br />
New construction of Ware House at District<br />
Health Officer<br />
90 1 90<br />
New construction of MPW Quarter at Sub<br />
Center<br />
8 10 80<br />
New construction of Medicine store Room at<br />
Primary Health Center<br />
4 15 60<br />
New construction of 20 Bedded EYE Ward at<br />
District Hospital<br />
100 1 100<br />
New construction of Trauma Ward at District<br />
Hospital and Dharmashala<br />
115 1 115<br />
New construction of Specialist Room at District<br />
Hospital<br />
15 5 75<br />
New construction of Type- IV Quarter at District<br />
Hospital<br />
22 18 396<br />
Total 1516
C. Mobility Support<br />
As this district is totally naxalite affected, there is no sufficient public transport system. The<br />
distances of <strong>health</strong> facilities are also very far off. Therefore it is proposed to provide<br />
Ambulances and supervisory vehicles to PHCs, Hospitals and Blocks. Requirement of vehicles<br />
is as follows:<br />
Table – Budget required for Mobility Support<br />
Sir Name of Activities/initiative Unit cost<br />
No. of<br />
units<br />
243<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
1 Ambulances to PHC 5.5 6 33<br />
2 Ambulances to RH/SDH 7.5 4 30<br />
3<br />
Supervisory vehicle to District Officials (DHO<br />
and CS side)<br />
5.2 5 26<br />
5 Supervisory vehicles to Block Health Officer 5.2 10 52<br />
6 Blood bags supply vehicle 5.2 1 5.2<br />
Total 146.2<br />
D. Total budget required for Gadchiroli district<br />
Total budget required for special plan of Gadchiroli district is mentioned below:<br />
Table – Total Budget required for Gardchiroli District<br />
Rs. In lakhs<br />
Sir Activity/scheme Budget proposed<br />
1 Operationalization of Mobile Units 58.8<br />
2 New Construction / repairs 1516<br />
3 Mobility Support 146.2<br />
Total 1721<br />
Summary of budget required for Special Action Plan of High Focus districts<br />
Total budget required for special action plans of high focus districts is mentioned in table<br />
below:
Table – Summary budget required to High Focus Districts<br />
Sir District Budget Required<br />
244<br />
Rs. In lakhs<br />
1 Nandurbar 1484.94<br />
2 Gondia 1045.4<br />
3 Gadchiroli 1721<br />
Total 4251.34
MAHARASHTRA<br />
NATIONAL RURAL<br />
HEALTH MISSION<br />
PIP <strong>2012</strong>-<strong>13</strong><br />
Page | 1
Sr.no Components<br />
Component wise PIP <strong>2012</strong>-<strong>13</strong><br />
Amount<br />
Proposed to<br />
NPCC<br />
Approved<br />
by NPCC<br />
Additional<br />
Budget<br />
requested<br />
Total<br />
budget<br />
A RCH 510.74 403.69 53.41 457.09<br />
B MFP 869.40 358.44 590.23 948.67<br />
C RI 32.54 42.44 2.94 45.39<br />
requested Remark<br />
Revised as per<br />
discssussion<br />
during 6-8<br />
June.<br />
Original MFP<br />
PIP is of Rs.<br />
769.39 Cr.<br />
Requirement of<br />
high utilization<br />
hosptials (B.15,<br />
Rs. 179.28 Cr<br />
added as per<br />
discussion)<br />
Revised as per<br />
new guidelines<br />
D1 NIDDCP 0.3 1.47 0 1.47 No Change<br />
D2 ISDP 4.6 4.17 0 4.17 No Change<br />
D3 NVBDCP 12.57 20.65 0 20.65 No Change<br />
D4 NLEP 4.33 4.<strong>13</strong> 0 4.<strong>13</strong> No Change<br />
D5 NPCB 39.14 20 0 20.00 No Change<br />
D6 RNTCP 55.04 55.29 0 55.29 No Change<br />
Page | 2
Sr.no Components<br />
Amount<br />
Proposed to<br />
NPCC<br />
Approved<br />
by NPCC<br />
Additional<br />
Budget<br />
requested<br />
Total<br />
budget<br />
requested Remark<br />
Infrastructure<br />
Maintenance 300 356.05 0 356.05 No Change<br />
Total 1828.66 1266.33 646.58 1912.91<br />
Page | 3
PART – B : MISSION FLEXIPOOL<br />
SECTION - B.1: ACCREDITED SOCIAL HEALTH ACTIVIST (ASHA)<br />
A trained female community <strong>health</strong> worker called as Accredited Social Health Activist (ASHA) is<br />
being provided to tribal as well as non-tribal areas in the approximate ratio of one per 1000<br />
population.<br />
B.1.1.1 : Selection and training of ASHA<br />
Approved and Accepted.<br />
B.1.1.2 : ASHA Drug Kit Medicine<br />
Approved and Accepted.<br />
B.1.1.3 : Incentive to ASHA<br />
Approved for incentive as per the list attached. Accepted.<br />
B.1.1.4 : Awards to ASHA<br />
Approved and accepted.<br />
B.1.1.5 : Support Mechanism for ASHA<br />
All the activities at State and District Level are approved. Regarding Block Level activities, Block<br />
level contingency is approved whereas Salary TA/DA of Block Community Mobiliser is not<br />
approved. At PHC level, TA/DA to ASHA facilitator not approved, Honorarium to MO not<br />
approved and contingency at PHC level not approved.<br />
Regarding the activities which are not approved, PHC level decision of not approving activities<br />
such as TA/DA to ASHA facilitator and Honorarium to MO is acceptable. Therefore it is not<br />
submitted in revision. However, GoI has not approved Salary and TA of Block Community<br />
Mobiliser of non-tribal block which need to be reconsidered. This activity is resubmitted with<br />
explanation below:<br />
Salary and TA of Block Community Mobiliser.<br />
Budget requested : Rs. 100.0 Lakh, Remarks of ROP : Not Approved<br />
GOI was requested Rs. 100.0 Lakh. However, total amount approved is Rs. 30.0 Lakh. Presently<br />
Block Community Mobilisers are working in tribal blocks only. These are 60 blocks. It is<br />
proposed to appoint Block Community Mobiliser in another 40 non-tribal blocks. If criteria<br />
Page | 4
mentioned in ROP are to be applied, budget required for this activity will be Rs. 50.0 Lakh as<br />
mentioned in table below:<br />
Budget Requirement for Salary of Block Community Mobiliser in Non-tribal areas<br />
Sir Particulars<br />
Budget<br />
/ unit<br />
Total<br />
Units<br />
Budget<br />
required<br />
2 Block Community Mobiliser (salary + TA/DA) - Tribal 0.5 60 30<br />
Block Community Mobiliser (salary + TA/DA) - Non-<br />
Tribal<br />
0.5 40 20<br />
Block total 50<br />
As discussed during the meeting of 7-8 June <strong>2012</strong>, the non-tribal blocks with high IMR are<br />
selected. List of selected blocks is submitted as Annex – B.1.1<br />
B.1.2 : Strengthening of ASHA Resource Centre<br />
There are approximately 60,000 ASHAs functioning in the state. ASHA program's success<br />
depends on strong supportive system. For this purpose ASHA Resource Centre (ARC) plays very<br />
vital role. In Maharashtra ARC is attached to SHSRC and Senior Public Health Consultant in<br />
heading the ARC. As per GOI letter dated 15 th March 2011 entire team of ARC needs to be<br />
recruited for the effective supervision of the program in the State. Therefore, following<br />
structure and budget is proposed for strengthening of ASHA Resource Centre.<br />
No Category<br />
1<br />
Project Manager<br />
(Sr. Public Health Consultant)<br />
SUBSECTION - B.2.1 : CHC<br />
Approved<br />
Unit cost<br />
in Rs. In<br />
lakhs<br />
No of units<br />
Total cost in Rs.<br />
In lakhs<br />
0.5 1 5<br />
Total 6<br />
SECTION - B.2 : UNTIED FUNDS TO HEALTH INSTITUTIONS<br />
Page | 5
SUBSECTION - B.2.2 : PHC & APHC<br />
Out of Rs. 452.50 Lakh requested, Rs. 426.53Lakh approved for PHC. Accepted.<br />
Out of Rs. 198.75 Lakh requested, Rs. 186.83 Lakh approved for PHC. Accepted.<br />
SUBSECTION - B.2.3 : Sub Center<br />
Out of Rs. 1056.60 Lakh requested, Rs. 1011.27 Lakh approved for Sub-Center. Accepted.<br />
SUBSECTION - B.2.4 : UNTIED FUNDS TO VHC<br />
Out of Rs. 3967.44 Lakh requested, Rs. 3548.61 Lakh approved for VHNSC. Accepted.<br />
SUBSECTION - B.3.1 : CHC<br />
Approved<br />
SUBSECTION - B.3.2 : PHC & APHC<br />
-B.3 : ANNUAL MAINTENANCE GRANTS (AMG)<br />
Out of Rs. 807.0 Lakh requested, Rs. 737.03 Lakh approved for PHC. Accepted.<br />
Out of Rs. 240.0 Lakh requested, Rs. 218.28 Lakh approved for APHC (PHU). Accepted.<br />
SUBSECTION - B.3.3 : Sub Center<br />
Out of Rs. 828.60 Lakh requested, Rs. 768.69 Lakh approved for SC. Accepted.<br />
SECTION - B.4 : HOSPITAL STRENGTHENING<br />
SUBSECTION - B.4.1.1 : UPGRADING HEALTH FACILITIES TO IPHS<br />
Page | 6
Remarks of GoI in RoP : Approval Pended. State to provide detailed breakup of the cost<br />
components as there is lack of clarity on the cost components for which the funds are to be<br />
utilized.<br />
Detailed break up of cost components and procedure adopted by GoM to arrive at gaps and<br />
converting gaps to budget requirement is submitted in this chapter. Information already<br />
provided regarding criteria for selection of <strong>health</strong> facility, Steps in up gradation, number of<br />
institutions upgraded by 31.3.<strong>2012</strong>, IPHS Evaluation system, Utilization of IPHS facility, more<br />
emphasis on burn ward and Dialysis this year, implementation of Book Your Bed (BYB), etc. are<br />
not mentioned here as this is already mentioned in PIP.<br />
GoI has specifically mentioned about Up gradation of <strong>health</strong> facilities to IPHS in NRHM<br />
Framework for Implementation. GoI has given time line for this and also given formats for gap<br />
calculation in these guidelines. As mentioned by GoI, these standards have been fixed by a high<br />
powered task group through a consultative process with states and other experts. IPHS is novel<br />
concept to fix bench marks for infrastructure including building, manpower, equipment, drugs,<br />
etc. Most importantly they define the level of services each <strong>health</strong> facility expected to provide.<br />
Under RCH-II, upgradation of PHCs as 24×7 PHCs and CHC as FRU is being attempted to provide<br />
emergency services to mothers and children. IPHS Upgradation activity in Maharashtra is being<br />
carried out as per the guidelines of GoI in NRHM Framework and IPHS Guidelines for Health<br />
facilities.<br />
Salient features of cost calculations are:<br />
• Cost calculation is based on annual survey of each of the <strong>health</strong> facility.<br />
• Provision from state funds, provision from other sources including other schemes<br />
of NRHM, provision from user fees and other local grants, etc are substracted from<br />
annual requirement of facility and only gap is paid from IPHS funds.<br />
• Gap is calculated for human resource, medicine, equipment, physical infrastructure<br />
and support services separately and annual plan submitted by the facility is<br />
scruitinised at district and state level.<br />
• Identified gap is converted into budget and only required budget is released.<br />
Budget requirement varies from facility to facility depending upon load (e.g.<br />
deliveries, OPD, IPD, etc). Budget requrested is average of the requirement.<br />
Detailed explanation of Cost components, their break up and how the gap is calculated is<br />
submitted below:<br />
How the cost is calculated for IPHS Upgradation<br />
Page | 7
Government of India has published IPHS Guidelines for Sub Center, PHC, CHC and Hospitals as<br />
per beds (51-100, 101-200, 201-300 and 301-500). In these guidelines, GoI has defined essential<br />
services for each type of <strong>health</strong> facility.<br />
Following steps have been carried out to identify the gaps and to convert the gaps into budget<br />
requirement.<br />
a. Basic Information<br />
1. External Facility Survey is carried out during 2008-09 and 2009-10 with the help of<br />
External Agency. Format provided in NRHM Framework for Implementation 2005-<strong>2012</strong><br />
were used for the survey.<br />
2. Gaps in providing essential services to each type of facility as per IPHS were identified.<br />
Meetings of Medical Officers, Medical Superintendents, RCH Officers and Civil Surgeons<br />
were conducted to disseminate the findings. The gaps were converted into budget<br />
requirement.<br />
3. State level workshop was carried out under Chairmanship of Hon. Additional Chief<br />
Secretary (PH & FW) for overall picture of the State. In this meeting, <strong>health</strong> facilities to<br />
be upgraded were shortlisted by applying criteria of availability of building, OPD, IPD,<br />
deliveries and emergency load.<br />
4. It was decided in the workshop that as per GoI guidelines for IPHS upgradation, all the<br />
designated PHCs will be first upgraded to 24×7 PHCs and all the Hospitals will be first<br />
upgraded to FRU.<br />
5. Accordingly, gaps related to PHCs (9 services) and FRU (10 services) were identified from<br />
external survey and process of Upgradation started.<br />
b. Planning for year <strong>2012</strong>-<strong>13</strong><br />
Initially for two years, planning was carried out by IPHS cell in the district and only budget<br />
was proposed in District Plans. However from 2011-12 onwards, each of the <strong>health</strong> facility<br />
plan was prepared by the district and submitted to State Health Society IPHS Cell. For year<br />
<strong>2012</strong>-<strong>13</strong>, detailed plans are prepared at Facility level, scrutinized first at district and then<br />
state level.<br />
The detailed activities carried out are as follows:<br />
1. One committee was established at state level of officers such as Joint Director (T), Joint<br />
Director (Hospitals), Joint Director (SC-PHC) and Senior Consultant IPHS.<br />
2. Detailed format with eight sections was prepared by committee and circulated to all the<br />
districts.(Format enclosed as Annex – B.4.1)<br />
3. At the district level, two day workshop of annual assessment of <strong>health</strong> facility was<br />
undertaken. Annual plan was prepared based on pre-tested format and committee of<br />
District RCH Officer, RMO (Outreach) and IPHS Coordinator scrutinized the format.<br />
Page | 8
4. These plans were again checked by State level committee and final approvals were<br />
given.<br />
c. Budget calculations for year <strong>2012</strong>-<strong>13</strong><br />
Following actions were taken for calculation of budget for IPHS upgradation of <strong>health</strong> facilities<br />
a. As mentioned in GoI Guidelines, annual survey of each IPHS Institutions is done. One<br />
separate format for annual survey is devised based on the GoI format. Each of the IPHS<br />
<strong>health</strong> facility has to fill up the format. This format is checked at district and state level<br />
and budget is released only after finalization of format.<br />
b. Budget was requested for Hiring of Manpower (Table -2), Procurement of Medicine<br />
(Table-3), Procurement of Equipment (Table -4), Maintenance of Equipment (Table-5),<br />
Physical Infrastructure (Table-6), Support services (Table -7) and Miscellaneous services<br />
(Table-8). All these requirements are summarized in Table -1.<br />
c. For each category, annual requirement, supply from government, supply from other<br />
sources if any and gap was identified. Unit price of each unit required was calculated<br />
and finally budget required for fulfilling of the gaps was calculated.<br />
d. Exercise as mentioned above is carried out for all the <strong>health</strong> facilities included in IPHS<br />
Upgradation. Considering the number and small requirement in SC, monitoring of<br />
upgradation of SC is done at District level. However from PHC onwards total monitoring<br />
is done from State level. Annual plan of each facility is around 15 pages. We have<br />
prepared detailed plans for 658 PHCs and 220 Hospitals. Total plans come to <strong>13</strong>174<br />
pages. Therefore this is submitted in separate CD. To get an idea, plan of PHC and<br />
hospitals one in each category is submitted as Annex – B.4.2.<br />
Budget requested in the PIP was submitted as average of all the requirements. However,<br />
detailed budget requirement have been calculated for each <strong>health</strong> facility before submitting to<br />
GoI and was available in the Society. This detailed budget along with physical requirement is<br />
submitted for approval.<br />
1. Table - 1 : Requirement of Manpower : Manpower requirement include Specialists,<br />
Nurses and Paramedical Staff. Requirement of manpower is enlisted as per IPHS. Staff<br />
available is recorded and gap is identified. Salary of this staff is calculated. Range of<br />
salary is communicated to all the District Societies and RKS. Actual salary is fixed by RKS<br />
depending upon qualifications (degree/diploma), experience of the doctor and number<br />
of days of OPD and Surgery. (Detailed circular sent to districts is annexed ; (Annex –<br />
B.4.3). Staff presently working under IPHS is given in table below:<br />
Table – IPHS Staff availability as on 1.4.<strong>2012</strong><br />
Sr. No. Speciality On Contract (IPHS)<br />
Page | 9
Sr. No. Speciality On Contract (IPHS)<br />
1 Specialists 607<br />
2 Lab Technician (PHC+Hospitals) 634<br />
3 Staff Nurses <strong>13</strong>75<br />
4 Data Entry operator/Accountant (PHC+Hospitals) 847<br />
5 IPHS Coordinator 28<br />
6 Statistical Investigator (IPHS Coordinator) 15<br />
7 Data Entry operator (IPHS Coordinator) 31<br />
Total 3537<br />
Out of the staff above, post of Statistical Investigator and DEO at district level are discontinued<br />
in year <strong>2012</strong>-<strong>13</strong>. Also 342 Accountants at PHC and Hospitals are discontinued. Remaining staff is<br />
continued. The DEO cum Accountant are engaged in account of <strong>health</strong> facility and also entering<br />
data for MCTS and other online software.<br />
Break up of Specialists appointed as on 1.4.<strong>2012</strong> in IPHS designated hospitals is submitted in<br />
the table below.<br />
Table – Specialists appointed in IPHS upgradation hospitals.<br />
Sr. No. Specialty On Contract (IPHS)<br />
1 Surgeon 74<br />
2 Physician 46<br />
3 Gynecologist 89<br />
4 Pediatrician 95<br />
5 Anesthetist 120<br />
6 Ophthalmic Surgeon 8<br />
7 ENT Surgeon 7<br />
8 Dermatologists 4<br />
9 Orthopedics <strong>13</strong><br />
10 Radiologist 17<br />
11 Dentist 119<br />
Page | 10
Sr. No. Specialty On Contract (IPHS)<br />
12 Public Health Manager 9<br />
<strong>13</strong> Psychiatrist 6<br />
Total Specialists 607<br />
Summary of budget required for Manpower to IPHS <strong>health</strong> facilities is submitted in table below:<br />
Table – Budget required for Manpower to upgrade <strong>health</strong> facilities to IPHS<br />
Rs. In Lakhs<br />
Sr. No. Type of facility<br />
No. designated for up<br />
gradation<br />
Budget requested by the facilities<br />
1 PHC 658 1245.69<br />
2 RH 110 <strong>13</strong>86.95<br />
3 SDH – 50 51 848.61<br />
4 SDH – 100 23 503.91<br />
5 WH 9 246.60<br />
6 GH 4 152.26<br />
7 DH 23 894.61<br />
Total 878 5278.64<br />
Detailed budget required for each <strong>health</strong> facility is submitted as Annex B.4.4A for Hospitals and<br />
Annex B.4.4B for PHCs.<br />
2. Table – 2 : Medicine Requirement<br />
Budget for medicine is provided through following source:<br />
i) State Government Medicine Grants<br />
ii) User fees charges collected in hospitals<br />
iii) Other schemes of NRHM<br />
iv) Remaining through IPHS funds as gap filling.<br />
State Government has developed list of medicines required for <strong>health</strong> facilities by establishing<br />
committee of experts. This committee considered WHO essential drugs list, IPHS Medicine List<br />
and Lists of medicines recommended by various GoI program experts. This list is updated<br />
periodically and latest updated list is published by Government Order on 30.4.<strong>2012</strong>. List<br />
submitted as Annex B.4.5.<br />
Page | 11
State Government has approved budget for medicines to <strong>health</strong> facilities as per the criteria<br />
given below:<br />
Table – Medicine Budget from state grants<br />
Sr Type of Health Facility Tribal areas Non-tribal areas<br />
1 Sub-Center 0.12<br />
2 Primary Health Center 1.2 1.6<br />
3 Rural Hospitals 4.0 6.0<br />
4 Hospitals with
Sr. No. Type of facility<br />
No. designated for up<br />
gradation<br />
Budget requested by<br />
the facilities<br />
5 WH 9 427.92<br />
6 GH 4 423.87<br />
7 DH 23 1233.39<br />
Total 878 8007.80<br />
Detailed budget required for each <strong>health</strong> facility is submitted as Annex B.4.4A for Hospitals and<br />
Annex B.4.4B for PHCs.<br />
3. Table -3 : Equipment / instrument requirement<br />
IPHS Guideline have identified essential services and also equipment required for services to be<br />
provided by that particular <strong>health</strong> facility. This list of equipment changes with type of facility.<br />
List of equipment for each facility is circulated to all IPHS designated <strong>health</strong> facility in the state.<br />
Instruments already available are subtracted from the list. Equipment which can be repaired is<br />
considered as available. Specialty specific equipment, (e.g. C-arm for orthopaeditian, Dental<br />
chair for dentist) are not included in plan unless we get specialist and technician if required.<br />
Thus, requirement of equipment and instrument is directly dependent on availability of<br />
manpower.<br />
Similar to medicines, gap of instrument and equipment is identified. Unit price of equipment is<br />
decided and the gap is converted into budget.<br />
Budget required for equipment / instrument procurement by the state in <strong>2012</strong>-<strong>13</strong> for IPHS<br />
designated <strong>health</strong> facilities are submitted in table below:<br />
Table – Budget required for equipment / instruments to upgrade <strong>health</strong> facilities to IPHS<br />
Sr. No. Type of facility<br />
No. designated for up<br />
gradation<br />
Rs. In Lakhs<br />
Budget requested by the<br />
facilities<br />
1 PHC 658 537.94<br />
2 RH 110 831.91<br />
3 SDH – 50 51 509.58<br />
4 SDH – 100 23 251.96<br />
5 WH 9 284.89<br />
6 GH 4 84.27<br />
7 DH 23 2001.18<br />
Total 878 4501.74<br />
Page | <strong>13</strong>
Detailed budget required for each <strong>health</strong> facility is submitted as Annex B.4.4A for Hospitals and<br />
Annex B.4.4B for PHCs.<br />
4. Table -4 : Maintenance of equipment<br />
As per GoI IPHS Guidelines, every equipment if out of order should be repaired within 30 days.<br />
Considering this following actions have been taken regarding maintenance of equipment.<br />
i. All the equipment will have two year warranty at the time of purchase.<br />
ii. All the equipment users will have address of the person to whom they should contact<br />
in case the equipment is out of order.<br />
iii. Maharashtra state has 8 Health Equipment Maintenance Units in the state. Each unit<br />
visits one block once in month and repairs the equipment. This unit repairs all minor<br />
equipment and major equipment such as all types of autoclaves, shadow less lamps,<br />
centrifuge machines, suction machines, etc.<br />
iv. Advanced equipment like C-Arm, CT Scan, Sonography, high end X-ray machine, are<br />
entered into contract with manufactures for maintenance.<br />
All the districts are instructed to keep the equipment and instrument of IPHS <strong>health</strong> facilities<br />
functional. Budget required for AMG and other minor issues is first claimed from Government<br />
budget, then from user fees and lastly from IPHS funds.<br />
Separate format is given for identifying gaps and converting the gaps into budget requirement.<br />
Summary of budget requirement for instrument / equipment is submitted in table below:<br />
Table – Budget required for maintenance of equipment / instrument to upgrade <strong>health</strong><br />
facilities to IPHS<br />
Rs. In Lakhs<br />
Sr. No. Type of facility<br />
No. designated for up<br />
gradation<br />
Budget requested by the facilities<br />
1 PHC 658 2<strong>13</strong>.32<br />
2 RH 110 118.86<br />
3 SDH – 50 51 89.23<br />
4 SDH – 100 23 42.33<br />
5 WH 9 18.47<br />
6 GH 4 9.39<br />
7 DH 23 154.44<br />
Total 878 646.03<br />
Detailed budget required for each <strong>health</strong> facility is submitted as Annex B.4.4A for Hospitals and<br />
Annex B.4.4B for PHCs.<br />
Page | 14
5. Table – 5 : Physical infrastructure<br />
GoI IPHS Guidelines have identified areas required for each type of facility and also about<br />
support services (Laundry, kitchen, etc.) and quarter. Gap for these areas is identified and<br />
physical infrastructure is requested. Here also budget received from State Government and<br />
other sources is subtracted and only gap budget is requested to GOI.<br />
One register is kept at Facility and district level to avoid duplication of the civil works. One page<br />
of this register is for each building. This helps to avoid duplication of the works from different<br />
sources. As this data will be voluminous, at state level this monitoring is done with the help of<br />
software called as ‘Construction Tracker’.<br />
Budget required for physical infrastructure is submitted in table below:<br />
Table – Budget required for physical infrastructure to upgrade <strong>health</strong> facilities to IPHS<br />
Sr. No. Type of facility<br />
No. designated for up<br />
gradation<br />
Rs. In Lakhs<br />
Budget requested by the facilities<br />
1 PHC 658 3453.24<br />
2 RH 110 2242.95<br />
3 SDH – 50 51 1705.03<br />
4 SDH – 100 23 1177.42<br />
5 WH 9 751.51<br />
6 GH 4 167.41<br />
7 DH 23 2665.01<br />
Total 878 12162.56<br />
Detailed budget required for each <strong>health</strong> facility is submitted as Annex B.4.4A for Hospitals and<br />
Annex B.4.B for PHCs.<br />
6. Table – 6 : Support services<br />
Support services include Security services, Kitchen services, Cleaning services, laundry services,<br />
etc. Normally budget from state government is provided for these services. However, at some<br />
places, this budget is not sufficient due to high patient load. This gap is only filled in from IPHS<br />
budget. Budget required for these services is mentioned below:<br />
Table – Budget required for Support services to upgrade <strong>health</strong> facilities to IPHS<br />
Sr. No. Type of facility<br />
No. designated for up<br />
gradation<br />
Rs. In Lakhs<br />
Budget requested by the<br />
facilities<br />
1 PHC 658 466.56<br />
Page | 15
Sr. No. Type of facility<br />
No. designated for up<br />
gradation<br />
Budget requested by the<br />
facilities<br />
2 RH 110 248.68<br />
3 SDH – 50 51 151.51<br />
4 SDH – 100 23 112.83<br />
5 WH 9 94.82<br />
6 GH 4 52.76<br />
7 DH 23 272.61<br />
Total 878 <strong>13</strong>99.77<br />
Detailed budget required for each <strong>health</strong> facility is submitted as Annex B.4.4A for Hospitals and<br />
Annex B.4.4B for PHCs.<br />
7. Table – 7 : Other requirements<br />
Other requirements which are not mentioned in Table – 1 to 6 but are essential to keep the<br />
hospitals to IPHS standards are mentioned here. This includes expenses on un-interrupted<br />
electrical supply, water supply, etc. For this also the guidelines says that first regular state<br />
budget followed by user fees should be used. IPHS budget is to be used only when these budget<br />
are not available or insufficient.<br />
Budget required for this activity is submitted in table below:<br />
Table – Budget required for other requirements to upgrade <strong>health</strong> facilities to IPHS<br />
Sr. No. Type of facility<br />
No. designated for up<br />
gradation<br />
Rs. In Lakhs<br />
Budget requested by the facilities<br />
1 PHC 658 559.56<br />
2 RH 110 185.90<br />
3 SDH – 50 51 193.50<br />
4 SDH – 100 23 212.77<br />
5 WH 9 39.29<br />
6 GH 4 41.14<br />
7 DH 23 312.72<br />
Total 878 1544.87<br />
Detailed budget required for each <strong>health</strong> facility is submitted as Annex B.4.4A for Hospitals and<br />
Annex B.4.4B for PHCs.<br />
Summary of total budget required for IPHS upgradation is submitted in table below :<br />
Table – Summary of Budget required upgrading <strong>health</strong> facilities to IPHS<br />
Rs. In Lakhs<br />
Page | 16
Sr. No. Type of facility<br />
No. designated for up<br />
gradation<br />
Budget requested by the<br />
facilities<br />
1 PHC 658 8956.36<br />
2 RH 110 6779.53<br />
3 SDH – 50 51 4536.03<br />
4 SDH – 100 23 2940.90<br />
5 WH 9 1863.50<br />
6 GH 4 931.11<br />
7 DH 23 7533.96<br />
Total 878 33541.41<br />
Detailed budget required for each <strong>health</strong> facility is submitted as Annex B.4.4A for Hospitals and<br />
Annex B.4.4B for PHCs.<br />
Once the state budget is made available to state in April and also once PIP is approved by GoI<br />
which will give idea of other sources of funds, total Plans of the <strong>health</strong> facilities are revised by<br />
calling the meetings of MO/MS, Store in charge and Pharmacist to finalize the Plan. During<br />
finalization, GoI guidelines given for that year are also considered.<br />
This year budget required for IPHS up-gradation is Rs. 335.41. Considering the limitation for PIP<br />
size, Executive Committee of NRHM Maharashtra allotted Rs. 109. Cr for IPHS. Considering this,<br />
the budget will be finalized for all the <strong>health</strong> facilities once it is approved by the GoI.<br />
Impact of NRHM, criteria for selection, plans for this year and other minute details are already<br />
submitted in PIP. Therefore they are not mentioned again here. Final budget required for state<br />
remains same as mentioned in table below. The figures mention here are average amount<br />
required after revising the budget demand of each facility.<br />
Budget requirement<br />
Considering above factors and based on the IPHS guidelines, one Planning Format was prepared<br />
by SHS and distributed to all the districts. Plans received from the districts are analysed and<br />
only the <strong>health</strong> facilities fulfilling Delivery Point criteria or with potential of improvement in<br />
delivery services have been included in the upgradation list. We have ready plans for each of<br />
the facility in the state. SC plans are kept at the level of District Society and all the plans for PHC<br />
and higher <strong>health</strong> facilities are scrutinized by Quality Assurance wing of the SHS.<br />
Once the budget is approved by GoI, one day workshop of all facilities (circle wise) is<br />
conducted. Till that time, GoM funds and other activities are also known. Plans revised as per<br />
availability of GoM funds and funds from other (particularly RCH activities) and plans are<br />
finalized.<br />
Although we have detailed plans of each facility, the budget required is mentioned as average<br />
of these facilities.<br />
Budget required for up gradation for year <strong>2012</strong>-<strong>13</strong> is as follows:<br />
Page | 17
Table -: Budget required for up-gradation of <strong>health</strong> institutions as per external facility survey<br />
Rs. In Lakhs<br />
Sir Type of facility<br />
No. of facilities<br />
included for<br />
IPHS<br />
Upgradation<br />
Average<br />
Budget<br />
required per<br />
unit<br />
Total budget<br />
required<br />
1 SC 1521 0.25 380.25<br />
2 PHC 658 6 3948<br />
3 RH 110 20.15 2216.5<br />
4 SDH – 50 51 24.3 1239.3<br />
5 SDH – 100 23 41.7 959.1<br />
6 GH – 200 4 72.5 290<br />
7 WH - (300 +) 2 72.6 145.2<br />
8 WH - (200-299) 2 54.9 109.8<br />
9 WH - (
• Some private medical institutions / organizations are willing to appoint specialists on<br />
yearly basis.<br />
Details of these areas are as follows:<br />
Table – Special Focus Hospitals in Maharashtra<br />
Sir District Names of RH/SDH Total No. Remarks<br />
1 Gadchiroli SDH Aheri, RH<br />
Sironcha, RH<br />
Bhamragad, RH<br />
Dhanora, RH Etapalli<br />
2 Amravati<br />
(Melghat area<br />
only)<br />
SDH Dharani, RH<br />
Chikhaldara, RH<br />
Churni<br />
3 Nandurbar RH Akkalkuwa, RH<br />
Dhadgaon, RH Molgi<br />
5 Very remote and LEA affected<br />
areas. Except Dhanora, all other<br />
more than 100 KM away from<br />
DH. No specialist facility<br />
available since establishment.<br />
3 Very remote reserve forest area.<br />
Very high IMR and MMR. No<br />
specialty services available.<br />
3 Very remote area within<br />
Satpuda mountain range and<br />
Narmada river. No specialties<br />
available since establishment.<br />
High IMR and MMR.<br />
Performance of special focus hospitals<br />
Deliveries conducted in these hospitals for last three years is mentioned in table below. These<br />
hospitals do not have specialists. After appointment of specialists, these hospitals will further<br />
improve their performance.<br />
Table : No. of deliveries conducted in Special Focus Hospitals<br />
Sr. No.<br />
Name of the<br />
District<br />
Name of the<br />
institute<br />
No. of Deliveries<br />
2009-10 2010-11 2011-12<br />
SDH Aheri 279 247 341<br />
RH Sironcha 82 <strong>13</strong>6 142<br />
1 Gadchiroli RH Bhamaragad 26 18 31<br />
RH Dhanora 95 106 116<br />
RH Etapalli 10 38 81<br />
2 Amravati SDH Dharni 483 487 532<br />
Page | 19
Sr. No.<br />
Name of the<br />
District<br />
3 Nandurbar<br />
Name of the<br />
institute<br />
Budget required for special focus Hospitals<br />
No. of Deliveries<br />
2009-10 2010-11 2011-12<br />
RH Chikhaldara 61 38 46<br />
RH Churni 104 78 48<br />
RH Akkalkuwa 199 185 203<br />
RH Dhadgaon 594 798 845<br />
RH Molgi 122 190 190<br />
Total 11 hospitals have been included as special focus hospitals in the state. These are very<br />
remote hospitals, without availability of specialists, far away from District Hospitals and with<br />
very high IMR and MMR.<br />
Salary of human resource to these hospitals was requested under RCH Flexi pool and repairs<br />
and main building and quarters requested under Mission Flexi pool. GOI has approved salary of<br />
Specialist Rs. 369.6 Crores for the specialists.<br />
These are very small places without any staying arrangement in the village or city. Therefore<br />
package declared to these doctors include rent free quarters. Considering this, plan is<br />
submitted to establish laboratories, repair OT, labour room BSU and repairs of quarters.<br />
Table above clearly show that these hospitals are well utilized. If additional inputs are given<br />
then cesarean section and other important services can also be started in these hospitals.<br />
As per discussion on 6-8 June <strong>2012</strong>, budget requirement is recalculated. Duplication of budget<br />
requested for Blood Bank / Blood Storage Unit is deducted and budget completely revised.<br />
Hospital wise budget requirement for construction work is as follows:<br />
Sr District<br />
Table – Hospital wise requirement of budget for special focus hospitals<br />
Rs. In Lakhs<br />
Name of the<br />
hospital<br />
Laboratory<br />
and blood<br />
bank<br />
equipment<br />
Repairs and new<br />
construction<br />
Main<br />
building<br />
Quarters<br />
Total<br />
1 Gadchiroli SDH Aheri 0 11 45 56<br />
RH Sironcha 9.4 22.5 111 142.9<br />
RH Bhamragad 8.4 19.3 74 101.7<br />
RH Dhanora 6.2 17.8 88 112<br />
RH Etapalli 5 21 63 89<br />
Page | 20
Sr District<br />
Name of the<br />
hospital<br />
Laboratory<br />
and blood<br />
bank<br />
equipment<br />
Repairs and new<br />
construction<br />
Main<br />
building<br />
Quarters<br />
Total<br />
2 Amarawati SDH Dharani 0 16.8 1<strong>13</strong> 129.8<br />
RH Chikhaldara 3.7 9.5 34 47.2<br />
RH Churni 3.7 7 106 116.7<br />
3 Nandurbar RH Akkalkuwa 8.4 23 147 178.4<br />
RH Dhadgaon 8.5 19.5 123 151<br />
RH Molgi 3.7 14.1 54 71.8<br />
Total 57 181.5 958 1196.5<br />
Considering the clarification given above, GoI is requested to reconsider its decision and<br />
approve this activity. Rs. 1196.5 may be approved for strengthening of 11 special focus<br />
hospitals in the state.<br />
SUBSECTION - B.4.1.3 : ESTABLISHMENT OF SNCU<br />
Remarks of ROP : Approval pended. State to submit equipment audit of existing equipment and<br />
resubmit the plan as per gap analysis.<br />
Maharashtra State is establishing SNCU as per IPHS at 34 Hospitals in these States. GoI in its<br />
guidelines for establishment of SNCU has identified equipment, instrument and support<br />
services for these SNCU.<br />
Presently NICU is functional at small scale all these places and establishment of full-fledged<br />
SNCU is in progress. Beds of SNCU are based on number of deliveries criteria provided in SNCU<br />
guidelines. These beds have increased from 198 beds to 557 beds. Instrument and Equipment<br />
required for each of SNCU as per IPHS norms published by GoI are identified, presently<br />
available instrument and equipment were deducted from this and finally only gap is being<br />
proposed for procurement. Total 32 types of equipment are required for SNCU. No. of<br />
equipment are 5238. Out of these 1001 equipment are already available and 4237 equipment<br />
need to be purchased.<br />
As per discussion with Child Health Division, detailed equipment wise requirement as per<br />
norms, current availability and actual requirement is calculated for each equipment in table<br />
below. SNCU wise list of equipment availability and requirement is submitted as Annex – B.4.5.<br />
Sr.<br />
No<br />
Table – Requirement of equipment for SNCU in Maharashtra<br />
Name of Equipment<br />
No.<br />
Required<br />
as per<br />
norm<br />
No.<br />
Available<br />
No. to<br />
be<br />
Procured<br />
Unit<br />
Price (in<br />
Lakh)<br />
Rs. In Lakhs<br />
Total<br />
Cost (In<br />
Lakh)<br />
Page | 21
Sr.<br />
No<br />
Name of Equipment<br />
A Major Equipment<br />
No.<br />
Required<br />
as per<br />
norm<br />
No.<br />
Available<br />
No. to<br />
be<br />
Procured<br />
Unit<br />
Price (in<br />
Lakh)<br />
Total<br />
Cost (In<br />
Lakh)<br />
1 Infant Warmer 742 200 542 0.53 289.75<br />
2 Phototherapy Unit 271 101 170 0.47 80.33<br />
3 Pulse Oxyimeter 271 29 242 0.79 191.79<br />
4 Syringe Pump <strong>13</strong>8 28 110 0.36 39.38<br />
5 Monitor 42 0 42 1.20 50.40<br />
Total<br />
Small<br />
1464 358 1106 3.36 651.64<br />
B Instrument/Equipment<br />
1 Laryngoscope Set 271 54 217 0.02 3.80<br />
2 Manual resuscitator 94 43 51 0.03 1.53<br />
3 Pump,Suction,Portable 94 37 57 0.03 1.43<br />
4 Pump,Suction,foot operated 94 32 62 0.04 2.28<br />
5 Suture instruments 94 22 72 0.02 1.08<br />
6 Oxygen Hood 271 60 211 0.10 21.53<br />
7 Thermometer Clinical, digital 536 77 459 0.00 1.42<br />
8 Scale baby electronic 188 27 161 0.05 8.05<br />
9 Stethoscope Neonate 536 51 485 0.00 0.81<br />
10<br />
Sphygmomanometer,<br />
electronic<br />
271 5 266 0.03 6.65<br />
11 Light, Examination 271 18 253 0.01 2.53<br />
12 Hub Cutter syringe 94 31 63 0.02 1.23<br />
<strong>13</strong> Basin Kidney 188 39 149 0.00 0.10<br />
14 Tray dressing 188 54 <strong>13</strong>4 0.00 0.07<br />
15 Stand Infusion 46 19 27 0.01 0.26<br />
16 Infantometer 46 5 41 0.02 0.62<br />
17 Autoclave, Steam 46 4 42 0.08 3.25<br />
18 Laundry Washer dryer 46 1 45 0.12 5.40<br />
19 Centrifuge 46 0 46 0.19 8.74<br />
20 Glucometer <strong>13</strong>6 45 91 0.01 0.68<br />
21 Split AC 46 1 45 0.30 <strong>13</strong>.50<br />
22 Refrigerator 110 Lit. 46 6 40 0.10 4.00<br />
23 Voltage Stabilizer (25-50 K.V.) 46 6 40 0.25 10.00<br />
24 Computer With Printer 46 6 40 0.48 19.26<br />
Page | 22
Sr.<br />
No<br />
Name of Equipment<br />
No.<br />
Required<br />
as per<br />
norm<br />
No.<br />
Available<br />
No. to<br />
be<br />
Procured<br />
Unit<br />
Price (in<br />
Lakh)<br />
Total<br />
Cost (In<br />
Lakh)<br />
25 Generator 25-50 KV 34 0 34 3.04 103.43<br />
Total 3774 643 3<strong>13</strong>1 4.93 221.66<br />
Grant Total A + B 5238 1001 4237 8.29 873.30<br />
Considering the services above and guidelines of GoI for SNCU establishment and functioning,<br />
budget required for SNCU under MFP is as follows:<br />
Sir Type of institute<br />
Table – Budget required for SNCU<br />
Average<br />
cost per<br />
SNCU<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Total<br />
cost<br />
1 Larger equipment as per GoI list 19.2 34 651.64<br />
2<br />
Minor equipment and instrument as per GoI<br />
List<br />
6.5 34 221.66<br />
3 Maintenance of Equipment 3 34 102<br />
4 Cleaning services 2.37 34 80.64<br />
5 Security Services 1.78 34 60.48<br />
6 Laundry Services 0.4 34 <strong>13</strong>.6<br />
7 Contingency 1.2 34 40.8<br />
Total 1170.82<br />
Considering the explanation submitted above, budget of Rs. 1170.82 Lakh is requested for<br />
approval.<br />
B.4.2 : STRENGTHENING OF DISTRICT, SUB-DISTRICT HOSPITALS, CHCs, PHCS.<br />
Budget not requested.<br />
SUBSECTION - B.4.2.1 : UN-INTERRUPTED POWER SUPPLY TO FACILITIES<br />
Un-interrupted power supply to <strong>health</strong> facilities (Solar Photovoltaic System) is requested at<br />
B.4.2.1 for non-tribal and also at B.24.6 for tribal hospitals. GoI has approved this activity for<br />
non-tribal areas (Rs. 660.0 Lakh) and not approved for tribal hospitals (Rs. 512.02 Lakh0. As per<br />
discussion during 6-8 June Meeting at Delhi, the activity of Supply of Solar Photovoltaic System<br />
to Tribal Hospitals (B.24.6) is now shifted to Section B.4.2.1. In addition to this, in activity for<br />
budget required for monitoring cell of Photovoltaic system (A.8.1.9), there is remark that this<br />
may be requested from MFP. Accordingly, this budget is also requested from MFP. This may be<br />
approved as follows:<br />
Page | 23
B.4.2.1 A : Uninterrupted power supply to Solar Health Facilities – Non tribal areas<br />
Budget requested : Rs. 660.0 Lakh. Budget Approved : Rs. 660.0 Lakh. Accepted.<br />
B.4.2.1 B : Uninterrupted power supply to Solar Health Facilities – Tribal Hospitals (CHCs/SDH)<br />
There is severe electricity problem in state. IPHS <strong>health</strong> institutions require continuous power<br />
supply. Therefore solar backup system is proposed for selected IPHS Hospitals (CHCs/SDH) in<br />
tribal areas. Hospital will be selected on the basis of performance of hospitals in indicators such<br />
as Delivery, IPD, OPD and Cesarean Sections performed during 2011-12.<br />
Special system has been developed in the state with the help of Government College of<br />
Engineering Pune for <strong>health</strong> facilities. This system can provide power to all the equipment in<br />
PHC for 24 hours.<br />
Same system will be used for tribal areas. This year, it is proposed to try solar back up system<br />
for selected Rural Hospitals. Budget required for this system is as follows:<br />
Compliance of remarks<br />
All the PHCs in tribal areas are covered now so there is no need of grants for tribal PHCs.<br />
However, this year, grant is requested for hospitals which fulfill criteria of delivery point.<br />
Budget required for solar power backup<br />
Budget required for solar power backup is mentioned below:<br />
Table – :Budget required for solar power backup in tribal area hospitals<br />
Rs. In Lakhs<br />
Sir Type of institute Cost per unit No. of units Total cost<br />
1 Solar Backup – RH 32 16 192<br />
Total<br />
192<br />
Considering the importance of un-interrupted power supply, it is proposed to add new <strong>health</strong><br />
institutes for solar power if there is saving in other activities.<br />
B.4.2.1 C : Solar back up monitoring Cell<br />
So far, solar back up is provided to 330 PHCs and 5 Hospitals since last three years. All these<br />
systems are provided with simcards which daily send message about condition of the solar<br />
system. Information of all the centers is collected at one place in Mumbai, daily it is analyzed<br />
and the message is given to the Supplier for systems under warranty and Maintenance Agency<br />
for the systems which are now under maintenance contract. Daily 6-7 messages are received.<br />
These messages are communicated to concerned agency and also follow up is made for timely<br />
repairs.<br />
Page | 24
Same cell is also has responsibility of getting demands from District Societies, corrections in any<br />
required, floating tender, analyzing the tender, getting sanctions and assisting the Procurement<br />
Department to issue the orders. Solar cell also monitors the establishment of Solar system in<br />
selected <strong>health</strong> facility.<br />
Solar cell is established in 2009-10 and is functional currently at SHS Mumbai.<br />
Budget required for solar cell is as follows:<br />
Table – Budget required for Solar Back UP monitoring Cell<br />
Rs. In Lakhs<br />
Sir Type of institute Cost per unit No. of units Total cost<br />
1<br />
Salary of Program Officer for<br />
Support<br />
2.88 1 2.88<br />
2 Salary of DEO for support 1.2 1 1.2<br />
Total<br />
4.08<br />
SUBSECTION - B.4.2.2 : QUALITY ASSURANCE IN IPHS FACILITIES<br />
The activity of Quality Assurance was mentioned in PIP guidelines of GoI in 2010-11. That time<br />
this activity was submitted and got approval also. However, activity could not be implemented<br />
as Technical Support Partners could not be appointed. Therefore this was again requested in<br />
PIP of 2011-12 and again got approval. It took long time to clear the pre-conditions and NGOs<br />
selected so the activity started in October 2011. Now MoU is made with four Technical Support<br />
Partners and NHSRC and this is fourth month they have started work.<br />
Work of Quality Assurance is being carried out in stages as per guidelines issued by NHSRC in<br />
2011. NHSRC has also given guidelines for percentage of payment at each stage as mentioned<br />
in table below:<br />
Table – Guidelines of NHSRC for payment of Technical Support partners<br />
Sr Stage Description % of Payment to be<br />
made<br />
1 I Sub<strong>mission</strong> of 15 copies of “As is report” with gaps 15%<br />
2 II Preparation and distribution of training and process<br />
manual to all the concerned staff of hospital<br />
15%<br />
3 III Implementation of all quality system documents 30%<br />
4 IV Pre-certification audit and closure of all nonconformities<br />
20%<br />
5 V Completion of final audit 20%<br />
Total 100%<br />
Page | 25
Presently all the TSPs have completed first stage and they are in the second stage. Therefore, if<br />
to be discontinued, they have to be paid payment up to second stage.<br />
Payment of the Technical Support Partners as per NHSRC guidelines and MOU will be as per<br />
table submitted below:<br />
Sr. No. Name of TSP<br />
Table – Budget need to be distributed to TSP<br />
1 st installment<br />
15%<br />
2 nd<br />
installment<br />
15%<br />
Training<br />
expenses<br />
Rs. In Lakhs<br />
Total<br />
1 HOSMAC 70.968 70.968 8.4 150.336<br />
2 ACME 38.8245 38.8245 6.9 84.549<br />
3<br />
MEDICA<br />
SYNERGIE<br />
34.7235 34.7235 6.68 76.127<br />
4 OCTAVO 61.5255 61.5255 7.6 <strong>13</strong>0.651<br />
Total 206.0415 206.0415 29.59 441.663<br />
The reports prepared by TSPs will be utilized for further improvement in quality services.<br />
Remaining part of ISO certification will be carried out under IPHS Up gradation.<br />
SCHEME - B.4.2.3 : BARRIER FREE ENVIRONMENT IN HOSPITALS<br />
GoI has not approved this activity. It is proposed to drop this activity as per remarks of GOI.<br />
SUBSECTION - B.4.4 : LOGISTICS MANAGEMENT AND IMPROVEMENT<br />
SCHEME - B.4.4.1 : MOBILITY SUPPORT<br />
As per remarks of ROP, this activity is submitted a comprehensive plan in Chapter B.12 :<br />
Referral Transport.<br />
Page | 26
SCHEME - B.4.4.2 : EQUIPMENT MAINTENANCE AND REPAIRS<br />
Mobility support for HEMR unit is shifted to Mobility Support under NRHM. GoI has rejected<br />
appointment of technical consultants for repairs of instrument and equipment. This decision is<br />
accepted. No additional budget requested under this head.<br />
SCHEME - B.4.4.3 : DISABILITY WORKSHOPS AT DISTRICT HOSPITALS<br />
Approved activity<br />
SCHEME - B.4.4.4 : MODERNIZATION OF HOSPITAL KITCHEN<br />
Approved activity<br />
SCHEME - B.4.4.5 : PUBLIC HEALTH ESTATE MANAGEMENT CELL<br />
Need of Public Health Estate Management Cell<br />
Most of the <strong>health</strong> facilities in Maharashtra are constructed on land either donated by donor or<br />
on government land.<br />
There is need to update the record of land of <strong>health</strong> facilities in the state for following<br />
reasons<br />
• Infrastructure development<br />
• To make availability of land for constructions of the new <strong>health</strong> facility.<br />
• To remove the encroachment on <strong>health</strong> facility.<br />
• To update the records of land of <strong>health</strong> facility.<br />
Many of these lands are not in the name of <strong>health</strong> department. In some facility the<br />
boundaries are not cleared.<br />
Considering the above fact, Public Health Estate Management Cell is established in state<br />
Health society & at regional places in the Deputy Director Health office during 2011-12. The<br />
State Health Society, Maharashtra Mumbai have already established four Public Health Estate<br />
Management Cell in the state & remaining five will be established till March <strong>2012</strong>.<br />
Present position of PHEMS<br />
PHEMS was approved in 2011-12. Advertisement was given for filling up of posts in July 2011.<br />
Cell started functioning from September 2011. Position of filling up of posts in the state as on<br />
1.4.<strong>2012</strong> is as follows:<br />
Page | 27
Table – Position of posts filled in as on 1.4.<strong>2012</strong><br />
Sr. No. Designation No. of posts<br />
No. in position<br />
on 1.4.2011<br />
1 Senior Estate Manager 8 5<br />
2 Junior Estate Manager 9 8<br />
3 Program Officer at state level 1 1<br />
4 Program Assistant 9 9<br />
5 Travel & Mobility 9 9<br />
6 Office Contingency 9 9<br />
7 Office equipment& Furniture 9 9<br />
Total<br />
All these officers have started working and have collected valuable records for <strong>health</strong><br />
department. Total performance of this cell in year 2011-12 (7 months) is mentioned in table<br />
below:<br />
Table - Performance of Public Health Estate Management Cell (September 2011 to<br />
March<strong>2012</strong>)<br />
Sir Name of the<br />
circle<br />
No of<br />
<strong>health</strong><br />
institutes<br />
visited<br />
Record<br />
Updated<br />
Encroach<br />
ment<br />
Removed<br />
Land made<br />
available for<br />
construction<br />
1. Pune 194 451 0 0<br />
2. Aurangabad 206/65LL 87/61L 2<br />
3. Nagpur 275 122 0 0<br />
4. Latur 311 168 0 01<br />
If this cell continues then it can work more efficiently this year. It is expected that this cell will<br />
be able to get records of all existing <strong>health</strong> facilities. Considering the load, it is proposed to<br />
continue this activity for next three years.<br />
Page | 28<br />
7
Considering the remarks of RoP, budget is requested only for existing staff. Therefore it is<br />
requested to sanction the budget as proposed.<br />
Sr.<br />
No.<br />
Table : Budget required for Estate Management Cell during <strong>2012</strong>-<strong>13</strong><br />
(Rs. In Lakhs)<br />
Designation<br />
No. of<br />
posts<br />
No. in<br />
position on<br />
1.4.2011<br />
Budget<br />
per post<br />
Budget<br />
required<br />
1 Senior Estate Manager 8 5 3.6 18<br />
2 Junior Estate Manager 9 8 2.4 19.2<br />
3<br />
Program Officer at state<br />
level<br />
1 1 3 3<br />
4 Program Assistant 9 9 1.2 10.8<br />
5 Travel & Mobility 9 9 5 45<br />
6 Office Contingency 9 9 0.6 5.4<br />
7 Office equipment& Furniture 9 9 0.5 4.5<br />
Total 16.3 105.9<br />
It is requested that this activity may be approved and budget of Rs. 105.9 Lakh may be<br />
sanctioned.<br />
SCHEME - B.4.4.6 : IPHS MONITORING WING<br />
There are many aspects which need to be monitored closely for upgrading the hospitals and also for<br />
providing quality services. All these things should be done as per findings of External Facility survey.<br />
Thus there is need of closely monitoring structure for timely upgrading of hospitals.<br />
Out of the total budget requested under Mission Flexi pool, more than 20% budget is requested for<br />
IPHS. Thus this is extremely important program as mother and child services will not be accepted by<br />
community unless the <strong>health</strong> facility is in good condition. Considering the importance of program and<br />
need to closely monitor this, IPHS monitoring system is established at district, divisional and state level.<br />
IPHS monitoring system at district level is mentioned in IPHS chapter. In this section, IPHS monitoring<br />
system at state and district level is mentioned. These units have been established in 2009-10 and have<br />
been proved to be very useful.<br />
Responsibilities of IPHS Wing at District level is as follows:<br />
• Screening the data of <strong>health</strong> facilities for inclusion of facility in IPHS. Recommending names of<br />
facilities with data support.<br />
• Support to MO PHC / Medical Superintendent in planning <strong>health</strong> facility up gradation. Filling up<br />
of gap formats and editing the formats.<br />
Page | 29
• Monitoring for filling up of identified gaps. One separate file is maintained for each <strong>health</strong><br />
facility in district and gap filling is monitored on monthly basis.<br />
• Supporting district for procurement of medical equipment, maintenance of medical equipment<br />
and decision about out of order equipment.<br />
• Monitoring the functional status of medical equipment in the IPHS facilities of the district.<br />
Coordination with Health Equipment Unit for scheduling the visit of HEMR Units and informing<br />
this to MO PHC.<br />
• Monitoring mobility support to PHCs and Hospitals. Providing mobility support budget to <strong>health</strong><br />
facility. Monitoring referral transport under JSSK.<br />
• Monitoring support services such as electricity either through express feeder or through Solar<br />
Photovoltaic system.<br />
IPHS Coordinator is only Biomedical Engineer available at District level in Public Health Department.<br />
He/she is posted at CS office so she can discharge above mentioned duties appropriately.<br />
Therefore same is to be continued for next year.<br />
Considering the comments on IPHS wing, post of Consultant – IPHS is discontinued. Mobility support<br />
required for IPHS Consultant and contingency is also discontinued. At district level, post of DEO and<br />
Statistical Investigator is also discontinued. Therefore out of 5 posts, only one post is continued for year<br />
<strong>2012</strong>-<strong>13</strong>.<br />
As per discussion with Maternal Health Division during 6-8 June <strong>2012</strong> meeting, Consultants under RCH<br />
Office will be included in the Cell for monitoring of quality improvement in the services offered by<br />
Health Facilities. No new staff is recommended but staff appointed for Quality Assurance will be reoriented<br />
for this activity and both the cells will work in close liaison.<br />
Present position of the staff<br />
IPHS Wing is in position since 2009-10. No. of staff approved for this wing since last three years is 92<br />
persons as mentioned in second column of table below. Out of these, 87 persons were working in the<br />
cell on 31.3.<strong>2012</strong>. As per discussion, 45 persons are discontinued or absorbed somewhere else and now<br />
staff of 42 persons is requested under the scheme. Staff retained is experienced and is supporting the<br />
<strong>health</strong> system for implementation of this program. Request for staff to be continued in <strong>2012</strong>-<strong>13</strong> is as<br />
follows:<br />
Sr Name of post<br />
Table – Proposed IPHS Staff as on 31.3.<strong>2012</strong><br />
No.<br />
approved<br />
No. in<br />
position on<br />
31.3.<strong>2012</strong><br />
No<br />
proposed<br />
in <strong>2012</strong>-<br />
<strong>13</strong><br />
1 IPHS Coordinator at district level 33 33 33<br />
2 IPHS Consultant at Circle level 9 8<br />
0<br />
3 State Senior IPHS Consultant 1 1 1<br />
4 Data Entry operator at Circle level 8 8<br />
0<br />
Remarks<br />
Post<br />
discontinued<br />
Post<br />
discontinued<br />
Page | 30
5<br />
Data Entry Operator at District<br />
level<br />
33 29<br />
6 IPHS Supervisors at state level 4 4 4<br />
7 Salary of DEO (4) 4 4 4<br />
Total 92 87 42<br />
Considering the above fact, detailed budget requirement is as follows:<br />
Budget requirement<br />
0<br />
Post<br />
discontinued<br />
Total manpower is revised. Initially budget required for State-Circle and District IPHS wings was Rs.<br />
440.88 Lakh. Now it is revised to Rs. 181.65 Lakhs which is 60% reduction.<br />
Budget requirement is as follows:<br />
Table - : Budget requirement for IPHS Wing<br />
Sr Name of post Unit cost<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Total<br />
budget<br />
1 Salary and TA/DA of IPHS Coordinator 3.9 33 128.7<br />
Stationary, internet, office maintenance,<br />
2 photocopying, AMC of office equipment, etc at<br />
District Office)<br />
0.75 33 24.75<br />
3 Salary of State IPHS Consultant 6 1 6<br />
4 Salary of IPHS Supervisors (4) at SHS 3.6 4 14.4<br />
5 Salary of DEO (4) 1.2 4 4.8<br />
6 For civil works, renovation, repairs, furniture 3 1 3<br />
Total 181.65<br />
SECTION - B.5 : NEW CONSTRUCTION, RENOVATION AND SETTING UP OF HEALTH FACILITIES<br />
New construction, repairs of <strong>health</strong> facility infrastructure in Maharashtra is carried out by two<br />
agencies. Infrastructure Development Wing is established to carry out construction work of<br />
buildings of PHC/PHU and Sub-Centers. Contractual Junior Engineer, Deputy Engineer and<br />
Executive Engineers are appointed in this wing. This wing is headed by Superintending Engineer<br />
who is regular SE from PWD. In addition to this, Executive Engineers of PWD also supervise the<br />
work of IDW engineers wherever necessary.<br />
No additional charges are levied on the works done by IDW wing.<br />
Page | 31
New construction of Hospitals, Nursing Schools and Regional Warehouses is carried out by<br />
Public Works Department of Government of Maharashtra. PWD claims 5% Centage charges for<br />
all works done and it is included in estimate provided by PWD.<br />
Both the wings – IDW and PWD use DSR for making estimates.<br />
For specified works such as construction of SNCU or construction of Audiometry Room, PWD<br />
hires special architect for planning. Architect is selected from approved panel of PWD and<br />
payment to architect is made as per approved government rates. Fees of architect are included<br />
in estimate provided by PWD.<br />
Considering the volume of work being done in Health Department and time bound program of<br />
NRHM funds, PWD has appointed Chief Engineer Aurangabad as Nodal Officer for Health<br />
Department works. Positive difference with PWD is observed after appointment of Nodal<br />
officer.<br />
One new software ‘Construction Tracker’ is introduced in Maharashtra state for all <strong>health</strong><br />
department constructions. The work is registered in the system immediately after awarding<br />
administrative approval. Work is tracked till possession. It is proving very useful to the state for<br />
timely completion of construction.<br />
SUBSECTION - B.5.1 TO B.5.3 : NEW CONSTRUCTION AND RENOVATION OF SUB-CENTERS,<br />
PHCs AND CHCs<br />
A) Spill Works:-<br />
Spill works are those works which started before 31.3.<strong>2012</strong> i.e. last year and could not be<br />
completed in same financial year. Precaution is taken to not to start new work in last three<br />
months of the year so that spill cost remains within the limits. This year due to water scarcity,<br />
civil works could not be completed within given time in some areas of the state. This has<br />
increased the spill cost.<br />
There are 190 Spill works pertaining to Repairs Works (Spill Cost Rs. 458.79 Lakhs) and 161 spill<br />
works pertaining to New Construction (Spill Cost Rs. 3154.56 Lakhs). The total spill cost comes<br />
out to be 36<strong>13</strong>.35 Lakhs. All these works are sanctioned works of last year.<br />
Budget required for spill works as per type of facility is submitted in table below:<br />
Table-(A) – Budget required for spill works<br />
Sr. No. Type of work Facility No. of works<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
1 Repair works Sub-Centre 87 <strong>13</strong>5.32<br />
Page | 32
Sr. No. Type of work Facility No. of works<br />
Budget<br />
required<br />
PHC 103 323.47<br />
RH/SDH 0 0.00<br />
DH 0 0.00<br />
Total 190 458.79<br />
2 New Works Sub-Centre 122 1153.46<br />
PHC 39 2001.10<br />
RH/SDH 0 0.00<br />
DH 0 0.00<br />
Total 161 3154.56<br />
Grand total All facilities 351 36<strong>13</strong>.35<br />
As these works are ongoing works and this is a committed expenditure, this may be approved.<br />
List of works is attached as Annex B.5.1<br />
B) New Construction works Proposed in <strong>2012</strong>-<strong>13</strong>:-<br />
1. PHCs:- New construction of PHCs 10 No’s and Quarters at 31 PHCs are proposed, (<br />
Amounting to Rs. 1475.00 Lakhs )<br />
GOI Remarks:- Approval pended. Need to submit fresh plan. Approval will be<br />
given on the basis of performance e.g. Delivery points.<br />
Justification for Approval:- Fresh plan is submitted now on the basis of<br />
performance e.g. Delivery points. Hence the activity may be approved.<br />
2. SHCs:- New construction of 25 SHCs are proposed, ( Amounting to Rs. 450.00 Lakhs )<br />
GOI Remarks:- Approval pended. State to provide break up on the ones existing<br />
in rented buildings and the ones that are completely new constructions. If<br />
existing in rented building state to provide details of functionality such as<br />
delivery load, OPD/IPD and bed occupancy rate.<br />
Justification for Approval:- Building status for all the works is mentioned now (<br />
i.e. Whether the institute is working in rented building or a new<br />
construction.) All the relevant information about rented<br />
building is also given. Hence may be approved.<br />
Table-(B) – Budget required for New works<br />
Rs. In Lakhs<br />
Page | 33
Sr. No. Type of work Facility<br />
No. of<br />
works<br />
Unit Cost Budget required<br />
1 New Construction Sub-Centre 25 18.00 450.00<br />
PHC+<br />
Quarters<br />
41(10+31)<br />
New<br />
construction 10<br />
PHCs @ 72 L<br />
(31 Qtrs.)<br />
1475.00<br />
RH/SDH(CHC) 0 0.00 0.00<br />
DH 0 0.00 0.00<br />
Total 66 1925.00<br />
The list of the facilities proposed for new construction is submitted as Annex – B.5. – II<br />
Table-(C) – Budget Approved for Upgradation works<br />
Rs. In Lakhs<br />
Activity<br />
proposed<br />
Unit cost<br />
(in lakhs)<br />
Physical<br />
Target<br />
Amount<br />
Proposed<br />
(in lakhs)<br />
Amount<br />
Approved<br />
(in lakhs)<br />
Remarks<br />
Repairs/ Upgradations<br />
DH<br />
11 325.00 325.00 Approved as per<br />
SDH<br />
CHC<br />
PHC<br />
SHC<br />
15<br />
57<br />
304<br />
475<br />
204.00<br />
658.25<br />
1997.66<br />
1284.14<br />
204.00<br />
658.25<br />
1997.66<br />
1284.14<br />
list provided by<br />
State. State to<br />
ensure that work<br />
will be completed<br />
this year and no<br />
further grants<br />
Total<br />
862 4469.05 4469.05<br />
will be given<br />
from new year<br />
for these facilities<br />
Table– Total Summary (For A)Spill Work, B) New Construction, C) Repairs/Upgradation)<br />
Rs. In Lakhs<br />
Activity proposed<br />
Physical<br />
Target<br />
Amount<br />
Approved<br />
(in lakhs)<br />
Amount<br />
Proposed<br />
(in lakhs)<br />
A)Spill works 351 0.00 36<strong>13</strong>.35<br />
B)New Construction 66 0.00 1925.00<br />
C)Repairs/ Upgradations 862 4469.05 4469.05<br />
Total 1279 4469.05 10007.40<br />
Remarks<br />
Requested in<br />
revised PIP<br />
Requested in<br />
revised PIP<br />
Already<br />
approved<br />
Page | 34
From Proposed total PIP of Rs. 10007.40 Lakhs only repairs/ upgradation works amounting<br />
Rs. 4469.05 Lakhs is approved. Spill works and New Construction works of Rs. 5538.35 Lakhs<br />
are proposed for approval of GOI.<br />
The list of the facilities proposed for new construction is submitted as Annex – B.5. – II<br />
SUB-SECTION - B.5.4 : SETTING UP OF INFRASTRUCTURE DEVELOPMENT WING<br />
As per remarks, shifted to Program Management Section and approved.<br />
SUBSECTION - B.5.5 : GOVERNMENT DISPENSARIES AND OTHER RENOVATIONS<br />
No budget requested<br />
SUBSECTION - B.5.6 : CONSTRUCTION OF BLOCK HEALTH OFFICE<br />
Maharashtra had requested budget for three activities. These are Repairs of BPMU/DPMU, new<br />
construction of BPMU / DPMU in non-tribal areas and new construction of BPMU/DPMU in<br />
tribal areas. This proposal is revised. New construction of Block Office in tribal areas only is<br />
requested and repairs of BPMU in tribal and non tribal areas is requested in this chapter. It was<br />
also discussed to support construction of DPMU at 10 places in the state where there is no<br />
space for Civil Surgeon to sit as the District Hospital is handed over to Medical Colleges. This<br />
activity is shifted to B.5.12 : Strengthening of Program Management Unit.<br />
As per discussion, proposal for quarters to BPMU staff is also dropped.<br />
Budget required for strengthening of BPMU is as submitted below:<br />
Budget requirement<br />
Budget required for this activity is as follows:<br />
Table – Budget requirement for Civil Works in BPMU<br />
Sir Particulars Unit cost No. of block<br />
1<br />
Repairs of BPMU in tribal and non –<br />
tribal areas. (Cost mentioned in average<br />
of total demand + Spills of one BPMU in<br />
Nagar Dist)<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
12.4 14 173.6<br />
Page | 35
2<br />
New Construction of BPMU in tribal and<br />
LEA areas<br />
28 6 168<br />
Total 341.6<br />
SUBSECTION - B.5.7 : MAJOR CIVIL WORKS FOR OPERATIONALIZATION OF FRU<br />
State government has established Women Hospitals at Gadchiroli and Nanded. Gadchiroli is<br />
being constructed completely newly whereas, in Nanded, district administration has given one<br />
hospital constructed for Guruta gaddhi (religious ceremony) organized last year in Nanded.<br />
Both these hospitals are planned to be operationalized as FRU as large number of deliveries are<br />
expected at both these places.<br />
Approval for Gadchiroli is already received and Rs. 2.2 Crores handed over to PWD Maharashtra<br />
from NRHM grants. Remaining grants need to be released this year. Gynaec ward of Gadchiroli<br />
is always overcrowded and requires floor beds. Current rate of 300 deliveries per month at<br />
Gadchiroli is expected to increase by 50%. We are expecting about 450-500 deliveries per<br />
month in WH Gadchiroli once it is established. The district administration has allotted central<br />
space to this hospital. Total estimate of the WH Gadchiroli is Rs. <strong>13</strong>.2 crores. Currently we have<br />
released Rs. 2.2 Crores. Out of reaming 11 Crores, Rs. 5.0 Crores will be required during this<br />
year. Establishment of Women Hospital in Gadchiroli will improve the service availability.<br />
Similarly, State Government has established Women Hospital at Nanded. Currently, deliveries<br />
are taking place @ 600-700 PM in Government Medical College Nanded. However, the college<br />
is being shifted to Vishnupuri which is around 12 KM from city. This will increase the load of the<br />
Women Hospital by many fold. It is expected that about 600 deliveries will take place per<br />
month in Women Hospital Nanded. It is proposed to repair the existing WH building, establish<br />
the SNCU, and repair the labour rooms and Operation theaters.<br />
Budget required for these activities is as follows:<br />
Table – Budget required for WH Nanded and WH Gadchiroli to establish as FRU.<br />
Rs. In Lakhs<br />
Sir Activity Unit cost<br />
No. of<br />
units<br />
Budget<br />
requirement<br />
1 WH Gadchiroli<br />
i<br />
Second installment<br />
construction of WH<br />
to PWD for<br />
500 1 500<br />
2 WH Nanded<br />
i Repairs of main building, provision of lift 37 1 37<br />
ii Extension of wards (2 wards of 30 beds) 58 1 58<br />
Page | 36
Sir Activity Unit cost<br />
No. of<br />
units<br />
Budget<br />
requirement<br />
iii Repairs of Labour rooms 2.6 2 5.2<br />
iv Repairs of 2 OTs 3.1 2 6.2<br />
v Establishment of SNCU 72 1 72<br />
vi Establishment of Blood Bank 14 1 14<br />
Total of WH 192.4<br />
Grand total 692.4<br />
SUB-SECTION - B.5.8 : MAJOR CIVIL WORKS FOR OPERATIONALIZATION OF 24×7 PHCs<br />
Covered in IPHS Upgradation. Therefore deleted from this activity<br />
SUBSECTION - B.5.9 : CIVIL WORKS TO OPERATIONALIZE INFECTION MANAGEMENT AND<br />
ENVIRONMENT PROTECTION PLAN<br />
Not approved therefore deleted.<br />
SUBSECTION - B.5.10 : STRENGTHENING OF TRAINING INFRASTRUCTURE<br />
Remarks of RoP : Approval Pended. State to submit detailed plan.<br />
Budget is required for maintaining the buildings of training institutes (minor civil works and<br />
furniture), construction or extension of training institutes and for provision of training aid and<br />
equipment.<br />
i) Mainenance of training institutes<br />
Regarding minor civil works and furniture, this grant is utilized for civil maintenance work of<br />
buildings and hostels. This is because, load of training institutes has increased and budget<br />
available through regular resources is not sufficient. For example, during last year, total 16261<br />
persons trained in HTT and 510516 persons trained in DTT. This increases the pressure on<br />
existing system and this requires changes. This budget is utilized on following aspects:<br />
• Repairs or replacement of tables, chairs, boards and other furniture as per need.<br />
• Repair or replacement of beds, mattresses, study tables in hostel and other hostel<br />
furniture<br />
• Plumbing services repairs<br />
Page | 37
• Electrical services repairs, replacement of geezers, water coolers, etc<br />
• Repairs and maintenance of drainage system<br />
For above mentioned activities, first regular budget is used and then NRHM budget is used.<br />
Considering the load of training for year <strong>2012</strong>-<strong>13</strong> and availability of budget from regular budget,<br />
budget for minor civil works is requested as follows:<br />
Table – Budget required for maintenance of training institutes<br />
Sir Activity<br />
Average<br />
Unit cost<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
requirement<br />
i District Training Center 3 33 99<br />
ii Hospital Training Center 2 23 46<br />
iii HFWTCs and PHI 15 8 120<br />
iv BTCs 1 8 8<br />
Total 273<br />
ii) Construction or extension of training institutes<br />
In Maharashtra there are total 33 DTT approved. However, out of these, DTT building is<br />
available in only 30 districts. It is proposed to construct remaining three DTTs at Gondia, Hingoli<br />
and Washim.<br />
Similarly for HTT, currently only 14 HTT have its own building. Remaining HTT does not have<br />
building. Out of these, HTT at Gadchiroli, Beed and Ratnagiri has available space. Therefore HTT<br />
building is requested for these three HTTs.<br />
Considering the load of HFWTC and PHI, it is proposed to expand the training institutes as per<br />
requirement. Current hostel of 3 stories of PHI is proposed to expand by 2 more floors.<br />
Similarly, HFWTCs at Nagpur, Amarawati, Pune and Aurangabad needs extension of hostels.<br />
Budget required for each of these institutes as per block estimates is requested. Nutrition<br />
Training Center is functional in Maharashtra since 1978 in SIHFW campus Nagpur. Considering<br />
the problem of malnutrition, this center is provided with new responsibilities. Budget is also<br />
required for extension of the Nutrition Training Center of Nagpur. For works above 1.0 Crore,<br />
once the administrative approval to design is obtained, drawings will be submitted to GoI.<br />
Facility wise requirement of construction is submitted in table below:<br />
Table – Facility wise requirement of budget for construction<br />
Rs. In Lakhs<br />
Page | 38
Sir Type of institute<br />
Cost per<br />
unit<br />
No. of<br />
units<br />
Total cost<br />
1<br />
District Training Center at Gondia, Hingoli and<br />
Washim<br />
210 3 630<br />
2<br />
Hospital Training Center at Gadchiroli, Beed<br />
and Ratnagiri<br />
195 3 585<br />
3 Remaining construction of HFWTC Kolhapur 100 1 100<br />
4 Remaining construction of HFWTC Thane 175 1 175<br />
5 Extension of Hostel at PHI Nagpur 226 1 226<br />
6 Extension of Hostel at HFWTC, Pune 172 1 172<br />
7 Extension of Nutrition Training Center 98 1 98<br />
Total 1986<br />
Although the budget required for this activity is Rs. 1986 Lakh, budget of Rs. 1029.0 lakh will be<br />
required this year for construction as proposed in PIP. Remaining budget will be requested in<br />
year 20<strong>13</strong>-14.<br />
iii) Provision of required training aid and equipment<br />
All the training centers now a day require LCD Projector, IDP, Lap top and other training aid.<br />
Training center wise requirement of training aid is as follows:<br />
Sir Activity<br />
Table – Provision of Training Aid and equipment<br />
Average<br />
Unit cost<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
requirement<br />
1 District Training Center 1 33 33<br />
2 Hospital Training Center 0.5 23 11.5<br />
3 HFWTCs and PHI 3 8 24<br />
5 BTCs 0.5 7 3.5<br />
6<br />
Library for training institutes and data<br />
management center<br />
2 8 16<br />
Grand Total 88<br />
As mentioned in the remarks, detailed plan is submitted. It is requested to approve the<br />
proposal.<br />
iv) New Construction of Colde Chain Equipment Training Center at Pune.<br />
Page | 39
Immunisation division, MoHFW has proposed to establish a National Cold Chain, Vaccine,<br />
Logistics Management Resource Center at New Delhi. Present training Center of Government of<br />
Maharashtra for Cold Cjhain Equipment will be designated as Cold Chain Equipment Training<br />
Center. Government of India MOHFW by letter No. M – 11014/1/2010-CC&V dated 27.7.2011<br />
directed to Director, NIHFW New Delhi to establish CCE Training Center thorugh PIP of<br />
Maharashtra. UNICEF is providing technical support to the project. Formal MOU is signed<br />
between GoI and GoM for this institute.<br />
As per the discussion of State Health Transport Organisation and Immunization Divion of GoI,<br />
the budget for traning center will be as follows:<br />
Table – Budget required for establishment of CCE Training Center Pune.<br />
Rs. In Lakhs<br />
Sr Name of the Subject Approximate Cost<br />
A Non-recurring cost<br />
1<br />
Complete renovation work and infrastructure strengthning of<br />
existing training center building. 90<br />
2 Construction of new hostel building in SHTOcampus 1000<br />
3 Vehicle provision 30<br />
Total Non-recurring 1120<br />
B Recurring cost<br />
1 Staf salary 95<br />
2 Operational expenses 105<br />
Total - Recurring 200<br />
Grand total <strong>13</strong>20<br />
Out of above mentioned activities, only non-recurring activity will start this year, and for this,<br />
SHTO Pune has requestd Rs. 300.0 Lakh budget for year <strong>2012</strong>-<strong>13</strong>.<br />
SUBSECTION B.5.11: CONSTRUCTION AUDIT<br />
Remarks of ROP : Not approved<br />
In NRHM, execution of civil works pertaining to state sector Buildings (i.e. District<br />
Hospitals, Sub District Hospitals and CHCs) is done by State PWD and execution of works<br />
pertaining to Zilla Parishad sector i.e. PHCs and SCs is done by Infrastructure Development Wing<br />
(IDW) established in every district. As far as State PWD is concerned there is a separate wing<br />
called “Vigilance and Quality Control Wing” for monitoring the quality of works being executed<br />
by PWD. But for the works executed by IDW there is no independent quality assurance wing.<br />
Page | 40
Hence it is decided to get the quality control work (pertaining to IDW works) done by<br />
appointing a separate agency at State level for “Third party evaluation.” The State Executive<br />
Committee also sanctioned the proposal for appointing a separate agency for third party<br />
evaluation in the E.C. meeting held on 22-12-2011.<br />
The scope of the work for “Third Party Evaluation” is decided on the basis of system existing in<br />
“Sarva Shiksha Abhiyan” in Education Department and it is as below :<br />
1. The consultant / representative (Engineer) shall visit each site of work for minimum<br />
four times during the construction of work. These visits shall be when the construction work is<br />
at Excavation level, at plinth level, at beam / slab level and at completion stage for issue of<br />
completion certificate.<br />
2. The consultant, at his own cost, shall check the quality of the materials brought on the<br />
site of work and ensure that the materials are in accordance with the specifications generally<br />
prescribed for the work. The laboratory test results of the materials tested is submitted to<br />
district CEO, ZP.<br />
3. consultant should remain present in the co-ordination / review meeting to be held at<br />
State level or at District level once in a month or earlier as required (at no extra cost.)<br />
4. As per the intimations, the consultant or his authorized Engineer should accompany to<br />
the IDW Engineers when they take site visits / organize meetings at District level.<br />
5. If any deviation in design / construction or compromise in quality is observed during the<br />
site visit of consultant, it should be immediately reported to CEO, ZP at district level and SE,<br />
IDW, Mumbai for further action.<br />
6. Consultant shall organize with his own arrangement and equipment, at his cost, a one<br />
day workshop to impart training to District IDW Engineers at mutually agreed suitable place at<br />
district. The expenses towards the TA & DA of participants except the consultant) will be borne<br />
by NRHM. A suitable place will be made available free of cost to consultant for arranging such<br />
training program.<br />
7. The consultant shall appoint two Engineers (Minimum Qualification B.E. Civil) for each<br />
district. If the no. of works in any district is more than 500 then an extra Engineer for 250 works<br />
should be appointed.<br />
8. Consultant shall submit monthly report about the general progress of the works (for<br />
each work).<br />
9. Consultant should suggest the remedial measures to be carried out if any defects are<br />
noticed, during construction.<br />
10. Consultant should suggest the ways and means for economical construction. (To reduce<br />
the cost of construction without affecting quality of work.)<br />
11. Consultant should suggest methodology “to check and ensure the quality of work done”<br />
(by IDW Engineer) and check the work quality accordingly.<br />
12. Consultant shall not issue any instructions directly if in his opinion it is found necessary<br />
to change specifications or modify design. The same shall be brought to the notice of regional<br />
Executive Engineer and SE, IDW, Mumbai.<br />
Page | 41
<strong>13</strong>. The consultant shall have minimum 3 years’ experience in the field of civil works of<br />
similar magnitude to that of the works covered in the proposed project.<br />
14. Consultant shall have to prepare “Manual for good construction practices” and<br />
“Checklist” covering all the items to be executed as per the estimate and furnish it to IDW,<br />
Engineers.<br />
15. After the work is completed consultant shall issue completion certificate as per format<br />
approved by SE, NRHM, Mumbai.<br />
The procedure for appointing such agency at state level is in progress and it is expected<br />
that the agency will be fixed up to the end of March <strong>2012</strong>. Hence provision for the above<br />
activity is necessary in PIP <strong>2012</strong>-<strong>13</strong>.<br />
Provision is done on lump sum basis i.e. @ 2.0% of the total budget for civil<br />
construction. The total budget for civil construction (i.e. Mission <strong>flexipool</strong> + Minor civil works<br />
for FRUs and 24 x 7 PHCs) is 88.66 + 2.25 + 6.03 = 96.94 Crores.<br />
Hence budget required for third party evaluation of civil works is :-<br />
2.0 % x 9694 (Lakhs) = 194 Lakhs.<br />
SUBSECTION B.5.12: STRENGTHENING OF PROGRAM MANAGEMENT UNIT<br />
Maharashtra had requested budget for three activities. These are Repairs of BPMU/DPMU, new<br />
construction of BPMU / DPMU in non-tribal areas and new construction of BPMU/DPMU in<br />
tribal areas. This proposal is revised.<br />
In Maharashtra, 10 district HQ do not have District Hospital or any building or structure for<br />
office or quarters. It is becoming very difficult to keep total DPMU staff at one place in these<br />
places. Civil Surgeon is also not having any office or quarters to monitor the program. As NRHM<br />
is now entering second phase, it will be very useful for districts to build own office at these<br />
places.<br />
This activity was again discussed during 6-8 June <strong>2012</strong> meeting. It was advised that one DPMU<br />
complex may be developed in each of the 10 Medical Colleges. Ground floor of the complex will<br />
be medicine store of around 3000 Sq feet and first floor will be office of the Civil Surgeon and<br />
other DPMU staff of the district. Accordingly budget is requested for this activity as follows. All<br />
remaining activities are discontinued.<br />
Budget requirement<br />
Budget required for this activity is as follows:<br />
Table – Budget requirement for BPMU/DPMU<br />
Rs. In Lakhs<br />
Page | 42
Sir Particulars Unit cost<br />
1<br />
No. of<br />
block<br />
Budget<br />
required<br />
New Construction or repairs of DPMU in<br />
10 districts.<br />
96 10 960<br />
Total 960<br />
SUBSECTION B.5.<strong>13</strong>: STRENGTHENING OF NURSING SERVICES<br />
Given the current problem of availability of trained nurses in the state, NRHM seeks to try a range of<br />
innovations and experiments to improve the position. These include strengthening of Nursing/ANM<br />
training schools and colleges to produce more paramedical staff, special batches of tribal students in<br />
private nursing schools, providing scholarships and loans to poor students to complete course in <strong>rural</strong><br />
areas, higher salary, etc.<br />
Sr<br />
Table – : Requirement of nursing staff and current capacity of nursing schools<br />
Health institute and<br />
nursing staff/inst.<br />
No. of<br />
institutions<br />
Requirement of staff Training capacity<br />
Regular Contra. Total of govt. Schools<br />
1 SHC – 2 ANMs 10579 10579 10579 21158 940<br />
2 PHC – 1 LHV 1816 1816 1816 3632 225<br />
3<br />
4<br />
PHC – 3 Staff Nurses<br />
RH – Staff Nurse<br />
1816<br />
453<br />
0<br />
2718<br />
5448<br />
<strong>13</strong>59<br />
5448<br />
4077<br />
360<br />
Plan for year <strong>2012</strong>-<strong>13</strong><br />
Considering the importance of availability of trained nursing staff to achieve the objectives of NRHM,<br />
various steps are proposed to be taken to increase the availability of trained nurses in the state.<br />
Important steps to be taken during year 2011-12 are mentioned below:<br />
• Strengthening of all nursing schools as per MNC norms<br />
• Repairs or New construction of nursing schools or hostels wherever necessary<br />
• Repairs or new construction of annex buildings<br />
• Public Private Partnership<br />
Budget requirement for year <strong>2012</strong>-<strong>13</strong><br />
As need of nurses has increased many fold after introduction of NRHM, ad<strong>mission</strong> capacity of all the<br />
Nursing Schools is increased two or three folds. This has resulted into increase in requirement of basic<br />
facilities such as classrooms, hostels, annex buildings (places of field practice), addition of books, models<br />
and teaching aid as per MNC norms, etc. Major part of the requirement is being borne by state<br />
government, however, gaps are being filled under NRHM for specific matters. Budget requested by<br />
District Societies is submitted below as average budget requirement for the construction work of<br />
Nursing schools.<br />
As discussed in 6-8 June meeting, GoI is independently providing budget to Nursing Schools. Budget<br />
provision of GoI outside the NRHM budget is as follows:<br />
Page | 43
• Rs. 50 Lakh for strengthening of nursing schools at Latur and Kolhapur.<br />
• Training material to three new nursing schools (Pusad, Sindhudurg, Washim) – Rs. 8.36 Lakh<br />
• Construction of Main building, hostel and annex building of new Nursing Schools (Pusad,<br />
Sindhudurg, Washim) – Rs. 42.53 Crores.<br />
As mentioned above, budget is provided for five nursing schools. These schools are not proposed budget<br />
for civil works under this activity.<br />
Budget will be required for following purposes:<br />
Table – : Budget required for strengthening of nursing services<br />
Sr Particulars Unit price<br />
No. of<br />
units<br />
Rs. In Lakh<br />
Total<br />
budget<br />
required<br />
1 Repairs of Annex building 6 31 186<br />
2 New construction of annex building 55 3 165<br />
3 Repairs and new construction of main building 44 4 176<br />
4 Repairs and new construction of hostel building 27 8 216<br />
Total 743<br />
SUBSECTION B.5.14: CONSTRUCTION WORK IN HIGH FOCUS DISTRICTS<br />
As per discussion with GoI officials, shifted from B.25 to Construction section (B.5)<br />
1. NANDURBAR DISTRICT<br />
Nandurbar district is 100% tribal district in North Maharashtra. High ranges of Satpuda<br />
Mountain ranges and Narmada River along with backwaters of Sardar Sarovar has made more<br />
than 30% of the villages very remote and not accessible by road. This is one of the important<br />
reasons for poor performance of the districts in <strong>health</strong> indicators. Considering the situation of<br />
the district, following activities / schemes are proposed for Nandurbar district.<br />
a. New Construction / repairs of quarters of RH/SDH and PHCs<br />
Areas in Nandurbar are so interior that there is no facility for staying of the <strong>health</strong> staff in the<br />
village. Presently provided quarters require large repairs and also not adequate. It is proposed<br />
to repair the existing quarters and to build quarters for one driver, two nurses and one<br />
attendant in each of the hospital and PHCs.<br />
Budget required for this activity is as follows:<br />
Table – Budget requirement for Civil Works<br />
Page | 44
Sir Activity<br />
A Repairs of the quarters<br />
Unit<br />
cost<br />
units<br />
Budget<br />
required<br />
1 PHC quarters 17 14 238<br />
2 RH Quarters 52 4 208<br />
Total Repairs 446<br />
B New Construction of quarters<br />
1 PHC quarters 55 6 330<br />
2 RH quarters 55 4 220<br />
Total new construction 550<br />
Grand Total 996<br />
2. GONDIA DISTRICT:<br />
Construction of MPW quarter in sub center building in highly naxal affected blocks<br />
(Deori, Salekasa, Arjuni/ Mor.)<br />
MPW and ANM works at sub center to cater <strong>health</strong> services .In the difficult and naxal<br />
affected area there is always scarcity of transportation. Thus to cater the services round<br />
the clock one of the MPW/ANM is expected to reside at Sub center premises. Thus<br />
construction of MPW quarter is required at such area.<br />
Construction of Staff Quarter in RH<br />
There is no staff quarters available at RH Amgaon of Gondia district .To cater the<br />
services round the clock staff should reside in the campus of Hospital. Thus quarters for<br />
these staff at Hospital vicinity is proposed.<br />
Construction of Staff Quarters in WH, DH & RH<br />
Residential Quarter for Hospital employees. With a view to provide 24 hour <strong>health</strong><br />
services to the patients attending RH . The <strong>health</strong> staff need to available in hospital<br />
premises because of non-availability of residential quarter most of the employees in 3<br />
RH stay outside the premises and they are not in position to render quick services to the<br />
needy patients.<br />
Construction of Staff Quarters in PHC<br />
With a view to provide 24 hour <strong>health</strong> services to the patients attending PHC . The<br />
<strong>health</strong> staff need to available in hospital premises. But because of non-availability of<br />
residential quarter most of the employees in 4 PHCS stay outside the premises and they<br />
are not in position to render quick services to the needy patients.<br />
Page | 45
Table: Budget required for Gondia under Special Action Plan<br />
Section Activities No. Of Unit<br />
Cost per<br />
Unit<br />
Total<br />
Budget<br />
1<br />
Construction of MPW quarter in sub center<br />
building in highly naxal affected blocks (Deori,<br />
Salekasa, Arjuni/ Mor.)<br />
39 9 351<br />
2 Construction of Staff Quarter in RH 1 100 100<br />
3 Construction of Staff Quarters in WH,DH& RH 3 60 180<br />
4 Construction of Staff Quarter in PHC 4 22.35 89.4<br />
GADCHIROLI DISTRICT:<br />
Total 720.4<br />
New construction of Ware House<br />
A large quantity of medicine is supplied to PHCs and Hospitals as this is special focus<br />
district. At present there is no sufficient and convenient storage facility available for<br />
storage of this huge quantity of medicines and consumable. It is proposed to construct<br />
one Warehouse in the premises of District Hospital for both the DHO and Civil Surgeon.<br />
Thus construction of new warehouse at District level is proposed for safe storage and<br />
distribution of Medicine and consumables.<br />
Construction of Dharmashala at DH<br />
As DH is the only place to receive specialty care in district, large number of tribal<br />
patients attends the DH and SDH Aheri daily. These poor patients do not have any<br />
facility to stay. As monsoon of this area is very strong, patients are at very much<br />
hardship. Therefore it is proposed to construct shelter (Dharmashala) for poor patients<br />
one each at Gadchiroli and Aheri. This will consist of two halls one kitchen room with<br />
platform and two sanitary blocks (separate for men and women).<br />
New construction of MPW Quarter at Sub Centre<br />
One ANM and a MPW are appointed at sub center to cater basic <strong>health</strong> care at village<br />
level. One of these is supposed to be available on 24 hrs. basis for serving the<br />
population. Thus construction of MPW quarters at well-performing subcentres are<br />
proposed in the special action plan.<br />
New construction of Medicine store Room at Primary Health Centre<br />
Page | 46
PHCs are catering <strong>health</strong> services in the form of OPD as well as IPD(6 beds or<br />
more).Availability and storage of medicine is very important at the PHC itself. At present<br />
32 PHCs in the district haven’t their medicine store. Therefore, construction of 32<br />
medicine store rooms are required in these PHCs.<br />
New construction of 20 Bedded EYE Ward at District Hospital<br />
Gadchiroli District hospital caters various specialty services to <strong>rural</strong> population. There is<br />
no separate ward for ophthalmology patients in this hospital. Ophthalmology patients<br />
need to stay in the hospital for cataract surgeries and in case of ophthalmic<br />
emergencies. Separate 20 bedded eye ward is proposed for this purpose.<br />
New construction of Trauma Ward at District Hospital<br />
Gadchiroli is tribal and naxalite affected area. Naxalite activities used to occur in this<br />
district which leads to large no. of trauma emergencies . To handle these emergencies at<br />
present no separate trauma ward in DH. All these emergencies come to DH ,hence<br />
trauma ward construction is proposed.<br />
New construction of Type- IV Quarter at District Hospital<br />
DH Gadchiroli is a big <strong>health</strong> facility and a large no. of Class IV employees works for the<br />
hospital. Residence quarters for these employees are less as compare to no. of<br />
employees .So to accommodate all class IV employees additional 18 quarters are<br />
needed.<br />
Table: Budget required for Gadchiroli under Special Action Plan<br />
Sir Name of Activities/initiative Unit cost<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
2<br />
New construction of Ware House at District Health<br />
Officer<br />
90 1 90<br />
3 New construction of MPW Quarter at Sub Center 8 10 80<br />
4<br />
New construction of Medicine store Room at<br />
Primary Health Center<br />
4 15 60<br />
5<br />
New construction of 20 Bedded EYE Ward at District<br />
Hospital<br />
100 1 100<br />
6<br />
New construction of Trauma Ward at District<br />
Hospital and Dharmashala<br />
115 1 115<br />
7<br />
New construction of Specialist Room at District<br />
Hospital<br />
15 5 75<br />
Page | 47
8<br />
New construction of Type- IV Quarter at District<br />
Hospital<br />
22 18 396<br />
Total 916<br />
SUBSECTION B.5.15 : STRENGTHENING OF HIGH UTILIZATION PHCs and HOSPITALS<br />
In Maharashtra, utilization of Hospitals is fairly good. Utilization of some of the <strong>health</strong> facilities<br />
is very high. It is proposed that PHCs with very high delivery rate and Hospitals with more than<br />
90% bed occupancy rate will be strengthened. Requirement of additional wards, Operational<br />
theater, labour room, OPD complex, laboratory complex, Blood bank, water supply,<br />
electrification, diet and laundry facility and also quarters for important staff required for 24<br />
hours services (excluding managerial staff) will be fulfilled for such highly utilized hospitals.<br />
Budget requested below is block estimates of the requirement as prescribed by IDW Engineers.<br />
Once the activity is approved, exact estimates will be prepared by the PWD for these works.<br />
Maharashtra PWD has appointed one Chief Engineer level officers from PWD as Co-ordination<br />
Officer for all the works to be undertaken under NRHM grants. One Construction Tracker is also<br />
developed for tracking all the constructions. Beside this, now regular meetings of Executive<br />
Engineers and Civil Surgeons are being carried out by Health Department to get the works<br />
faster and in time.<br />
Following groups are considered for additional help to <strong>health</strong> facilities<br />
i. Primary Health Centers with more than 50 deliveries per month (6)<br />
ii. SDH with more than 80% bed occupancy (1)<br />
iii. Women hosptials with more than 80% bed occupancy (4)<br />
iv. District Hosptials with more than 80% bed occupancy (6)<br />
Group wise budget requirement of <strong>health</strong> facilities is as follows:<br />
Sr Name of the activity<br />
No. of deliveries in<br />
2011-12<br />
Table – Budget required for Primary Health Centers<br />
Sonpeth<br />
dist<br />
Parbhani<br />
Dongaon<br />
Dist<br />
Buldhana<br />
Name of the PHC<br />
PHC<br />
Walur<br />
Dist<br />
Parbhani<br />
Sakharshet<br />
Dist Thane Barahali<br />
Lasur<br />
Stn<br />
Dist<br />
Abad<br />
1501 703 654 493 447 588<br />
Rs. In Lakhs<br />
Total<br />
budget<br />
requiremetn<br />
Page | 48
Sr Name of the activity<br />
1<br />
2<br />
Extension of Labour<br />
Room<br />
Female Ward for<br />
delivery cases<br />
Sonpeth<br />
dist<br />
Parbhani<br />
Dongaon<br />
Dist<br />
Buldhana<br />
Name of the PHC<br />
PHC<br />
Walur<br />
Dist<br />
Parbhani<br />
Sakharshet<br />
Dist Thane Barahali<br />
Lasur<br />
Stn<br />
Dist<br />
Abad<br />
Total<br />
budget<br />
requiremetn<br />
4.5 1.5 2 2.5 2.5 2 15<br />
16 4.5 4 5 0 4.5 34<br />
3<br />
Construction/repairs<br />
of Laboratory<br />
3 0 2.5 3 0 2.5 11<br />
4<br />
Medicine Store<br />
Room<br />
2.5 2.5 0 2.5 0 2 9.5<br />
5 MO quarters 18 18 18 18 36 17 125<br />
6 Driver quarter 12 12 12 12 12 12 72<br />
7<br />
Twin Quarter for<br />
nurses<br />
Construction of one<br />
48 36 24 44 44 24 220<br />
additional toilet 1.5 0 2 2.5 3 2 11<br />
8 block<br />
9<br />
Repairs of Sanitaory<br />
block and drainage<br />
system<br />
1.5 2.5 1 5 0 0 10<br />
Water Supply<br />
system and water<br />
storage system for<br />
24 hours water<br />
8 3 2.5 9 0 2 24.5<br />
10 supply<br />
11 Kitchen Shed 2.5 0 2 2 2 2 10.5<br />
12 Electrification 3 3 3 0 0 2.5 11.5<br />
<strong>13</strong> Internal Roads 12 0 10 12 8 0 42<br />
Total <strong>13</strong>2.5 83 83 117.5 107.5 72.5 596<br />
Table – Budget required for Sub-District Hosptials<br />
Rs. In Lakhs<br />
Sr Name of the activity Name of the Hospital<br />
Facility Jawahar<br />
Bed Occupancy 92.93<br />
1 Dedicated labour room for inf cases 45<br />
2 Additional Female Ward for delivery cases 78<br />
Page | 49
Sr Name of the activity Name of the Hospital<br />
3 Establishment of NBSU 0<br />
4 Repairs of OT 20<br />
5 Repairs of Laboratory 9.06<br />
6 Repairs of Blood Storage Unit 30.18<br />
7 reapirs of x-ray 7<br />
8 Reapis of ICU 40<br />
9 Repairs of blood bank & dental room 7<br />
10 Reapirs of labour ward 3<br />
11 Kitechen room 7<br />
12 Medicine Store Room 85<br />
<strong>13</strong> Doctors quarters 22<br />
14 Driver quarter 56<br />
15 Nurses quarters 356<br />
16 Repairs of Sanitaory block and drainage system 40<br />
17<br />
Water Supply system and water storage system for 24 hours water<br />
supply 20<br />
18 Electrification 70<br />
19 Waiting room 20<br />
20 Gardening and planting 10<br />
21 Internal Road 25<br />
22 Septic Tank 20<br />
23 Dhobi Ghat 5<br />
24 Denatl Room 15<br />
25 Fire Extinguisher 14<br />
Total 1004.24<br />
Table – Budget required for Women Hosptials<br />
Sr Name of the activity Name of the Hospital<br />
Rs. In Lakhs<br />
Total budget<br />
requirement<br />
Facility Jalna Amravati Akola Thane<br />
Bed Occupancy 148.69 125.4 124.43 85.61<br />
Repairs of existing labour room<br />
1 and addtioal labour room for inf<br />
cases<br />
18 14 27 24 83<br />
2<br />
Additional Female Ward for<br />
delivery cases<br />
140 76 105 112 433<br />
Page | 50
Sr Name of the activity Name of the Hospital<br />
Total budget<br />
requirement<br />
Establishment of NBSU 0 0 0 0 0<br />
Repairs of OT 24 16 19 23 82<br />
Repairs of Laboratory 14 19 21 14 68<br />
Repairs of Blood Bank 9 44 35 0 88<br />
3 Medicine Store Room 12 12 <strong>13</strong> 15 52<br />
4 Doctors quarters 784 615 541 225 2165<br />
5 Driver quarter 36 49 35 22 142<br />
6 Nurses quarters 54 550 468 596 1668<br />
7<br />
8<br />
Repairs of Sanitaory block and<br />
drainage system<br />
Water Supply system and water<br />
storage system for 24 hours<br />
water supply - pump and<br />
harvesting<br />
207 38 35 32 312<br />
47 12 26 11 96<br />
9<br />
Electrification - repairs and new<br />
90 <strong>13</strong> 16 64 183<br />
11 Security guard Cabin 10 5 0 5 20<br />
12 Internal Road 115 <strong>13</strong>4 121 98 468<br />
<strong>13</strong> Gardening 25 15 15 5 60<br />
14 Installing transformer MSEB 20 0 0 0 20<br />
Total 1605 1612 1477 1246 5940<br />
Table – Budget required for District Hosptials<br />
Sr Name of the activity District wise budget<br />
Rs. In Lakhs<br />
Total<br />
budget<br />
requiremetn<br />
Facility Chandrapur Amravati Bhandara Osmanabad Ratnagiri Hingoli<br />
Bed Occupancy 119.78 100.6 91.36 89.74 89.71 84.9<br />
1<br />
Repairs of existing labour<br />
room and addtioal labour<br />
room for inf cases<br />
41 0 32 33 150 52 308<br />
2 Additional Female Ward<br />
for delivery cases<br />
72 0 145 <strong>13</strong>3 142 156 648<br />
3 Establishment of NBSU 0 0 0 0 0 0 0<br />
4<br />
Construction of Obstretic<br />
ICU<br />
0 0 156 106 55 114 431<br />
5 Repairs of OT 58 55 86 74 87 79 439<br />
6 Laboratory - repairs and<br />
new constructin<br />
23 71 85 64 16 78 337<br />
7 Repairs of Blood Storage 0 0 0 0 0 0 0<br />
Page | 51
Sr Name of the activity District wise budget<br />
Unit<br />
Total<br />
budget<br />
requiremetn<br />
8 Wards 105 117 173 149 0 165 709<br />
9 Burns ward 72 54 46 51 16 51 290<br />
10 Speciality wards 204 194 2<strong>13</strong> 258 205 198 1272<br />
11 Medicine Store Room 54 52 48 42 50 22.4 268.4<br />
12 Kitchen repairs 23 26 19 21 18 18 125<br />
<strong>13</strong> Kitchen shed for patient<br />
relatives<br />
14 11 0 11 15 14 65<br />
14 Doctors quarters 150<br />
155 145<br />
1611<br />
15 Driver quarter 42 205 44 52 415 541 <strong>13</strong>8<br />
16 Nurses quarters 206 314 312 832<br />
17 Lift construction/repair 35 1 41 36 35 24 172<br />
18 X - ray room 18 19 21 18 18 20.6 114.6<br />
19<br />
Repairs of Sanitaory block<br />
and drainage system<br />
198 84 104 41 114 89 630<br />
20<br />
Water Supply system and<br />
water storage system for<br />
24 hours water supply<br />
75 84 68 27 69 81 404<br />
21 Electrification 88 59 74 85 38 47 391<br />
22<br />
Shed and canteen for<br />
relatives 15 15 19 17 18 52 <strong>13</strong>6<br />
23 Express feeder 0 0 0 0 85.91 0 85.91<br />
24 OPD Complex 0 0 0 212 151.21 0 363.21<br />
25 Land<br />
Development/scaping<br />
18 41 12 14 19 20 124<br />
26 Cattle trap & main<br />
0 0 0 0 0 3 3<br />
entrance gate<br />
27 Internal roads 105 89 97 85 74 34 484<br />
Total 1616 1177 1952 1986 1791.12 1859 10381.12<br />
Summary of budget requested is as follows:<br />
Table – Summary of budget required for High Utilisation Health Facilities<br />
Rs. In Lakhs<br />
Budget<br />
Sr Type of <strong>health</strong> faciliyy<br />
requrested<br />
1<br />
Primary Health Centers with more than 50 deliveries per month (6)<br />
596<br />
2 SDH with more than 80% bed occupancy (1) 1004.24<br />
Page | 52
3<br />
4<br />
Women hosptials with more than 80% bed occupancy (4)<br />
District Hosptials with more than 80% bed occupancy (6)<br />
5940<br />
10388.12<br />
Total 17928.36<br />
SECTION - B.6 : CORPUS GRANT TO HMS/RKS<br />
Approval in ROP accepted.<br />
SECTION : B.7 : PREPARATION OF DISTRICT HEALTH ACTION PLANS<br />
For preparation of District Action Plan, Rs. 1.0 Lakh is provided per district and State is provided<br />
Rs. 5.0 Lakh. In Maharashtra, DHAP preparation is carried out as per GoI guidelines for DHAP by<br />
steps given below:<br />
1. One day Dissemination Workshop of RCH Officers, DPM and DAM at state level to<br />
communicate GoI guidelines for the year for DHAP. Formats are circulated and detailed<br />
planning is discussed.<br />
2. Same meeting is organized at district level of MO PHC and MS Hospitals and other<br />
officers of Disease Control Programs. Printed formats are distributed to all the PHCs and<br />
Hospitals.<br />
3. PHC workshop is organized after district meeting. Village plans are discussed and<br />
formats distributed.<br />
4. Village plans prepared in one week and submitted to Village Health Committee.<br />
5. MO PHC and supervisor meet at block level and PHC level plans are prepared at Block<br />
level. This meeting is conducted at 353 block HQ. Approval of RKS is taken. Hospital<br />
plans are prepared at hospital level and submitted to RKS.<br />
6. MS of Hospitals, THO, 1-2 MO and supervisors meet at district level to prepare block<br />
level plan. This plan is submitted to Block Health Mission.<br />
7. All block plans are collected and one week workshop is conducted at HFWTC level of all<br />
districts. RCH Officer, RMO (O), DPM, DAM, Dist Supervisors (6 persons from one<br />
district) attend this workshop. DHO and Civil Surgeon attend the workshop on 4 th and<br />
5 th day to finalize the plan.<br />
8. The prepared plan is submitted to District Mission and after approval of <strong>mission</strong>,<br />
submitted to state.<br />
9. Principal HFWTC, his staff, Deputy Director Circle and his staff are travelling from day of<br />
MO preparation meeting to sub<strong>mission</strong> of plan.<br />
Page | 53
10. All the plans are prepared by our own staff without any help of consultants.<br />
GoI has approved only Rs. 38 Lakhs for the total exercise. With this exercise, it will not be<br />
possible to conduct PHC level, block level and district level workshops and as HFWTCs and<br />
Circles are not given budget, no supervisory visits can be conducted.<br />
Experience of Maharashtra of last four years indicate that calling all blocks at district level and<br />
calling all districts inc] circle at HFWTC helps in developing quality plans.<br />
As per GoI guidelines, NRHM has allowed up to Rs. 20.0 Lakh per district for DHAP. This budget<br />
is 25% of the guidelines.<br />
If bottom up approach as per DHAP guidelines is to be followed, it is very difficult to prepare<br />
plans in approved amount. Therefore it is requested to approve the budget as proposed.<br />
Budget requirement<br />
This issue was discussed during 6-8 June Meeting at New Delhi. It was decided that budget for<br />
DHAP will be provided as per expenditure of year 2011-12. Accordingly budget requirement is<br />
submitted as follows:<br />
Table –: Budget required for preparation of PIP for year <strong>2012</strong>-<strong>13</strong><br />
Sir Particulars<br />
PIP<br />
Exp.<br />
prep.<br />
10% add<br />
Rs. In Lakhs<br />
Budget<br />
required for<br />
yr <strong>2012</strong>-<strong>13</strong><br />
1<br />
District Health Action Plan at block<br />
level<br />
143.24 157.564 160<br />
2<br />
HFWTC for Preparation<br />
Compilation workshops<br />
and<br />
7.99 8.789 9<br />
3 Circle offices for supervision 0.03 0.033 1<br />
4<br />
State PIP (All components - meeting,<br />
review, printing, etc)<br />
35 38.5 40<br />
Total 210<br />
Page | 54
SECTION - B.8 : PANCHAYATI RAJ INITIATIVE<br />
SUBSECTION - B.8.1 : & B.8.2 : CONSTITUTION AND ORIENTATION OF COMMUNITY LEADERS<br />
AND VHSC, SHC, PHC, CHC, ETC<br />
Approval received. Accepted.<br />
SUBSECTION - B.8.2 : GUIDED TOURS FOR MLAs, MLCs AND OFFICE BEARERS OF ZILLA<br />
PARISHADS<br />
Approvals received. Accepted.<br />
SECTION - B.9 : MAINSTREAMING OF AYUSH<br />
GoI has approved almost all the sub-components of the program. However, re-consideration is<br />
requested for only one activity as mentioned below:<br />
TA/DA to AYUSH Coordinators : TA/DA of Rs. 12.25 Lakh for AYUSH Coordinator was<br />
requested. There is no other source of budget for this activity. Therefore TA/DA for tours may<br />
be approved. Otherwise, review meetings and monitoring will be difficult in AYUSH program.<br />
As per discussion during 6-8 June meeting, provision of AYUSH facility to Women Hospitals is<br />
shifted to Chapter B.15 : Innovations.<br />
Rest of the activities in AYUSH acceptable as per ROP.<br />
SECTION - B.10 : IEC/BCC UNDER MISSION FLEXI-POOL<br />
Introduction :<br />
Maharashtra is considered to be one of the better developed state of India.<br />
However there are considerable variations in language, culture and social setup. While<br />
implementing IEC BCC activities. We have to focused on local needs and linked with expected<br />
out come of <strong>health</strong> goals.<br />
State focus for IEC/BCC will be on following issues.<br />
1) Reduction of MMR<br />
2) Reduction of Anaemia in mothers, children and adolescent girls.<br />
3) Reduction of IMR<br />
4) Reduction of TFR<br />
Page | 55
5) Improving age at Marriage<br />
6) Adolescent Reproductive and Sexual <strong>health</strong><br />
Currently in Maharashtra the MMR is 104, the state has setup goal for reduction<br />
it < 90 by 20<strong>13</strong>. To achive this goal IEC BCC will focused on Inter Personal Communications<br />
activities, cultural programmers and various compitations for women groups. Awareness will<br />
be generated through community & electronic media regarding Intuitional delivery, J.S.Y, JSSK,<br />
ARSH, immunization, PCPNDT, family planning etc.<br />
Child <strong>health</strong><br />
While considering the status of child <strong>health</strong> indicators IEC BCC activities will be<br />
implemented to achieve the following goals.<br />
1) Reduction in neonatal mortality from 29 to 20 and reduction of IMR from 33 to 27<br />
2) Immunization coverage up to 85%<br />
3) Early breast feeding up to 65%<br />
4) Reduction in grade 3 and grade 4 malnutrition.<br />
For achieving the goals the activities like mother counseling, groups meetings<br />
<strong>health</strong>y baby computations, will be implemented. Awareness will be generated through<br />
community and, Folk media, special women’s camps will be organized in <strong>rural</strong> area.<br />
Family Planning<br />
The Maharashtra has always been in the forefront in the implementation of<br />
family planning programme. State has declared Population policy. According to policy state has<br />
accepted 2 children family as a small family norm.<br />
Awareness generation activities will be implemented for increase the acceptance<br />
of NSV, Use of contraceptives, sterilization, acceptance of IUD etc. through IPC, Folk media,<br />
Health melas, Exhibitions and Electronic media.<br />
10.1 IEC Strategy :<br />
IEC strategy development requires decisions with respect to three key questions :<br />
Whom to address, that is identification of target groups.<br />
What do we want to say to them that is selection of messages contents .<br />
What communication method should we use to deliver a specific message to a particular target<br />
group, that is media selection.<br />
In Maharashtra state for planning, implementation and monitoring of IEC/BCC<br />
activities an independent state Health IEC Bureau is established in the year 1996 which is<br />
headed by the Deputy Director of Health Services, a mass Media Specialist. Every district has a<br />
small IEC unit of 2-3 officials functioning under the supervision of District Health Officer.<br />
Page | 56
Planning, implementation and monitoring of various IEC/BCC activities under<br />
Reproductive and child Health Programme as well as other various <strong>national</strong> <strong>health</strong> programmes<br />
are being carried out throughout the year through the state Health IEC Bureau. Maharashtra<br />
Arogya Patrika a monthly magazine in Marathi is being published and circulated regularly by<br />
the State Health IEC Bureau for continuous <strong>health</strong> education to <strong>health</strong> providers and<br />
community in the State. Parivartan Express, a very unique a audio visual Van is run by State<br />
Health IEC Bureau. Various activities such as <strong>health</strong> exhibitions, film shows are organized<br />
throughout the State with the help of Parivartan Express.<br />
Areas to be focused<br />
- Mother <strong>health</strong> - Child care<br />
- Immunization - Spacing<br />
- Family Planning - Adoselant <strong>health</strong><br />
- Diet - Safe Abortion<br />
- PCPNDT - Institutional Delivery<br />
- Breast Feeding - Ayush<br />
- Janani Surksha Yojana - TB Control<br />
- Janani Shishu Surksha Karyakram - Malaria, Dengue, Chikungunya<br />
- Rugn Kalyan Committee - Water barn diseases<br />
- Child Develapment Center - Non Communicable diseases<br />
- Village & Sanitation Committees - Blindness Control<br />
- Nutrition - Sickle cell Control<br />
- Mental Health<br />
Target groups<br />
Three segments we need to be included in the target audience for all institutions<br />
Govt. functionaries working at the grass root level- Ashas, ANMs Anganwadi<br />
workers, Gramsevikas, school teachers, extension workers & multi purpose <strong>health</strong> workers –<br />
should be targeted for information pertaining to what <strong>health</strong> services are available and where.<br />
These workers are likely to be seen as opinion leaders by the population. They serve & they can<br />
be key information sources in spreading knowledge about the working of the referral system .<br />
Women are be considered as priority target : they are ,managers of the<br />
households <strong>health</strong> status & have also demonstrated their capacity as a group to mobilize<br />
community response.<br />
Page | 57
Patients who enter the hospitals & <strong>health</strong> centre’s are considered a priority<br />
target There word-of-mouth as satisfied user will carry far more weight than any other channel<br />
of communication strategy to succeed improvement in quality clinical care & proper counseling<br />
of user may serve this purpose<br />
The community at large also constitutes an important target group since the<br />
initiative taken by community leaders and other stakeholders<br />
IEC for whom<br />
- ANM’s<br />
- Ashas<br />
- Anganwadi Workers<br />
- Health Workers<br />
- School teachers<br />
- NGO Workers<br />
- Other Service Providers<br />
- Mothers<br />
- Women's<br />
- Girls & Boys<br />
- General Community<br />
- Community Leaders<br />
- Panchayat members<br />
- Elected representatives<br />
- Social Workers<br />
- Doctors<br />
- Media Persons<br />
Methods & Media<br />
Often media such as print or electronics, dominates any mention of IEC whereas<br />
methods of communication are neglected. The IEC bureau will correct this imbalance of<br />
emphasis by underscoring the methods & media according to their role and contribution in<br />
behavior change. In the state of Maharashtra where for example awareness of family planning<br />
appears to be universal the role of mass media becomes secondary (basically to support re –<br />
enforce re- assure message) to two way channels of communication such as group approach<br />
inter-personal communication & counseling these approaches help a potential user of<br />
contraceptives to make the crucial decision of adopting the practice, by clarifying & doubts &<br />
misconceptions he or she might have.<br />
Community participation is another important approach in IEC. Community will be involved<br />
at all levels from strategy, planning to programme evolution.<br />
Electronic Media<br />
Electronic media such as radio and T V are the most powerful channels of<br />
communication, for creating awareness of <strong>health</strong> issues. Electronic media when used in a<br />
Page | 58
planned and creative way can be the most cost-effective way to inform and reassure people.<br />
Production of high quality T V and radio programmes is, however, a complex and technical task.<br />
Selection of Media<br />
1) Print Media<br />
- Handbills<br />
- Folders<br />
- Flip Booklets<br />
- Posters<br />
- Banners<br />
- News Papers, Advertisement<br />
- Message through electricity bills<br />
2) Electronics Media<br />
- T. V.<br />
- Radio<br />
- Local Cable<br />
- SMS<br />
- F M Stations<br />
- Scrolling boards<br />
3) Community Media<br />
- Rallies<br />
- Falk art<br />
- Film shows<br />
- Exhibitions<br />
- Health Melas<br />
- Floats<br />
Page | 59
- Hoardings<br />
- Wall Painting<br />
4) Group Media (I.P.C.)<br />
- Home visits<br />
- Small group meetings<br />
- Personal visits<br />
- Religious Functions<br />
- Haldi-Kum-Kum Programme<br />
- Immunizations<br />
10.2 Implementation of Strategy<br />
While implementing IEC / BCC Plan following issues will be focused.<br />
(1) Message will be well designed to solve the indentified <strong>health</strong> problems and<br />
issues.<br />
(2) IEC / BCC Messages, Material and media will be linked with programme<br />
objectives.<br />
(3) Intergrated approach will be adopted for implementing IEC / BCC activities.<br />
(4) Programmes will be strictly monitored for timely dispatch of IEC material to<br />
proper destination and its utilization.<br />
(5) Instead of mass media approach, IPC approach will be adopted for disseminate<br />
the message among the <strong>rural</strong> masses.<br />
(6) The district will be focal point for developing local specific IEC.<br />
(7) Special training programme will be organized for developing the communication<br />
skills of service providers and IEC personals.<br />
(8) State will encourage the Best IEC practices.<br />
(9) Role of different functionaries for implementation and supervision will be<br />
ensured.<br />
(10) Decentralized and participatory approach will be adopted.<br />
(11) Service providers at grass root level will be equiped with proper IEC material and<br />
methods.<br />
(12) Media people as well as journalists will be encouraged with best awards.<br />
(<strong>13</strong>) Health Meals will be organized for mass awareness.<br />
(14) Mass publicity campaigns will be organized for declining the sex ratio.<br />
Page | 60
Activities (B. 10.2.1 to B.10.2.4)<br />
Inter personal communication<br />
For behavior change, Inter personal communication is very effective tool. For this<br />
purpose. Counseling and interactive sessions with ASHAs, ANMs, and Anganwadi Workers,<br />
group meetings at village and block level, workshop for women groups, community leaders,<br />
adolescent groups at block and district level has been proposed. 358 workshops at block level<br />
@ Rs.5000) and 33 workshops at district level @ Rs. 10000 total Rs.21.20 lakh are proposed for<br />
the IPC activities.<br />
Community media – Folk Art:<br />
For creating awareness regarding various <strong>health</strong> porgrammes and projects, the activities<br />
like folk art, Rallies, Street plays have been proposed. 300 folk programmes @ Rs.4000 will be<br />
organized in each district. Provision of Rs. 396 lakhs is made in the PIP.<br />
Community media – Rallies:<br />
On occasion of <strong>health</strong> days, fairs and campaigns, 5 rallies in each district @ Rs. 10000<br />
will be organized. Rs. 16.50 lakhs have been proposed for 165 rallies.<br />
Electronic Media :<br />
To reach the masses, television and radio is the best option. The T.V. & Radio programs<br />
are watched by all classes of community. Various programs like serials, dances and music,<br />
News, discussions, interviews are telecasted and broadcasted for different target groups.<br />
considering the importance of T.V. & Radio following activities are proposed.<br />
• Telecasting of TV spots : Rs. 60,000/- per telecast x 475 telecasts = Rs. 285.00 lakhs.<br />
• Broadcasting of Radio jingles : Rs.<strong>13</strong>,000/- per broadcast x 500 = Rs.65.00 lakhs.<br />
Thus, a budget of Rs. 350.00 lakhs is proposed during the year<br />
<strong>2012</strong>-<strong>13</strong> for publicity through electronic media.<br />
Newspaper advertisements:-<br />
Newspaper is very popular and effective medium, through which <strong>health</strong> messages can<br />
be reached up to different target groups. Pictorial advertisements will be published in<br />
newspapers @Rs.15000/- per advertisement x 100 advertisements. Thus, a budget of Rs. 15<br />
lakh Proposed .<br />
Subsection – B.10.4: Health Mela<br />
For mass awareness regarding various <strong>health</strong> programs, <strong>health</strong> mela is the best<br />
opportunity. We can provide <strong>health</strong> check-up services as well as awareness campaign in the<br />
same mela. Health mela in each district will be organized. Each Mela will be for the period 1<br />
day. The mela will be organized in selected Sub district hospital premises or public ground. The<br />
facilities for <strong>health</strong> check-ups and diagnostic purpose will be provided to community by<br />
specialists. Health exhibitions, film shows, folk programs will be arranged in the mela. IEC<br />
material will be distributed to the beneficiaries.<br />
Page | 61
Pre-publicity of the camp through banners, posters, Davandi, Radio publicity will be<br />
done. Transport of public to the venue of Health mela, Remuneration of Private Specialist<br />
doctors (if requjired and mela expenditure will be required.<br />
Rs.5.00 lakhs x 33 Melas =Rs. 165.00 lakhs<br />
Subsection - B.10.5: Creating Awareness on Declining sex ratio issue<br />
Declining sex ratio is one of the big challenge before <strong>health</strong> services in the state. State is<br />
tackling this issue with creating awareness as well as implementations of law.<br />
For creating awareness, the media like T.V. Radio, Newspaper, hoardings, messages on<br />
electricity bills, Rallies, pictorial floats, banners, posters, exhibitions, folk programe will be<br />
utilized.<br />
(1) Telecasting of TV spots : Rs. 60000/- per telecast x 100<br />
telecasts = Rs.60.00 lakhs.<br />
(2) Broadcasting of Radio Jingles : Rs. <strong>13</strong>,000/- per broadcast x 46<br />
broadcasts = 06.00 lakhs.<br />
(3) Newspaper advertising Rs.5,000 x 100 advertisements = 15.00 lakhs.<br />
Subsection – B.10.6: Other Activities<br />
Awards for Journalists<br />
Award will be honored to journalists for best press articles and stories on 'Mother and<br />
Child Health' topic. For the award scheme, evaluation of articles will be done by expert<br />
committee, and awards will be distributed in a special function at state level. Details of the<br />
award scheme are as follows:<br />
1) Selection procedure : Rs. 2.00 lakhs<br />
2) Award distribution ceremony : Rs. 2.00 lakhs<br />
3) Pre-publicity of award scheme : Rs. 25.00 lakhs<br />
4) Prizes : Rs.00.63 lakhs<br />
(1 prize : Rs.25,000/- + 11 prize : Rs. 15,000/- + iii prize :<br />
Rs.10,000/- + IV prize : Rs.1,5000/- + V prize " Rs. 5,000/-)<br />
Award to district for best performance in IEC:<br />
Awards will be given to best three districts on performance basis in IEC. Evaluation will<br />
be done on the performance of the year 2011-12 and the sinner districts will be awarded with a<br />
momento in the same function of journalists. Therefore budget is requested only for awards. A<br />
budget of Rs. Rs.2.00 lakhs is proposed for this purpose.<br />
Exhibitions in major fairs in districts:<br />
Page | 62
In each district, exhibitions, film shows will be arranged in the major fairs where more<br />
than 1 lakh pepole gathered. 5 exhibitions will be arranged per year in each district. Thus 165<br />
exhibitions will be arranged in 33 districts.<br />
Rs.20,000 x 165 exhibitions = Rs.33.00 lakhs.<br />
Health Issues IPC<br />
Activitie<br />
s<br />
Mother child<br />
<strong>health</strong><br />
21.20 112.0<br />
0<br />
Health issue wise Media plan budget provision<br />
(Rs. In lakhs)<br />
Print Media Folk Electronic Media Community Media<br />
Books Newspa Media T.V. Radio Rallis Health Exhibitio<br />
per<br />
Melas ns Film,<br />
Advt.<br />
shows<br />
- 264.0<br />
0<br />
285.00 65.00 16.50 165.0<br />
0<br />
Page | 63<br />
Hoardin<br />
gs<br />
47.40 14.58<br />
PCPNDT - - 15.00 60.00 60.00 6.00 33.00 - - -<br />
Mass deverming<br />
and<br />
Vitamin a<br />
supplementati<br />
ons to children<br />
-<br />
5.00<br />
10.00<br />
-<br />
Epilepsy - - - - - - 3.30 3.30 - -<br />
Ayush - 25.00 - - - - - - - -<br />
5.00<br />
5.00<br />
-<br />
-<br />
-<br />
-
Activ-ity<br />
Code<br />
MAHARASHTRA<br />
IEC / BCC UNDER MESSION FLEXIPOOL PIP <strong>2012</strong>-<strong>13</strong><br />
B. 10 BUDGET SUMMERY<br />
B.10.2.1<br />
To<br />
B 10 2.4<br />
Focused<br />
areas for IEC<br />
1)Mother <strong>health</strong><br />
2)Child care,<br />
3) Institutional<br />
delivery,<br />
4)Breast<br />
Feeding<br />
5)Immunization<br />
6)PCPNDT<br />
7)NSV<br />
8)Spacing<br />
9)Adolescent<br />
Health<br />
10)Age at<br />
Marriage<br />
Other RCH<br />
issues<br />
Importance of<br />
Girl Child<br />
Small family<br />
norm<br />
B 10.4 1)Mother <strong>health</strong><br />
2)Child care,<br />
3)<br />
Immunization<br />
4)NSV<br />
5)Spacing<br />
6)Adolescent<br />
Health<br />
7)Blindness<br />
8)Heart<br />
problems<br />
9) Mental<br />
Health<br />
10)Leprosy<br />
11)T.B.<br />
12)HIV Aids<br />
<strong>13</strong>)Any <strong>health</strong><br />
problem.<br />
IEC for<br />
whom<br />
Target<br />
groups<br />
Service<br />
Providers<br />
General<br />
community<br />
General<br />
community<br />
General<br />
community<br />
Mode of<br />
Awareness<br />
Media<br />
Inter personal<br />
communicatio<br />
n<br />
Methods Expected<br />
Budget<br />
(Rs In<br />
lakhs)<br />
A – DISTRICT LEVEL ACTIVITIES<br />
Community<br />
media - Folk<br />
Art:<br />
Community<br />
media -<br />
Rallies:<br />
Community<br />
media<br />
For effective IPC<br />
counseling and<br />
interactive sessions<br />
with ASHAs, ANMs,<br />
and Anganwadi<br />
Workers, (block and<br />
district level)<br />
workshops has<br />
been proposed.<br />
358 workshops at<br />
block level (@Rs.<br />
5000) and 33<br />
workshops at district<br />
level (@Rs. 10000)<br />
For creating<br />
awareness<br />
regarding various<br />
issues of RCH, the<br />
activities like folk<br />
art, Rallies, Street<br />
plays have been<br />
proposed. 200 folk<br />
programmes @Rs.<br />
4000 will be<br />
organized in each<br />
district.<br />
On occasion of<br />
<strong>health</strong> days, fairs<br />
and campaigns, 5<br />
rallies in each<br />
district @ Rs. 10000<br />
will be organized.<br />
For mass<br />
awareness<br />
regarding various<br />
<strong>health</strong><br />
programmes,<br />
<strong>health</strong> mela is the<br />
best opportunity.<br />
We can provide<br />
<strong>health</strong> check-up<br />
services &<br />
awareness<br />
campaign in the<br />
same mela. One<br />
<strong>health</strong> mela in<br />
each district will be<br />
organized. Each<br />
Mela will be for the<br />
period of 1 day at<br />
Sub district<br />
hospital. The<br />
21.20<br />
264 .00<br />
Implemen<br />
tation<br />
Period<br />
June<br />
<strong>2012</strong> to<br />
Sept 20<strong>13</strong><br />
Sep <strong>2012</strong><br />
to Dec<br />
<strong>2012</strong><br />
16.50 June <strong>2012</strong><br />
to March<br />
20<strong>13</strong><br />
165.00<br />
Sept.<strong>2012</strong><br />
to Feb.,<br />
20<strong>13</strong><br />
Outcome<br />
Workshops will<br />
help to increase<br />
IPC skills of<br />
ASHAs, ANMs<br />
& Anganwadi<br />
workers to<br />
communicate<br />
messages<br />
effectively<br />
amongs<br />
womens group<br />
& community.<br />
Acceptance of<br />
<strong>health</strong> services<br />
by community<br />
will be<br />
increased.<br />
To create<br />
awareness in<br />
community<br />
People can get<br />
all the <strong>health</strong><br />
check-ups &<br />
IEC under one<br />
umbrella as<br />
well as they will<br />
get proper<br />
treatment.<br />
Page | 64
Activ-ity<br />
Code<br />
Focused<br />
areas for IEC<br />
IEC for<br />
whom<br />
Target<br />
groups<br />
B 10.6 Malnutrition General<br />
community for<br />
Tribal areas<br />
Mode of<br />
Awareness<br />
Media<br />
Mass Media<br />
Awareness<br />
through<br />
government<br />
approved<br />
Audio Visual<br />
Van agency<br />
Methods Expected<br />
Budget<br />
(Rs In<br />
facilities for <strong>health</strong><br />
check-ups and<br />
diagnostic purpose<br />
will be provided to<br />
community by<br />
specialists. Health<br />
exhibitions, film<br />
shows,folk<br />
programmes will be<br />
arranged in the<br />
mela. IEC material<br />
will be distributed<br />
to the<br />
beneficiaries. Prepublicity<br />
of the<br />
camp through<br />
banners,<br />
posters,Davandi,<br />
Radio publicity will<br />
be done. Transport<br />
of public to the<br />
venue of Health<br />
mela,<br />
Remuneration of<br />
Private Specialist<br />
doctors. Grant of<br />
Rs 5.00 lakh will be<br />
allotted per Mela.<br />
(Rs. 4.00 lakh will<br />
be placed at the<br />
disposal of Civil<br />
Surgeon & Rs.<br />
1.00 lakh will be<br />
kept with IEC<br />
Bureau.<br />
Rs. 5.00 lakh X 33<br />
districts<br />
For the sensitization<br />
in 3 tribal districts<br />
(Amarawati, Dhule<br />
& Thane) about<br />
malnutrition, IEC<br />
through Audio<br />
Visual Van is a very<br />
effective medium.<br />
Government<br />
approved Audio<br />
Visual Van agency<br />
will be selected for<br />
this purpose. 200<br />
villages in each<br />
district X 12<br />
programmes X Rs.<br />
2000/- per<br />
programme =<br />
Rs 4.80 lakhs for<br />
one district X 3 dist.<br />
lakhs)<br />
14.40<br />
Implemen<br />
tation<br />
Period<br />
July <strong>2012</strong><br />
to Aug<br />
<strong>2012</strong><br />
Outcome<br />
Awareness will<br />
be created in<br />
tribal people<br />
and the <strong>health</strong><br />
services will be<br />
accepted by<br />
them.<br />
RCH and General In each district, 5 exhibitions will be 33.00 Aug <strong>2012</strong> ____”____<br />
Page | 65
Activ-ity<br />
Code<br />
Focused<br />
areas for IEC<br />
other<br />
communicabl<br />
e & non<br />
communicabl<br />
e diseases.<br />
Malnutrition,<br />
sickle cell<br />
and RCH<br />
issues.<br />
IEC for<br />
whom<br />
Target<br />
groups<br />
Mode of<br />
Awareness<br />
Media<br />
community exhibitions, film<br />
shows will be<br />
arranged in the<br />
major fairs<br />
where more<br />
than 1 lakh<br />
people<br />
gathered.<br />
Service<br />
Providers &<br />
community<br />
Service<br />
Providers &<br />
community<br />
PCPNDT General<br />
Community<br />
Exhibition set &<br />
computers for<br />
district media<br />
units<br />
Funds will be<br />
given to 15<br />
tribal districts<br />
for printing of<br />
IEC material in<br />
local tribal<br />
language<br />
For<br />
organization of<br />
awareness<br />
campaign and<br />
preparation of<br />
floats on the<br />
occasion of<br />
26 th January<br />
20<strong>13</strong><br />
POL to IEC<br />
Van at<br />
districts/Hiring<br />
of IEC Van<br />
Methods Expected<br />
Budget<br />
(Rs In<br />
arranged per year.<br />
in each district.<br />
Thus 165<br />
exhibitions will be<br />
arranged in 33<br />
districts.<br />
Rs. 20,000 X 165<br />
exhibitions<br />
33 districts X Rs.<br />
2.00 lakhs per<br />
district<br />
15 districts X Rs.<br />
1.00 lakhs<br />
Rs. 1.00 lakh X 33<br />
districts<br />
Rs. 1.00 lakhs X 33<br />
Districtd<br />
lakhs)<br />
Implemen<br />
tation<br />
Period<br />
to March<br />
20<strong>13</strong><br />
66.00 June <strong>2012</strong><br />
to Oct<br />
<strong>2012</strong><br />
15.00 Aug <strong>2012</strong><br />
to Dec<br />
<strong>2012</strong><br />
33.00 July <strong>2012</strong><br />
to March<br />
20<strong>13</strong><br />
33.00<br />
A District level Total 661.10<br />
Note:-State level activities continued on next page<br />
STATE LEVEL ACTIVITIES<br />
Outcome<br />
District IEC cell<br />
will be strength<br />
The IEC<br />
material in local<br />
language will<br />
help to<br />
understand the<br />
messages<br />
Help to create<br />
awareness in<br />
community and<br />
the birth rate of<br />
girl child will be<br />
increased.<br />
Page | 66
Activ-ity<br />
Code<br />
B.10.5<br />
Focused<br />
areas for IEC<br />
PCPNDT<br />
Mother and<br />
Child care,<br />
Immunization,<br />
Breast<br />
IEC for<br />
whom<br />
Target<br />
groups<br />
General<br />
Community<br />
General<br />
Community<br />
Mode of<br />
Awareness<br />
Media<br />
1) Telecastin<br />
g of TV<br />
Spot<br />
2) Broadcast<br />
ing of<br />
Radio<br />
Jingle<br />
3) Newspap<br />
er<br />
Publicity<br />
4) Messages<br />
through<br />
folk art<br />
and<br />
drama<br />
Electronic<br />
Media<br />
Methods Expected<br />
Budget<br />
(Rs In<br />
For creating<br />
awareness, the<br />
media like T.V.,<br />
Radio, Newspaper,<br />
hoardings, Rallies,<br />
pictorial floats,<br />
banners, posters,<br />
exhibitions, folk<br />
programme will be<br />
utilized.<br />
(1) Telecasting of<br />
TV spots :<br />
Rs. 60,000/-<br />
per telecast x<br />
100 telecasts =<br />
Rs 60.00 lakhs<br />
(2) Broadcasting<br />
of Radio<br />
Jingles : Rs.<br />
<strong>13</strong>,000/- per<br />
broadcast x 46<br />
broadcasts =<br />
Rs. 06.00 lakhs<br />
(3) Newspaper<br />
advertising : Rs<br />
15,000 X 100<br />
advertisements<br />
= Rs. 15.00<br />
lakhs<br />
(4) Messages<br />
through folk art<br />
and drama :<br />
Programmes<br />
will be taken in<br />
the selected 20<br />
districts where<br />
the girl sex<br />
ratio is less :<br />
20 districts X 5<br />
programmes X<br />
Rs. 50,000 per<br />
programme =<br />
Rs. 50.00 lakhs<br />
For Selection<br />
procedure of<br />
Folk Media<br />
groups = Rs.<br />
10.00 lakhs<br />
: Total 60.00<br />
lakhs<br />
Telecasting of TV<br />
spots : Rs. 60,000/-<br />
per telecast x 475<br />
telecasts = Rs.<br />
lakhs)<br />
141.00<br />
350.00<br />
Implemen<br />
tation<br />
Period<br />
14 th Nov<br />
<strong>2012</strong> to<br />
14 th Dec<br />
<strong>2012</strong><br />
June <strong>2012</strong><br />
to Dec<br />
<strong>2012</strong><br />
Outcome<br />
Awareness will<br />
help to increase<br />
the sex ratio of<br />
girl child<br />
After creating<br />
awareness,<br />
more<br />
beneficiaries<br />
Page | 67
Activ-ity<br />
Code<br />
Focused<br />
areas for IEC<br />
Feeding,<br />
PCPNDT,<br />
NSV, JSSK.<br />
JSY,<br />
Institutional<br />
delivery,<br />
referral<br />
services,<br />
Nutrition,<br />
Spacing<br />
methods,<br />
Care at<br />
pregnancy<br />
Mother &<br />
Child Health.<br />
Award to<br />
district for<br />
best<br />
performance<br />
in IEC :<br />
IEC for<br />
whom<br />
Target<br />
groups<br />
Media<br />
Persons<br />
Service<br />
Providers<br />
Mode of<br />
Awareness<br />
Media<br />
Award will be<br />
honored to<br />
journalists for<br />
best press<br />
articles and<br />
stories on<br />
'Mother and<br />
Child Health'<br />
topic. For the<br />
award scheme,<br />
evaluation of<br />
articles will be<br />
done by expert<br />
committee. and<br />
awards will be<br />
distributed in a<br />
special function<br />
at state level.<br />
Awards will be<br />
given to best<br />
three districts<br />
on<br />
performance<br />
basis in IEC.<br />
Evaluation will<br />
be done on the<br />
performance of<br />
the year 2011-<br />
12 and the<br />
winner districts<br />
will be awarded<br />
with a<br />
momento in a<br />
Methods Expected<br />
Budget<br />
(Rs In<br />
lakhs)<br />
285.00 lakhs<br />
Broadcasting of<br />
Radio Jingles : Rs.<br />
<strong>13</strong>,000/- per<br />
broadcast x 500<br />
broadcasts =<br />
Rs.65.00 lakhs<br />
1) Selection<br />
procedure : Rs.<br />
2.00 lakhs<br />
2) Award<br />
distribution<br />
ceremony : Rs.<br />
2.00 lakhs<br />
3) Pre-publicity of<br />
award scheme<br />
: Rs. 25.00<br />
lakhs<br />
4) Prizes : Rs.<br />
00.63 lakhs<br />
( I prize : Rs.<br />
25,000/- + II<br />
prize : Rs.<br />
15,000/- + III<br />
prize: Rs.<br />
10,000/- + IV<br />
prize : Rs.<br />
7,500/- + V<br />
prize : Rs.<br />
5,000/-)<br />
1) Selection<br />
Procedure<br />
2) Special<br />
Function<br />
3) Memento<br />
29.63<br />
Implemen<br />
tation<br />
Period<br />
2.00 Nov <strong>2012</strong><br />
to Mar<br />
20<strong>13</strong><br />
Outcome<br />
will accept the<br />
<strong>health</strong> services.<br />
Jan 20<strong>13</strong> The award<br />
scheme will<br />
help to get<br />
positive<br />
feedback from<br />
press people.<br />
Due to<br />
appreciation,<br />
district IEC<br />
team will give<br />
better results.<br />
Page | 68
Activ-ity<br />
Code<br />
Focused<br />
areas for IEC<br />
RCH & other<br />
<strong>health</strong> issues.<br />
RCH & other<br />
<strong>health</strong> issues.<br />
IEC for<br />
whom<br />
Target<br />
groups<br />
Service<br />
Providers,<br />
Community<br />
Leaders<br />
(Sarpanch)<br />
General<br />
Community<br />
Ayush Service<br />
Providers &<br />
Community<br />
Mode of<br />
Awareness<br />
Media<br />
special function<br />
Hiring of<br />
Advertisement<br />
agency.<br />
Hiring of IEC<br />
consultant<br />
Development<br />
of Information<br />
centre at IEC<br />
Bureau<br />
Printing of<br />
Maharashtra<br />
Arogya Patrika<br />
Magazine and<br />
to provide it to<br />
Sarpanch,<br />
ASHAs, all<br />
<strong>health</strong><br />
institutes in the<br />
state<br />
Charges for<br />
transportation<br />
and<br />
redesigning of<br />
Audio Visual<br />
Van 'Parivartan<br />
Express'<br />
Designing of<br />
Float<br />
Printing of<br />
book<br />
Methods Expected<br />
Budget<br />
(Rs In<br />
lakhs)<br />
Rs. 2.00 lakhs per<br />
month X 6 months<br />
Implemen<br />
tation<br />
Period<br />
12.00 July <strong>2012</strong><br />
to Mar<br />
20<strong>13</strong><br />
--- 3.50 June <strong>2012</strong><br />
Purchase of<br />
exhibition panels,<br />
maintenance of<br />
exhibition sets,<br />
Artwork, workshops,<br />
and other creative<br />
work, Flex on<br />
existing hoardings<br />
97,000 copies per<br />
month X 10 months<br />
1) 9,70,000<br />
copies @<br />
X Rs. 10<br />
= Rs.97<br />
lakh.<br />
IEC Bureau<br />
organizing<br />
exhibitions in<br />
awareness<br />
campaign Health<br />
Melas and other<br />
occasions. The<br />
Parivartan Express<br />
Van is used for this<br />
purpose only.<br />
Innovative float will<br />
be designed in<br />
State level Republic<br />
day function.<br />
Information<br />
regarding Ayurved,<br />
Homeopathy, Unani<br />
and Yoga will be<br />
given with<br />
appropriate pictures<br />
in the book. It will<br />
be made available<br />
in 23 district<br />
hospitals and 236<br />
SDH & RH where<br />
Ayush Service is<br />
available.<br />
Size – A4<br />
Pages – 48 + 4<br />
Paper Maplitho 60<br />
GSM<br />
Cover – Art paper<br />
120 GSM<br />
Printing – Four<br />
14.50 May <strong>2012</strong><br />
to March<br />
<strong>2012</strong><br />
97.00 July <strong>2012</strong><br />
to Mar<br />
20<strong>13</strong><br />
5.00 June <strong>2012</strong><br />
to March<br />
20<strong>13</strong><br />
6.00 26 th Jan<br />
20<strong>13</strong><br />
25.00 Oct. <strong>2012</strong><br />
to Feb.,<br />
20<strong>13</strong><br />
Outcome<br />
To create<br />
awareness in<br />
community<br />
To create<br />
awareness<br />
regarding<br />
Ayush Services<br />
Page | 69
Activ-ity<br />
Code<br />
Focused<br />
areas for IEC<br />
IEC for<br />
whom<br />
Target<br />
groups<br />
Mode of<br />
Awareness<br />
Media<br />
Ayush Community Information<br />
boards<br />
regarding<br />
Ayush services<br />
1) PCPNDT<br />
2)Mother and<br />
Child Health<br />
3)Immunization<br />
4)Breast<br />
Feeding<br />
5)NSV<br />
6) Spacing<br />
Other RCH<br />
issues<br />
All Health<br />
Issues<br />
Mass de-<br />
Worming and<br />
vitamin A<br />
supplementati<br />
on to Children<br />
General<br />
community<br />
Service<br />
Providers &<br />
officers<br />
Community<br />
media –<br />
Messages<br />
through<br />
hordings<br />
National &<br />
Regional<br />
Workshops<br />
Methods Expected<br />
Budget<br />
(Rs In<br />
colour<br />
Copies - 2 lakhs<br />
Expected cost - Rs.<br />
25 per copy Rs. 25<br />
lakh.<br />
Information boards<br />
will be displayed in<br />
the premises of 23<br />
District Hospitals<br />
and 236 SDH & RH.<br />
Boards will be put<br />
up by hospital<br />
authorities and the<br />
funds will be provide<br />
to 23 Civil<br />
Surgeons.<br />
Rs. 50,000 x 23<br />
C.S.<br />
= Rs. 11.50<br />
Flex Messages will<br />
be displayed on 162<br />
hordings owned by<br />
<strong>health</strong> department<br />
in the premises of<br />
<strong>health</strong> institutes in<br />
the States<br />
Hoardings size : 20<br />
feet X 10 feet<br />
No of hordings : 162<br />
Each hording cost<br />
Rs. 9000/- for three<br />
quarters<br />
Rs. 9000 X 162 =<br />
14.58 lakh<br />
Organization,<br />
Travelling and other<br />
related cost for<br />
<strong>national</strong> and<br />
regional workshops<br />
lakhs)<br />
B State Total 793.31<br />
Parents Com Biannual mass de 25.00<br />
munit worming and<br />
y vitamin A<br />
Medi supplementation<br />
a campaign will be<br />
organized in June &<br />
December. For<br />
second phase<br />
awareness<br />
campaign will be<br />
organized in the<br />
month of Nov. <strong>2012</strong><br />
following IEC<br />
activities will be<br />
implemented.<br />
1) Newspaper<br />
Advertisement<br />
Rs. 10.00 lakh<br />
2) T.V.Scrolling<br />
Implemen<br />
tation<br />
Period<br />
11.50 Oct, <strong>2012</strong><br />
to Feb.,<br />
20<strong>13</strong><br />
14.58 June <strong>2012</strong><br />
To March<br />
20<strong>13</strong><br />
50.00 June <strong>2012</strong><br />
To March<br />
20<strong>13</strong><br />
Outcome<br />
For creating<br />
awareness<br />
-<br />
Page | 70
Activ-ity<br />
Code<br />
Focused<br />
areas for IEC<br />
IEC for<br />
whom<br />
Target<br />
groups<br />
Mode of<br />
Awareness<br />
Media<br />
Epilepsy Parents Community<br />
Media<br />
A District level: 661.10 + B State level<br />
: 793.31<br />
Methods Expected<br />
Budget<br />
(Rs In<br />
Messages 5.00<br />
lakh<br />
3) Broadcasting<br />
of Radio<br />
Jingles 5.00<br />
lakh<br />
4) Printing of<br />
Posters 5.00<br />
lakh<br />
Organization of<br />
Epilepsy day on 17th Nov. Event will be<br />
organized at every<br />
district level place.<br />
33 Events @ Rs.<br />
10,000<br />
Organization of<br />
Epilepsy and Other<br />
neurological<br />
disease camps.<br />
33 Camps @<br />
Rs.10,000/-<br />
lakhs)<br />
Total of A & B 1454.41<br />
SUBSECTION – B.10.7 : REGIONAL / NATIONAL WORKSHOPS<br />
Approved.<br />
SUBSECTION – B.10.8 : AWARENESS CAMPAIGN<br />
Not approved. Accepted.<br />
SUBSECTION – B.10.9 : PRINTING OF FORMATS<br />
Implemen<br />
tation<br />
Period<br />
3.30 Nov.<strong>2012</strong><br />
3.30 Sept <strong>2012</strong><br />
To<br />
March<br />
20<strong>13</strong><br />
As per GoI instructions, all the printing in the PIP is submitted at one place. There are six<br />
major printing activities in the PIP as mentioned below:<br />
Sr FMR<br />
Table – Printing required for various activities – <strong>2012</strong>-<strong>13</strong><br />
Name of<br />
Activities<br />
1 B.16.1.3 Printing of R-<br />
3 & R-4<br />
Registers<br />
Budget<br />
Proposed<br />
Budget<br />
Approved<br />
by NPCC<br />
Resubmitted<br />
for<br />
Approval<br />
Outcome<br />
Rs. In Lakhs<br />
Remark<br />
18 0 18 Printing of registers for<br />
FW cases records<br />
Page | 71
Sr FMR<br />
Name of<br />
Activities<br />
2 B.8 Panchayat<br />
Raj initiative<br />
3 B.10 IEC/BCC<br />
4 B.15.3 Monitoring<br />
&Evaluation<br />
5 B.15.3.3 Mother<br />
&Child<br />
Tracking<br />
System<br />
6 B.16 Procurement<br />
for ARSH<br />
Budget<br />
Proposed<br />
Budget<br />
Approved<br />
by NPCC<br />
Resubmitted<br />
for<br />
Approval<br />
35.3 35.3 0<br />
1<strong>13</strong> 28.25 84.75<br />
53.2 53.2 0<br />
115.06 115.06 0<br />
7.15 7.15 0<br />
7 B.16.2 Procurement<br />
of Drugs &<br />
supplies 4.72 4.72 0<br />
Total 346.43 243.68 102.75<br />
Remark<br />
B.8.1 ( Consitution &<br />
Orientation of<br />
Community Leader &<br />
VHSC,SHC,PHC,CHC)<br />
Preparation of Traninig<br />
Material<br />
B.10.6 Printing of<br />
Maharashtra Arogya<br />
Patrika Magzine , 8<br />
Tribal district for<br />
printing of IEC material<br />
in local language<br />
Other Expenses<br />
(Printing revised<br />
Formats MIS,<br />
shc,PHC,RH,DH,Traning)<br />
Printing & Supply Of<br />
RCH Registers to each<br />
village & <strong>health</strong><br />
facilities in the State<br />
Printing of Training<br />
modules for<br />
MO,ANMs/LHVs&ASHA,<br />
new record keeping<br />
regist er& formats<br />
Printing of consent<br />
forms & laboratory<br />
forms each for testing<br />
of pregnant mothers.<br />
Out of the above mentioned six activities, budget is provided for all the activities except<br />
B.10 Printing of Arogya Patrika etc. Therefore it is requestd to approve B.10 as proposed.<br />
Budget requestd is Rs. 84.75 Lakh.<br />
Approval accepted as per ROP<br />
SECTION - B.11 : MOBILE MEDICAL UNITS<br />
Page | 72
SECTION - B.12 : REFERRAL TRANSPORT & MOBILITY SUPPORT<br />
Transport facility is required to transfer emergency patients, attending epidemics and<br />
transferring serious patients, attending accidents and natural calamity, etc. and also to<br />
transfer routine patients, support to implement the activities related to National Health<br />
Programs and visit to ASHA, ANM and <strong>health</strong> institutions for supportive supervision.<br />
Plan of action <strong>2012</strong>-<strong>13</strong><br />
Approach for referral transport will be as follows:<br />
• On highways and at block HQ, EMS ambulance will be available for all the<br />
emergencies. One ambulance will be deployed for 1.0 Lakh population in <strong>rural</strong> areas<br />
and 2.0 Lakh populations in urban areas.<br />
• EMS ambulance will pick up obstratic emergencies but will not transport pregnant<br />
women not in emergency.<br />
• Regular Hospital ambulance will transport pregnant women willing to come for<br />
delivery and also other patients who are not in emergency but need transportation.<br />
• PHC vehicle is called as ambulance cum supervisory vehicle as this vehicle is used for<br />
transportation of patients, to check anganwadies, to attend epidemics and also to<br />
supervise the RCH / DCP work of <strong>health</strong> workers and nurses.<br />
• Support to existing ambulances in the form of repairs, POL and hiring driver if<br />
required if the state government grants are not sufficient due to higher load in<br />
<strong>health</strong> institution. This budget will be provided to RKS of the institution. This will<br />
ensure 24 hours availability of ambulance<br />
• Provision of ambulances wherever not available.<br />
• Review of all supervisory vehicles available in state and provision of supervisory<br />
vehicles where ever not available.<br />
As per discussion during NPCC meeting and 6-8 June <strong>2012</strong> meeting, total budget of referral<br />
transport and mobility is put in one chapter and submitted to GoI as follows:<br />
SUBSECTION – B.12.1 : REFERRAL TRANSPORT OF PATIENTS<br />
Referral transport of patients is at two levels. First level is Basic Ambulance Services. This<br />
level if of ambulance infrastructure of PHCs and Hospitals. This is required for quick<br />
transport of patients from home to hospital and back or from hospital to hospital for<br />
referral service. This is available for non-emergency patients / beneficiaries of National<br />
Health Programs such as Mothers for delivery, FW patients, cataract patients, <strong>health</strong> camp<br />
patients etc. These ambulances will be fitted with tracking system and will be controlled by<br />
District RT Cell by universal telephone no. 102.<br />
Second level of referral transport system is advanced and is called as Pre Hospital<br />
Emergency Response (Ambulance) scheme. In this scheme, one ambulance per 1 lakh<br />
Page | 73
population in <strong>rural</strong> areas and per 2 lakh population in urban areas is provided. This<br />
ambulance is used only for emergency purpose including road accidents and also emergency<br />
referral of pregnant or delivery patents or neonates. This system will be controlled by State<br />
level control room under telephone no. 108.<br />
B.12.1.1 : REFERRAL TRANSPORT BY BASIC AMBULANCES SERVICES<br />
About 85% PHCs/Rural Hospitals and all District Hospitals have ambulances. However many<br />
of the presently available ambulances are off road as they require repairs. It is proposed to<br />
provide funds for repairs, POL and driver salary whichever is deficit, to these institutions<br />
through RKS with condition that repairs to be carried out only by authorized dealers.<br />
This is for patients transport system. Transport will be from home to hospital to home or<br />
hospital to hospital. Transport will be of emergency patients, mothers for delivery in<br />
emergency or without emergency and transport of beneficiaries of National Disease Control<br />
Programs.<br />
Budget is required for procurement of new ambulances to PHCs and Hospitals where they<br />
are not available and also for additional repairs and POL grants to PHC and Hospital<br />
ambulances.<br />
Plan of action <strong>2012</strong>-<strong>13</strong><br />
Approach for mobility support will be as follows:<br />
• Support to existing ambulances in the form of repairs, POL and hiring driver if<br />
required if the state government grants are not sufficient due to higher load in<br />
<strong>health</strong> institution. This budget will be provided to RKS of the institution. This will<br />
ensure 24 hours availability of ambulance<br />
• Provision of ambulances wherever not available.<br />
Budget requirement <strong>2012</strong>-<strong>13</strong><br />
Budget proposed for providing vehicles to all the <strong>health</strong> institutions is as follows:<br />
Table – : Budget required for mobility support– <strong>2012</strong>-<strong>13</strong><br />
Sr Institution<br />
No. of<br />
vehicles<br />
Unit cost<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
A POL for ambulances<br />
1 PHC Ambulances 1743 0.2 348.6<br />
2 RH/SDH Ambulances 347 0.3 104.1<br />
3 DH Ambulances 96 0.5 48<br />
Total 2186 500.7<br />
B<br />
Repairs and procurement of tyres, batteries,<br />
etc<br />
1 PHC Ambulances 1235 0.08 98.8<br />
2 RH/SDH Ambulances 286 0.14 40.04<br />
3 DH Ambulances 42 0.14 5.88<br />
Total 1563 144.72<br />
Page | 74
Sr Institution<br />
C<br />
Procurement of new ambulances for Basic<br />
Ambulance Services<br />
No. of<br />
vehicles<br />
Unit cost<br />
Budget<br />
required<br />
1 PHC Ambulances (TATA SUMO) 196 5.2 1019.2<br />
2 Hospital Ambulance (Force) 84 7.3 6<strong>13</strong>.2<br />
Total 280 1632.4<br />
Grand Total 2277.82<br />
B.12.1.2 : PRE HOSPITAL EMERGENCY MEDICAL RESPONSE (AMBULANCE) SERVICES (EMS)<br />
Major part of approvals mentioned in ROP is acceptable. Only two important sub<strong>mission</strong>s<br />
are to be considered.<br />
1. Posts of Medical Officers and consultants are continued since 2011-12 and all are in<br />
position. However ‘new post not approved’ is written in remarks column against<br />
these posts. As this activity will be starting in next three months, all these posts are<br />
required. Therefore, it is requested to continue all existing posts. Salary of these<br />
posts will be paid from existing budget only.<br />
2. GoI has approved budget of Rs. 60.76 Crores as against 1<strong>13</strong>.03 Crores. Approved<br />
budget is for 50 ALS and 150 BLS ambulances. This need not be changed now.<br />
Presently Hon. High Court has issued order in favor of SHS Maharashtra. However<br />
has given time for complainants to file appeal. Considering all this, if the agency fixed<br />
for provision of ambulance is able to provide more number of ambulances, then<br />
Maharashtra may require more budgets. That may be approved from cushion<br />
available to state.<br />
SUBSECTION – B.12.2 : MOBILITY SUPPORT FOR PROGRAM MANAGEMENT<br />
As per discussions during 6-8 June <strong>2012</strong> meeting, mobility support includes support<br />
provided to block, district, regional and state level offices for supervision of work,<br />
verification of data, checking of work done and for visits during emergencies. Mobility<br />
support required for implementation of programs is requested from the program only so it<br />
is not added in this chapter.<br />
Some of the officers have been provided with hired vehicles. However, State Govt has<br />
approved drivers and POL for these posts which remain unutilized. Therefore it is proposed<br />
to procure cheapest vehicles (Standard Indogo) available on RC to these officers. One<br />
vehicle is purchased in one and half year cost of hiring. This will save budget on mobility<br />
support.<br />
Page | 75
As mentioned above, officers from block to state level require mobility support for<br />
monitoring work. Names and number of officers required for this work is mentioned in table<br />
below:<br />
Sr Level<br />
Table – Expected visits of officers in NRHM<br />
Names of Officers<br />
included for monitoring<br />
visit<br />
No in<br />
state<br />
No. of<br />
visits<br />
expected<br />
in one<br />
month/<br />
officer<br />
No. of<br />
visits<br />
expected<br />
in one<br />
year<br />
Total<br />
Expected<br />
visits in one<br />
year<br />
A Block Block Health Officer 353 12 144 50832<br />
Block Accountant 353 4 48 16944<br />
Medical Suprentendent 433 4 48 20784<br />
Total 1<strong>13</strong>9 88560<br />
B District Dist Health Officer 33 8 96 3168<br />
Civil Surgeon 33 8 96 3168<br />
Dist RCH Officer 33 12 144 4752<br />
RMO (O) 33 12 144 4752<br />
MO DTT 33 12 144 4752<br />
Stastical Officer 33 12 144 4752<br />
DPM 33 8 96 3168<br />
DAM 33 8 96 3168<br />
M & E Officer 33 12 144 4752<br />
IPHS Coordinator 33 12 144 4752<br />
Dist Senior Supervisor 72 12 144 10368<br />
SH Coordinator 33 12 144 4752<br />
Deputy Engineer 35 16 192 6720<br />
ASHA Coordinator 33 12 144 4752<br />
Total 503 67776<br />
C Circle Deputy Director 8 6 72 576<br />
Assistant Director 8 12 144 1152<br />
Circle Project Manager 8 8 96 768<br />
Principal HFWTC 7 8 96 672<br />
Vice Principal HFWTC 7 12 144 1008<br />
HEMR Unit 8 16 192 1536<br />
Public Health Specialist 8 16 192 1536<br />
Ex. Engg (IDW) 8 16 192 1536<br />
Total 62 8784<br />
D State Add. / Joint Directors<br />
(Bureau Chiefs)<br />
9 8 96 864<br />
Deputy Directors of DCPs 6 8 96 576<br />
Assistant Directors of<br />
RCH and MFP<br />
9 8 96 864<br />
Principal and faculty<br />
SIHFW<br />
4 6 72 288<br />
Page | 76
Sr Level<br />
Names of Officers<br />
included for monitoring<br />
visit<br />
No in<br />
state<br />
No. of<br />
visits<br />
expected<br />
in one<br />
month/<br />
officer<br />
No. of<br />
visits<br />
expected<br />
in one<br />
year<br />
Total<br />
Expected<br />
visits in one<br />
year<br />
Supt Engineer 1 12 144 144<br />
Senior Consultants (EMS,<br />
PPP, IPHS, RCH, Trg, etc)<br />
Public Health Specialist<br />
8 8 96 768<br />
Program Officers 18 8 96 1728<br />
Total 55 5232<br />
Grand Total 1759 170352<br />
Budget required for these officers is calculated considering the area they are covering for<br />
supervision, TA/DA of the post, mode of travel (public transport, hired vehicle, train with<br />
class and air) allowed to them as per Governing Body decision.<br />
Conditions are being put on officers for using the Mobility Support budget. These conditions<br />
will be as follows :<br />
• After each tour, the person touring should give brief actionable points to controlling<br />
authority<br />
• Action taken points to be submitted within one month after the communication of<br />
actionable points. This will be responsibility of the concerned touring officer, staff.<br />
• There should be pre-decided outcome of the tour which will be examined after one<br />
month of tour by the touring officer.<br />
Accordingly budget required for mobility support is as follows:<br />
Sr Category of Officers<br />
Table – One year Budget requirement for Mobility support<br />
Unit rate<br />
(Per day)<br />
No. of<br />
torus in<br />
year<br />
Budget<br />
required<br />
Rs. In Lakhs<br />
Remarks<br />
A Block Level<br />
1 THO + MS 0.008 71616 572.928<br />
Hired veh/POL in block<br />
only<br />
2 Others 0.002 16944 33.888 Public Transport<br />
Total 88560 606.816<br />
B District Level<br />
1 Dist Senior Officers 0.015 15840 237.6 Dist tour / hired veh/POL<br />
2 Dist Middle level officers 0.012 9504 114.048 Dist tour / hired veh/POL<br />
Page | 77
Sr Category of Officers<br />
Unit rate<br />
(Per day)<br />
No. of<br />
torus in<br />
year<br />
Budget<br />
required<br />
Remarks<br />
3 Senior contractual staff 0.01 15840 158.4 Dist tour / hired veh/POL<br />
4 Other staff 0.03 26592 797.76 Public transport<br />
Total 67776 <strong>13</strong>07.808 0<br />
C Circle<br />
1 Deputy Director 0.04 576 23.04 Regional / state tours<br />
2 Senior Offices 0.024 3600 86.4 POL/hired veh<br />
3 Others 0.003 4608 <strong>13</strong>.824 Public Transport<br />
Total 8784 123.264 0<br />
D State<br />
1 Bureau Chiefs 0.08 864 69.12 State tour, Air travel<br />
2 Other senior officers 0.04 2640 105.6<br />
3 Other staff 0.08 1728 <strong>13</strong>8.24 Public / hired<br />
Total 5232 312.96 0<br />
Grand Total 170352 2350.848 0<br />
GoI has approved 25% budget for some activities in approval. Total budget already<br />
approved is Rs. 122.53 Lakh. In addition to this, new guideliens will take another one month<br />
for implementation. Considering this, budget reqested is as follows:<br />
Table – Budget required for Mobility support – <strong>2012</strong>-<strong>13</strong><br />
Sr Category of Officers<br />
One year budget<br />
requirement<br />
Rs. In Lakhs<br />
Budget for<br />
<strong>2012</strong>-<strong>13</strong><br />
A Block Level<br />
1 THO + MS 572.93 401.05<br />
2 Others 33.89 23.72<br />
Total 606.82 424.77<br />
B District Level 0.00<br />
1 Dist Senior Officers 237.60 166.32<br />
2 Dist Middle level officers 114.05 79.83<br />
3 Senior contractual staff 158.40 110.88<br />
4 Other staff 797.76 558.43<br />
Total <strong>13</strong>07.81 915.47<br />
C Circle 0.00<br />
1 Deputy Director 23.04 16.<strong>13</strong><br />
2 Senior Offices 86.40 60.48<br />
3 Others <strong>13</strong>.82 9.68<br />
Total 123.26 86.28<br />
Page | 78
Sr Category of Officers<br />
One year budget<br />
requirement<br />
Budget for<br />
<strong>2012</strong>-<strong>13</strong><br />
D State 0.00<br />
1 Bureau Chiefs 69.12 48.38<br />
2 Other senior officers 105.60 73.92<br />
3 Other staff <strong>13</strong>8.24 96.77<br />
Total 312.96 219.07<br />
Grand Total 2350.85 1645.59<br />
SECTION - B.<strong>13</strong> : PPP/NGOs<br />
SUBSECTION - B.<strong>13</strong>.3 : NGO PROGRAM : GRANT IN AID TO NGOs<br />
Budget of Rs. 247.80 Lakh was requsted under this scheme which is approved by GoI.<br />
However, this amount is required for ongoing NGOs. Although MNGO scheme will be<br />
discontinued in next year, SNGO scheme will continue to be implemented after that.<br />
Considering this, revised budget requestd for the scheme is as follows:<br />
Budget requirement for <strong>2012</strong>-<strong>13</strong><br />
Sir Activity Proposed<br />
Table : Budget requirement for NGO Scheme<br />
No.of<br />
Units<br />
Unit cost<br />
Budget<br />
required<br />
1 MNGO SCHEME 6 15 90<br />
2<br />
3<br />
SNGO SCHEME PHASE- (Existing<br />
NGOs)<br />
SNGO SCHEME PHASE- (New<br />
NGOs) Only for Nandurbar,<br />
Gadchiroli, Nashik, Amravati,<br />
Beed, Yavatmal, Chandrapur,<br />
Bhandara, Dhule, Gondia)<br />
7 15 105<br />
16 8.5 <strong>13</strong>6<br />
4 EXTERNAL EVALUATION<br />
TRAINING TO NGOs (before &<br />
9 1 9<br />
5<br />
During the project like Baseline,<br />
data software, Writing project<br />
proposal, record keeping etc.)<br />
19 0.2 3.8<br />
6 Quarterly meeting 4 0.4 1.6<br />
7 Annual workshop 1 2 2<br />
Rs. In Lakhs<br />
Remarks<br />
Remaining<br />
payments<br />
of last year<br />
scheme<br />
Page | 79
Sir Activity Proposed<br />
No.of<br />
Units<br />
Unit cost<br />
Budget<br />
required<br />
8 Monitoring & Evaluation 19 0.6 11.4<br />
Total 358.8<br />
SECTION - B.14 : INNOVATIONS<br />
Remarks<br />
SUBSECTION : B.14.1 : ORGANIZATION OF EPILEPSY CAMPS WITH THE HELP OF EPILEPSY<br />
FOUNDATION MUMBAI<br />
Childhood diseases are very important to diagnose and treat at earliest to avoid the<br />
permanent damage to <strong>health</strong> of the child and to help him/her to have optimal scholastic<br />
performance. Many diseases which are important in childhood. School Health Program is<br />
mainly screening these children and identifying the children who require specialized care.<br />
Presently following activities under NRHM are being implemented for <strong>health</strong> of the children.<br />
1. School <strong>health</strong> program to screen the children, <strong>health</strong> education for <strong>health</strong>y living,<br />
provide treatment for minor ailments and refer to higher institutions as per<br />
requirement.<br />
2. Tribal Health Camps of specialists – Specialist care to school children of schools in<br />
tribal areas. Non-tribal children are also treated in these camps that are staying in<br />
notified tribal areas.<br />
3. Sickle cell program – children are identified at early age, counseling, treatment of<br />
crisis, immunization, etc.<br />
4. Hemophilia and thalassemia treatment – as pilot basis in few districts of state.<br />
5. Epilepsy – specialist camps for <strong>rural</strong> children<br />
As discussed in 6-8 June Meeting, other programs are dealt in corresponding activities and<br />
are sanctioned by GoI. Epilepsy program is remaining and is submitted in this chapter.<br />
Epilepsy is one of the important diseases of Public Health Importance. The prevalence of<br />
epilepsy is an average one in thousand children & also quite common in adult populations<br />
there are many new methods come for diagnosis & treatment. More than five thousand<br />
school boys are dictated suffering of from Epilepsy in school <strong>health</strong> examinations. To treat<br />
them properly & give regular follow-up, training of Pediatrician & Physician from district<br />
hospital along with the nurses is proposed.<br />
There could be many children & women suffering from Epilepsy. Stigma about this<br />
disease prevents them to great a good care & service. There are many misconceptions<br />
regarding Epilepsy in society. Considering above situation the following action is proposed<br />
during the year <strong>2012</strong>-<strong>13</strong>.<br />
• Training of Medical Officer to improve the diagnostic skill<br />
• Proper treatment to the epileptic patients by Health care provider<br />
• Regular follow-up & proper management of the patients<br />
Page | 80
• Improve the skill & Knowledge of nurses for patients care<br />
• Create awareness in society regarding Epilepsy<br />
• Organization of Epilepsy day in the state to create the awareness<br />
Budget requirement<br />
The details of the budget proposed is as follows<br />
Table – Budget requrement for Epilepsy Camps<br />
Rs. In Lakhs<br />
SR Activity Unit cost<br />
No. of.<br />
units<br />
Budget<br />
required<br />
1 Travel charges to specialists and team 1 11 11<br />
2 Staying arrangements for specialists 0.3 11 3.3<br />
3 Arrangements of camps 0.25 11 2.75<br />
4<br />
Honorarium to EEG technicians OT, PT<br />
and speech therapy technician<br />
Medicines and consumables for camps<br />
0.1 11 1.1<br />
5<br />
and for regular treatment ( Regular camp<br />
2.00 lakh and follow-up Medicine 1.00<br />
lakh)<br />
2.5 11 27.5<br />
6<br />
Diet facility to the patients (Tribal areas<br />
only)<br />
0.25 11 2.75<br />
Total 4.4 48.4<br />
B.14.2: CAPACITY BUILDING AND ORGANIZATION OF EPILEPSY DAY<br />
Budgeted under IEC/BCC<br />
B.14.3: HEALTH ADVISE CALL CENTER<br />
Approved<br />
B.14.4: AYUSH FACILITY IN WOMEN HOSPITALS<br />
Indian Systems of Medicine & Homoeopathy (ISM&H) have proven strengths of treating<br />
common and chronic diseases. With a view to make available the benefits of Ayurveda,<br />
Unani, Siddha, Yoga & Naturopathy and Homoeopathy to the public at large, so that the<br />
people can exercise their choice in accessing and specialized treatment centers of ISM&H in<br />
the Allopathic hospitals. The objectives is to build bridges across medical systems by<br />
providing general and specialized therapies of Ayurveda, Unani medicine, Siddha, Yoga &<br />
Page | 81
Naturopathy and Homeopathy for utilization as an adjunct or better alternative to<br />
conventional medical treatment.<br />
In Daga Hospital Nagpur, AYUSH facility is provided to pregnant women attending the<br />
hospitals. Women are given good response to all pathies but particularly to Yoga and<br />
Naturopathy. Considering this, it is proposed to provide AYUSH treatment to all the 11 (New<br />
and old) Women Hospitals in the State. Budget required will be as follows:<br />
Table – Budget required for AYUSH services in Women Hospitals<br />
Rs. In Lakh<br />
Sr Particulars Unit price No. of units<br />
Total<br />
budget<br />
required<br />
3 Salary of Medical Officer Yoga 0.864 11 9.504<br />
4 Salary of Medical Officer Naturopathy 0.864 11 9.504<br />
Total 19.008<br />
B.14.5: Blood Bags transportation to BSCs<br />
Public Health Hospitals in Maharshtra has 29 Blood Banks and 104 Blood Storage Units<br />
currently functional. In addition to this, establishment of Blood Storage Unit is under<br />
process in 87 hosptials. As per FDA Rules, blood is collected and tested at Blood Bank. Each<br />
of the Blood Storage Unit is attached to nearby Blood Bank and the test blood bags of each<br />
group (2/group) are kept at Blood Storage Units for use. Plain Blood bags has 35 days expiry<br />
and Blood Bags with presetvative has 42 days expiry. Blood bags with prevervatives are<br />
available only at Mahanagar Blood Banks. Therefore in majority of the Blood Banks, blood<br />
bags expires in 35 days. Units which are not used are send back to Blood Bank at least 5<br />
days before expiry. It requires transport facility to collect blood from Blood Bank and to<br />
again send back to BB if not used. Curently ambulances of hosptials are used for this<br />
purpose. Cost of ambulance transportation is very high as its running cost is around Rs. 5<br />
per KM and also ambulance is not available for patients when it has gone for blood bags<br />
collection. Considerin g this problem, it is propoed to introduce innovative scheme for ue of<br />
Motor Cycle for transportation of the Blood Bags. One person per district will be employed.<br />
He will be provided motor cycle with one Cold Box fitted on rear seat. This person will be<br />
going to each hospital as per need and also be usefull for Blood Banks to get blood from<br />
other Blood banks in case of emergency. It is proposed to start this scheme as pilot at 4<br />
places in the state.<br />
Budget required for this scheme is as follows:<br />
Table – Budget required for transportation of blood bags to BSC<br />
Sir Activity Proposed<br />
No.of<br />
Units<br />
Unit cost<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
Page | 82
Sir Activity Proposed<br />
1<br />
2<br />
Procurement of Motor Cycle and<br />
fitting up of cold box on rear seat<br />
Salary of the Blood Bag Transporter<br />
(Rs. 8000/month for 6 months)<br />
No.of<br />
Units<br />
Unit cost<br />
Budget<br />
required<br />
4 0.6 2.4<br />
4 0.48 1.92<br />
3 POL for motor cycle 4 0.6 2.4<br />
Total 6.72<br />
SECTION - B.15 : PLANNING, IMPLEMENTATION AND MONITORING<br />
SUBSECTION - B.15.1 : COMMUNITY BASED PLANNING & MONITORING (CBPM)<br />
Approved<br />
SUBSECTION - B.15.2 : QUALITY ASSURANCE<br />
There are some changes in approval. However approval given is acceptable.<br />
SUBSECTION - B.15.3 : MONITORING AND EVALUATION<br />
Review meetings : Subject wise meetings not approved. Acceptable. This expenditure will<br />
be booked in respective program.<br />
15.3.1n : Staff for monitoring and evaluation : Computer specialist (2)<br />
ROP Remarks : New Post, Not approved.<br />
All the posts are approved except for Computer Specialist with comments that ‘New Post<br />
not approved’. This is not true. These posts are existing since last two years and persons are<br />
working on these posts. They are required for E-Office, maintaining HMIS website and<br />
website of NRHM. They are also helpful in troubleshooting in various software being used in<br />
State Health Society, Maharashtra. Therefore budget of Rs. 6.48 may be approved<br />
considering this explanation.<br />
15.3.1p : TA/DA to M & E Officer & 15.3.1q : TA to Statistical Officer.<br />
ROP Remarks : 25% amount approved to total proposed budget. Further, State needs to<br />
submit comprehensive plan subject to 100% facility based data reporting on HMIS portal.<br />
Maharashtra was using its own software till 2009 and after that DHIS-2 software. Meeting<br />
under Chairmanship of Hon. ACS (PH & FW) has taken decision to move to GoI software<br />
which has facility based data reporting system. Maharashtra needs to add few indicators to<br />
Page | 83
currently available GoI system. That process is going on. Facility masters are being prepared<br />
by the state. Major part of work is over and Maharashtra will switch on to the GoI software.<br />
Considering the progress State has made in accepting facility based data reporting, it is<br />
requested to release remaining budget for the state. Thus total Rs. 49.20 Lakh may be<br />
approved for TA/DA to M & E Officer and Rs. 39.60 Lakh for TA to Statistical Officer.<br />
15.3.1z : Contingency at District Level & 15.3.1aa : Contingency at State level :<br />
Remarks of ROP : Not approved.<br />
This contingency is basically required to maintain the internet connection, maintenance of<br />
computers and printers and stationary. All these three things are very important for HMIS to<br />
function. Therefore it is proposed to reconsider this decision and approve the activity.<br />
Considering this, contingency to district level Rs. 49.5 Lakh and Contingency at State level to<br />
all bureaus Rs. 24.0 lakh may be approved.<br />
15.3.1ab : Creation and maintenance of website<br />
Remarks of ROP : Not approved<br />
Currently three websites are being maintained by the State <strong>health</strong> Society. One website is<br />
for general information and tenders, advertisements, important circulars to be published.<br />
Second is for HMIS and third is for all the schemes of NRHM. Out of these, two websites are<br />
to be maintained daily and one on monthly basis. Approximately Rs. 10.0 Lakh required per<br />
website for routine updating and maintenance. Therefore, Rs. 30 Lakh as proposed may be<br />
approved.<br />
15.3.1ac : Establishment of State Data Health Center<br />
Approved activity.<br />
SUBSECTION - B.15.3.3 : MOTHER AND CHILD TRACKING SYSTEM<br />
Mother and child tracking system<br />
Approval received is acceptable.<br />
Strengthening of State MCTS Cell<br />
Approval received is acceptable.<br />
Training of district staff in MCTS<br />
Approval received is acceptable.<br />
Review of MUCH tracking activities<br />
Page | 84
Not approved. Acceptable.<br />
Monitoring of data collection and data activity<br />
Not approved. Acceptable.<br />
Establishing of State Level MCTS Call Center<br />
Approval received is acceptable.<br />
SECTION - B.16 : PROCUREMENT<br />
Procurement of some goods not approved by GoI. Few of the not approved activities need<br />
to be reconsidered. Activities that submitted for re-consideration with reasoning are<br />
submitted as below:<br />
B.16.1.5 : Procurement of Laptops<br />
Not Approved. Accepted<br />
B.16.2.2 : Drugs required for mass deworming and Vitamin A supplementation<br />
Remarks of ROP : Not approved. State to resubmit proposal with re-calculation and unit<br />
cost. Approval pended.<br />
B.16.2.4 : Procurement of Iron Folic Acid Tablets for adolescent boys and girls<br />
Remarks of ROP : Approved @ Rs. 0.15. Cost projected is higher. Rates to be obtained by a<br />
transparent bidding process.<br />
SECTION - B.17 : REGIONAL DRUG WAREHOUSE<br />
SUBSECTION - B.17.1 : STATE LEVEL ACTIVITIES<br />
Remarks of ROP : Not approved<br />
Government of India is informing the States to set up Tamil Nadu like structure for Health<br />
Department. Two specific letters are submitted hear. First is letter from Shri B. K. Prasad,<br />
Joint Secretary, GoI dated 25.3.10. In this letter staff to be appointed by State Governments<br />
is indicated. Second letter is from Shri K. Chandramouli, Secretary GoI dated 24.5.2010. In<br />
this letter also Hon. Secretary (H & FW) has instructed States to form Procurement<br />
structure. During NPCC meetings of 2010-11 and 2011-12 also States were informed to go<br />
for Separate structure like Tamil Nadu.<br />
Page | 85
Salient features of procurement system<br />
• Currently medicine and equipment are partly procured at state and partly at district<br />
level. As Procurement Division of the state is now fully functional all the purchases in<br />
<strong>2012</strong>-<strong>13</strong> will be by Procurement Division of the state.<br />
• E-tendering software and Inventory control software is introduced in the state. This<br />
has enabled to get precise information about stock situation of every drug and<br />
equipment and also in procurement.<br />
• Demand generation, distribution of drugs and stock position is completely<br />
computerized. Data entry is made at PHC level onwards.<br />
• Medicines purchased will be stored in Regional and District warehouses. Therefore 8<br />
warehouses at regional level and 33 warehouses at district level will be<br />
strengthened.<br />
• Currently there are two warehouses in each district. One for DHO (for PHCs) and one<br />
for CS (for DH and CHCs). Now onwards, only one warehouse will be constructed in<br />
District Hospital premises. This will save in manpower and security requirements and<br />
will be easy for monitoring.<br />
• All the Pharmacies in Public Health Department offices are now connected by web<br />
for inventory control. This system will be strengthened further.<br />
• Medicines will be purchased by E-tender system only.<br />
• Medicines required in very small quantity and of minimal cost (requirement less than<br />
Rs. 1000/institute in year) and medicines of short expiry (e.g. adrenaline) will only be<br />
purchased locally. All other medicines will be purchased from central level.<br />
• State level Procurement Cell, Regional and district stores, etc. will be supported<br />
under NRHM.<br />
• Daily stock of important medicines is being monitored in the state.<br />
• One Procurement Verification Officer is appointed since 2009-10. This person visits<br />
all the stores at Districts and major blocks and verifies the stock register, assures<br />
whether the stock book is maintained, all NRHM purchases are entered in registers,<br />
etc.<br />
Based on Guidelines of GoI, Maharashtra has done following progress:<br />
Previous system of procurement:<br />
Maharashtra has two separate departments for Medical Education and Public Health.<br />
Medical Education department was fixing rates of the medicines required to all the hospitals<br />
in the state under Medical Education, Public Health and ESIS. Rate contracts were published<br />
for three years and procurement was made by Districts and State offices as per need based<br />
on these rate contracts.<br />
System adopted by State Government since October 2011.<br />
Page | 86
1. Separate Procurement Section is established by Public Health Department for<br />
procurement of the medicines.<br />
2. List of Medicines required for each type of Hospitals finalized by experts.<br />
3. Quantity contract is published for one time with staggered supply as per need.<br />
Medicines required for all the <strong>health</strong> facilities and all the programs are included in<br />
this contract.<br />
4. Total contract is by E-Tendering system. Officers from Procurement Cell, important<br />
bureaus and Vendors were informed about the E-Tendering system. One workshop<br />
was organized specially for vendors to understand the E-Tendering System.<br />
5. Two bid systems similar to Tamil Nadu are applicable for medicine purchase except<br />
for World Bank funded projects.<br />
6. Staff is trained for procurement procedure at ASCI Hydrabad and YASHADA Pune.<br />
7. Committee under chairmanship of Secretary Public Health established. This<br />
committee includes officers from FDA, Industries Department, Medical Education,<br />
Medical Directors of Private Hospitals, etc.<br />
Distribution system for medicines<br />
1. All the Districts are to submit facility wise requirement to the State.<br />
2. Medicines are now purchased centrally by analyzing the requirement.<br />
3. Vender is supposed to supply medicines up to Divisional level. Warehouses are being<br />
established at all the 8 divisional places in the state.<br />
4. Medicines will be distributed to Health Facility and District Warehouses as per need<br />
of the program.<br />
5. One software is installed to all the Pharmacy Officers in the State. Received medicine<br />
is entered in this software. Utilization of medicines is also entered in this software.<br />
Staff in Procurement Cell<br />
Joint Director who is incharge of Procurement Cell is senior Public Health Department<br />
Officer. Other staff at State and Circle/District level is also appointed.<br />
Staff appointed at State level is mix of regular and contractual staff. Required staff which is<br />
not available from Government and mentioned in GoI letter is appointed on contract basis.<br />
Date of appointment of each of the staff is mentioned in remarks.<br />
Table – Appointment of staff in Procurement Cell<br />
Sr.No. Name & Designation Responsibility<br />
Regular/<br />
Contractual<br />
1 Joint Director of Health Services Overall in charge Regular<br />
2<br />
Deputy Director of Health<br />
Services<br />
Overall in charge Regular<br />
Page | 87
Sr.No. Name & Designation Responsibility<br />
3<br />
4<br />
5<br />
6<br />
Assistant Director of Health<br />
Services (Medicine)<br />
Shri.R.R.Rane, Supdt. All over Supervision (All files of<br />
Cell moves through), Court cases,<br />
Monitoring of all purchases done by<br />
procurement cell and related issues.<br />
Smt. Trupti Patil, Procurement<br />
Officer<br />
Smt. Vaishali Daulatkar,<br />
Procurement Officer<br />
7 Smt. Shrutika Patil, Pharmacist<br />
8 Smt. Varsha Gavane, Pharmacist<br />
9 Shri Jaywant Jadhav, Pharmacist<br />
10 Shri Sandeep Powar, Pharmacist<br />
11<br />
Smt. Gayatri Shetye, Data Entry<br />
Operator<br />
12<br />
Smt. Seema Waghmare, Data<br />
Entry Operator<br />
Shri A.G.Khandekar, Statistical<br />
<strong>13</strong> Assistant<br />
14<br />
Shri Rajesh Bhankal, Senior<br />
Clerk<br />
Establishment of regional<br />
Warehouses, Procurement of<br />
Medicines ( T. No.21-28)<br />
Procurement of Medicines ( T.<br />
No.<strong>13</strong>-20)<br />
Procurement of Medicine ( T. No.<br />
6-12)<br />
Procurement of Medicine ( T. No.<br />
28-34)<br />
Assistant to Smt. Trupti Patil<br />
Assistant to Smt. Vaishali<br />
Daulatkar<br />
Procurement as per requirement as<br />
per Jt.DHS<br />
( M,F & WBD)<br />
RTI, Meeting of State Purchase<br />
Committee, State Scrutiny<br />
Committee & Director level<br />
Purchase Committee and<br />
Miscellaneous<br />
Regular/<br />
Contractual<br />
Regular<br />
Regular<br />
Contractual<br />
(From Sept.11)<br />
Contractual (From<br />
March 12)<br />
Contractual (From<br />
Dec.11)<br />
Contractual (From<br />
March.12)<br />
Contractual (From<br />
March 12)<br />
Contractual (From<br />
February 09)<br />
Contractual (From<br />
Sept.08)<br />
Regular<br />
Regular<br />
15 Smt. A.V.Joshi, Junior Clerk Inward Outward Regular<br />
16<br />
Smt. Chanda Dhurandhar,<br />
Lower Grade Steno<br />
P.A. to Jt. DHS<br />
Regular<br />
17<br />
18<br />
19<br />
20<br />
Assistant Director of Health<br />
Services (Instruments &<br />
Regular<br />
Equipment )<br />
Smt. Hire, Senior Clerk Procurement of Instrument<br />
Equipment for NPCB Regular<br />
Shri. Arvindekar, Senior Clerk Procurement of Lab. Equipment ,<br />
Rate contract of Lab. Material & as<br />
per requirement of Jt. DHS<br />
Shri K.S.Patil,<br />
Senior Clerk<br />
(Hospital)<br />
Procurement of Instrument<br />
Equipment for Deafness control<br />
program & as per requirement of Jt.<br />
DHS (Hospital)<br />
Regular<br />
Regular<br />
Page | 88
Sr.No. Name & Designation Responsibility<br />
21<br />
22<br />
23<br />
24<br />
25<br />
26<br />
Shri Amit Karchalwar,<br />
Procurement Officer<br />
Smt. Saraswati Patil,<br />
Procurement Officer<br />
Shri Yogesh Yevale,<br />
Procurement Officer<br />
Smt. Monali Sankhe, Quality<br />
Assurance Officer<br />
EMS, HACC, Solar Photovoltaic<br />
Inverter System, Hospital Furniture,<br />
Radiodignostic Center on PPP basis<br />
Printing of Banner, Poster, Booklet,<br />
Flipbook for IEC Program,<br />
Purchase by inviting quotations.<br />
Procurement of vehicle, Software &<br />
Computer and All paper bill<br />
Pre-Dispatch Inspection &<br />
Demonstration of Instruments &<br />
Equipment.<br />
Shri F.B.Sayyed, Pharmacist Sell of Tender Document,<br />
Collection of Samples, EMD<br />
Shri Swapnil Bawiskar, Data<br />
Entry Operator<br />
Assistant to Smt.Hire<br />
Regular/<br />
Contractual<br />
Contractual (From<br />
May 09)<br />
Contractual (From<br />
May 09)<br />
Contractual (From<br />
Dec.11)<br />
Contractual (From<br />
Sept.11)<br />
Contractual (From<br />
February 11)<br />
Contractual (From<br />
Feb.11)<br />
Similarly, One Pharmacist is appointed each at Circle Medicine Store, DHO Medicine Store<br />
and Civil Surgeon Medicine Store. These appointments are from year 2010-11.<br />
Major part of staff is appointed during 2010-11 and also during 2011-12 as per guidelines of<br />
GoI. Except for the post of Senior Consultant (Doctor) and Procurement Consultant<br />
(Pharmacy Postgraduate) all other staff already exists in the Department. Therefore these<br />
staffs need to be continued.<br />
Circle level and district level staff is appointed as per guidelines in 2009-10. This staff is<br />
existing since last three years. Therefore this staff is also required to be continued.<br />
Repairs and contingency<br />
Regarding repairs of Warehouses, this activity is completely revised and submitted in table<br />
below> Contingency is required to continue the internet facility, photocopying, travel for<br />
pre-dispatch inspection for NRHM procurements, etc. Considering this, it is proposed to<br />
approve these activities.<br />
Budget requirement – <strong>2012</strong>-<strong>13</strong><br />
Budget requested in this PIP is for currently functioning system, i.e. for divisional and district<br />
warehouses. Considering the above plan, budget required for procurement plan of<br />
Maharashtra state is as given below:<br />
Table - : Procurement Plan of Maharashtra state : <strong>2012</strong>-<strong>13</strong><br />
Sr Particulars Unit cost<br />
A State Level Activities<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
Page | 89
1<br />
Sr. Procurement Consultant (Medical<br />
Postgraduate with at least 3 years’ experience in<br />
Procurement and trained at reputed agency in<br />
World Bank Procurement Procedure)<br />
Procurement Consultant (Pharmacy postgraduate<br />
5 1 5<br />
2<br />
with at least 3 years’ experience in procurement<br />
and Trained at reputed agency in World Bank<br />
Procurement procedure)<br />
Salary of Procurement Officer (medicines (2),<br />
3.6 1 3.6<br />
1 Equipment (2) and Other goods (1) at state<br />
procurement cell<br />
3.4 5 17<br />
2<br />
Salary of procurement assistant /Pharmacist at<br />
state procurement cell (6)<br />
1.26 8 10.08<br />
3 Quality Assurance Officer 2.6 1 2.6<br />
5 Contingency to Procurement Cell 15 1 15<br />
6<br />
Travel and Daily allowances to State Procurement<br />
Officers for pre-dispatch inspection and meetings<br />
20 1 20<br />
B Circle and District Level activities<br />
1<br />
Repairs and new construction of Circle<br />
warehouses<br />
12 8 96<br />
2<br />
Repairs and new construction of District<br />
Warehouses<br />
<strong>13</strong> 33 429<br />
3 Pharmacist to DHO/CS and Circle warehouses 1.26 74 93.24<br />
4 Contingency to circle and district warehouses 1.2 74 88.8<br />
5 Stores Verification Officer (Rs. 25000/PM) 3.4 1 3.4<br />
Total 783.72<br />
SECTION - B.18 : NEW INITIATIVES / STRATEGIC INTERVENTIONS / PROJECTS<br />
SUBSECTION - B.18.1 : BIOMETRIC ATTENDANCE FOR HEALTH STAFF<br />
Presence of <strong>health</strong> staff is important to provide <strong>health</strong> services. Many times serious patients<br />
get delayed treatment because concerned staff is not available. Therefore, it is essential to<br />
monitor the arrival and leaving of <strong>health</strong> staff in hospitals/PHCs and concerned<br />
establishments. Three districts in Maharashtra, Thane, Akola and Wardha have<br />
implemented biometric attendance system on pilot basis. Attendance and timeliness of<br />
<strong>health</strong> staff in these districts have improved significantly. Based on experience of these<br />
districts, it is proposed to extent this scheme to all the PHCs, RHs and District Hospitals of<br />
the state.<br />
Salient features of the scheme will be as follows:<br />
• Biometric attendance is being installed in all the offices and <strong>health</strong> facilities except<br />
THO office and PHCs this year. These places will be covered in 2011-12.<br />
Page | 90
• The staff including senior officers will be required to put thumb impression on the<br />
device at the time of arrival and at the time of leaving the hospital. The device will<br />
keep record of arrival and departure.<br />
• The biometric device will be connected online with central server at district level and<br />
state level.<br />
• District information will be available on line to CEO ZP, DHO and Civil Surgeon at<br />
district level and Director of Health services and ACS (PH & FW) at state level.<br />
• Special efforts with the help of experts will be made in PHCs where there is no<br />
internet connection available for submitting information. These PHCs are not more<br />
than 10% in state.<br />
• Central server for HMIS will be sued for this purpose.<br />
Compliance of remarks<br />
• Biometric Attendance system is being used for basically two types of staff. One is<br />
office staff having fixed duty hours from 9.45 AM to 5.30 PM and <strong>health</strong> facility staff<br />
having changing duty system.<br />
• Regarding office staff, the system has started showing results within one month. As<br />
this system records impression of fingers, the person has to come to office in time.<br />
This is now being linked to salary software from 1.4.<strong>2012</strong>. After that every absentee<br />
will be treated as LWP unless certified by controlling officer.<br />
• Regarding clinical staff like doctors, nurses and support staff who have changing<br />
duties, there is some problem at operational level particularly in bigger hospitals.<br />
These problems are being sorted out with the help of IT experts.<br />
• Total data of the district is received at district, regional and state HQ. This data is<br />
reviewed. Even senior officers are called by Hon. ACS (PH) for their explanation if<br />
they are consistently late to office.<br />
• Except at 2 places in the state, the machine was well accepted by staff. No mischief<br />
was done but staff to make the machine out of order.<br />
• We expect that because of timekeeping by doctors and nurses, accessibility will be<br />
improved which will finally improve quality of <strong>health</strong> care delivery. However, till<br />
today no systematic study is done for this.<br />
• For year <strong>2012</strong>-<strong>13</strong>, the expansion will be in PHC where problem of regular attendance<br />
is much more serious.<br />
Considering above fact, it is proposed to approve this scheme.<br />
Budget requirement<br />
Budget requires for following purposes<br />
• Biometric device<br />
• Staff for monitoring<br />
Computers and internet facility is already available in PHC and all hospitals, therefore there<br />
is no request for budget for these items. Staff mentioned below is sanctioned in 2011-12<br />
and was appointed last year. This staff will be continued this year.<br />
Detailed budget requirement is as follows:<br />
Page | 91
Table -: Budget required for biometric attendance in <strong>health</strong> institutions<br />
Sr Activity Unit cost<br />
No.of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
1 Biometric equipment in PHCs and THO offices 0.3 1246 373.8<br />
2 One Computer Manager at DHS 3 1 3<br />
3 Computer Assistants one in each circle and 4 at DHS 1.26 12 15.12<br />
4 Contingency, internet stationary at circle HQ 0.5 8 4<br />
6 Contingency at state HQ 1.2 1 1.2<br />
Total 397.12<br />
SUBSECTION - B.18.2 : PREVENTION OF SICKLE CELL DISEASE<br />
For Sickle Cell Disease Control Program, budget of Rs. 1816.95 Lakh was requested out of<br />
which Rs. 1781.92 Lakh is approved. Few activities especially new staff is not approved.<br />
Explanation for approval of these activities is submitted for re-consideration.<br />
It is requested to consider the above and sanction the counselors for Sickle Cell Disease<br />
Control Program at Day Care Centre level.<br />
2. Salary of Lab Tech. in DH & WH (Day Care Centre)<br />
Remarks:- New staff not approved<br />
Justification:- The Hon. Lokayukta, Maharashtra State has ordered the establishment of Day<br />
Care facilities for treatment of Sickle Cell patients at district level. Electrophoresis and HPLC<br />
(Confirmatory test for SCD) are made available in district and women's Hospitals. Presently,<br />
there is no dedicated lab technician for electrophoresis test. Since this is a long and skilled<br />
procedure, a separate, specially trained lab technician is needed for testing at DH/WH level.<br />
This technician would also be responsible for all tests to be performed for Sickle Cell<br />
Sufferers who come to Day Care Centre. As these are skilled posts and considering the load<br />
of patients and Lokayukta ruling, it is requested to sanction these technicians.<br />
3. Salary & TA DA of SCD Coordinator (NGO Districts)<br />
Remarks:- Approved for 10 SCD Coordinator for Rs.1.62 lakhs per annum as per last year<br />
rates<br />
Justification:- The total no. of required units is 11 as there are 20 districts included in Sickle<br />
Cell Program out of which 11 are NGO districts. As only 10 posts are sanctioned it is<br />
requested to sanction one additional post. This post is there from 2009-10.<br />
The previous year's rate was 1.74 lakhs per annum. Therefore the calculated cost of 11<br />
Coordinators as per previous year's rates is 11 X 1.74 = 19.14 lakhs<br />
4. Salary & TA DA of SCD Coordinator (Non-NGO Districts)<br />
Remarks:- Approved for 9 SCD Coordinator for Rs.1.62 lakhs per annum as per last year<br />
rates<br />
Justification:- The previous year's rate was 1.74 lakhs per annum. Therefore the calculated<br />
cost of 9 Coordinators as per previous year's rates is 9 X 1.74 = 15.66 lakhs<br />
Page | 92
B.18.2.3 : DISTRICT LEVEL BUDGET REQUIREMENT FOR NGO DISTRICTS.<br />
Salary of Laboratory Technician in DH/WH (Day care center) & Salary of Counselor in<br />
District Hospital (Day Care Center)<br />
Remarks of ROP : New Staff. Not approved.<br />
B.18.2.4 : HEALTH WORKER DISTRICT BUDGET (NON NGO) FOR NGO DISTRICTS.<br />
Salary of Laboratory Technician in DH/WH (Day care center) & Salary of Counselor in<br />
District Hospital (Day Care Center)<br />
Remarks of ROP : New Staff. Not approved.<br />
Justification :-The Hon. Lokayukta, Maharashtra State has ordered the establishment of Day<br />
Care facilities for treatment of Sickle Cell patients at district level.<br />
More and more Sickle Cell patients and Carriers are being detected during screening. As this<br />
is a genetic disease it is mandatory to counsel Sickle Cell Carriers and Sufferers for marriage,<br />
family planning and regular treatment. No other trained and dedicated staff is available at<br />
district hospital level for Counseling of Sickle Cell patients and Carriers. The role of the<br />
Counselor is envisaged as follows:-<br />
Create individualized diagram of inheritance for each Sufferer (Punnet square) and family<br />
tree when required based on laboratory results. Provide genetic counseling: Counseling<br />
prior to screening, Counseling of Carriers, Counseling of Sufferers, Counseling for antenatal<br />
testing of eligible couples, Group counseling (Sufferer support group). Provide psychosocial<br />
support. Provide information and support needed to make decisions about marriage and<br />
family planning Provide educational materials to patient and family. Provide information<br />
about <strong>health</strong> problems which can occur in SCD and recommendations for regular treatment.<br />
Provide information and counseling regarding pre-natal diagnosis and facilitate the testing.<br />
SUBSECTION - B.18.3 : TELEMEDICINE PROJECT<br />
Salary & TA/DA of Telemedicine Consultant<br />
Remarks: - Approved as per last year's rates<br />
Justification: - Last FY 2011-12 Rs. 2.70 Lakhs Salary & TA/DA for the Telemedicine<br />
Consultant was proposed for only 9 months.<br />
In this FY <strong>2012</strong>-<strong>13</strong> the post of telemedicine consultant was already filled up & therefore the<br />
Salary & TA/DA will required for 12 months. Therefore it is sincere request to sanction the<br />
proposed amount on account of Salary and TA/DA of Telemedicine Consultant.<br />
SUBSECTION - B.18.4 : HAEMATOLOGY PROGRAM<br />
Approval accepted<br />
SUBSECTION : B.18.5 : SHORT TERM CERTIFICATE COURSES FOR MEDICAL OFFICERS IN<br />
PUBLIC HEALTH DEPARTMENT<br />
Page | 93
Maharashtra state has started short term certificate courses for Medical officers in Public<br />
Health Department of Maharashtra because Presently proportion of vacancies in the<br />
specialties’ like Pediatrics and Medicine is more than 60%. Specialists are not willing to join<br />
<strong>rural</strong> areas although appointed by the department due to various reasons like payment,<br />
basic amenities, lack of education facilities etc. Those who join the department are not<br />
continuing and proportion of leaving the job is significant etc. Necessary infrastructure has<br />
been developed at hospital level however it is not optimally utilized due to shortage of<br />
specialists.<br />
Requirement and availability of all type of specialists is as below.<br />
o Total posts of specialists sanctioned 521<br />
o Out of that post filled : 176<br />
o Total number of vacancies 346<br />
Therefore to fulfill the requirement of department of providing appropriate speciality<br />
services, Government has started short term training courses in all required specialities.<br />
Initially this will cover Pediatrics and Medicine and in due course other subjects like<br />
Gynecology, Obst. and Anesthesia will be included as per need. In addition to this training<br />
will also be imparted to Medical officers and some paramedical staff in disciplines like Bio<br />
chemistry, Microbiology and Radiology and Psychiatry .<br />
The training will be in the form of a certificate course and the certificate will be given<br />
by the Directorate of Health Services this will be only for working in the <strong>health</strong> facilities of<br />
<strong>health</strong> department and not for general practice outside the department.<br />
With the approval from Government of Maharashtra. We already have formulated core<br />
committee under Chairperson Dr. Mrudula A. Phadke ( Ex<br />
Vice- Chancellor of Maharashtra University of Health Sciences) For planning,<br />
implementation and monitoring of these training courses.<br />
Trainees have been identified from Medical officers with MBBS qualification who<br />
are already working in the dept. and willing to work at least for five years in the department,<br />
initially the selected medical officers were deputed to Nine govt. Medical colleges for the<br />
training and now next batch has 9 medical college and Duration of Course will be 6<br />
months. Curriculum has been prepared as per the requirement of the department based on<br />
the clinical services expected to be delivered at the respective hospital level. And these has<br />
been developed by the experts in the corresponding field. These experts group has been<br />
appointed by the core committee.<br />
Training will be given at following sites depending on the availability of trainers and also<br />
clinical cases.<br />
Medical College both govt. and Private as per willingness consent has already<br />
been taken from Medical Education Dept.<br />
All District Hospitals.<br />
Private Hospitals.<br />
Trainers have been appointed by the core committee.<br />
Page | 94
Examination of first batch will be held on 29 th and 30 th of June and successful<br />
candidates on 29 th and 30 th of June and successful candidates will be given MOCP<br />
certificates through D.H.S.<br />
Now Government Department of Public Health has issued 2 GR including 6 more<br />
colleges. So the training will be imparted through 9 colleges and around 90 Medical<br />
Officers will be trained. These Colleges are as under.<br />
1) Government Medical College, Nagpur<br />
2) Government Medical College, Aurangabad<br />
3) B. J. Medical College, Pune<br />
4) Seth G. S. Medical College and KEM Hospital, Parel, Mumbai<br />
5) Topivala National General Medical College and B. Y. Nair hospital, Mumbai Central,<br />
Mumbai<br />
6) Lokmanya Tilak Municipal General Hospital and Lokmanya Tilak Municipal College,<br />
Sion (West), Mumbai<br />
7) ESI-PGIMSR Mahamta Gandhi Memorial Hospital, Parel, Mumbai<br />
8) Mahamta Gandhi Institute of Medical Science, Sewagram, Wardha<br />
9) Sir J J Hospital – Grant Medical College, Byculla, Mumbai.<br />
After having taken the training and completing MOCP course these Medical Officers will<br />
be deputed in strategic PHCs like in Dhule (Nardhana), Nandurbar, (R.H. Molgi), Igatpuri and<br />
others where they will be able to take ECG’s, manage patients of cardiac ailments, infants<br />
with septicemia and malnutrition. This will be the ideal utilization of doctors after training.<br />
Budget requirement<br />
Budget is revised as per discussion during 6-8 June <strong>2012</strong>. Budget for each course will be<br />
required for various activities as below:<br />
Table – Budget required for MOCP Course<br />
No Activity Rate<br />
Rs. In Lakhs<br />
Budget required<br />
1. Preparation of training curriculum, Rs. 1 lac. For all 9<br />
1<br />
listing of essential skills, time table colleges<br />
etc.<br />
2. Remuneration for trainers 0<br />
a. For theory sessions (there will be Rs. 1000 for each<br />
2.4<br />
about 5-10 trainers. They will take Session *24<br />
one session per week. Total 24 Session *10<br />
sessions of each trainer)<br />
Trainers<br />
b. For practical and hands on training Rs. 10000/- per<br />
7.2<br />
(There will be about 5 – 12 trainers month*12 trainers<br />
from local district)<br />
* 6 months<br />
Page | 95
3. Contingency funds for printing<br />
training material conduct of<br />
examination books etc.<br />
4 Office expenses Rs. 50,000 per<br />
month<br />
Videoconferencing expenditure for<br />
virtual classroom<br />
5 Facility of video conferencing and<br />
CD preparation<br />
Total 22.6<br />
Every Batch of 90 students at 9 colleges, the expenditure is Rs. 22.6 lakhs.<br />
SUBSECTION – B.18.6 : NEW INITIATIVES IN HIGH FOCUS DISCTRICTS<br />
High Focus districts have special probmels. Considering this, new initiatives are planned in<br />
these districts. Theses activtiies were submitted in separate chapter of high focus districts.<br />
However, as per discussion during 6-8 June <strong>2012</strong>, these activities are shifted to chapter of<br />
new initiatives.<br />
B.18.6.1 : Health Shelter In Nandurbar District<br />
In blocks of Dhadgaon and Akkalkuwa, many of the <strong>health</strong> facilities and also villages are at<br />
such a remote place that <strong>health</strong> worker need to travel up to 45 Kilometers on foot to reach<br />
remote villages from his/her HQ. This makes extremely difficult for them to travel to these<br />
remote villages. There are no homes, schools or other places to stay overnight for the staff.<br />
Considering this peculiar situation, it is proposed to build pre-fabricated shelter homes at<br />
places where the villages are more than 25 KM from HQ of the <strong>health</strong> worker. Ten places in<br />
these blocks have been identified for such shelter homes.<br />
Shelter will be two rooms of 150 sq. feed one for male staff and one for female staff, one<br />
kitchen of 50 sq. feet and one toilet block of 50 sq. feet. Total shelter will be of 400 sq. feet.<br />
Local SHG or ASHA will be given responsibility to maintain the shelter. She will be paid Rs.<br />
3000/PM towards maintenance and provision of food. Food charges will be borne by<br />
concerned <strong>health</strong> worker.<br />
List of facilities where <strong>health</strong> shelter is required is submitted in annexure<br />
Budget requirement<br />
Budget required for shelter is for construction of shelter, maintenance and contingency for<br />
keeping drinking water, etc. Detailed budget requirement is as follows:<br />
Table – Budget requirement for Health Shelter<br />
5<br />
3<br />
0<br />
4<br />
Rs. In Lakhs<br />
Sir Activity Unit cost No.of Budget<br />
Page | 96
1<br />
Construction of Health Shelter including one bore<br />
well for water supply (one time)<br />
units required<br />
12 10 120<br />
2 Maintenance by SHG/ASHA 0.36 10 3.6<br />
3<br />
Other maintenance charges (Drinking water,<br />
electricity, drainage, etc.)<br />
0.36 10 3.6<br />
4 Furniture grant (one time) 0.5 10 5<br />
Total <strong>13</strong>2.2<br />
B.18.6.2 : Wireless Contact In Nandurbar District<br />
Major part of interior areas in the district is not approachable by any means of<br />
communication including mobile phones and BSNL wireless network. Therefore it is<br />
proposed to provide one wireless set to each of the SC in interior areas. The base of the<br />
wireless network will be at district level. Message for ambulance to shift mother in labour,<br />
critically ill child and epidemics are expected from this system. System will be procured by<br />
following procurement procedure. Budget required for this activity will be as follows<br />
Table – Budget requirement for Wireless contact system<br />
Sir Activity Unit cost<br />
No.of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
1 Wireless set 0.5 56 28<br />
2 Base station at Nandurbar 5 1 5<br />
3 Salary of operator at Nandurbar 1.2 1 1.2<br />
4 Contingency including civil works, stationary, etc. 0.5 1 0.5<br />
Total 34.7<br />
B.18.6.3 : Floating Dispensaries And Floating Ambulances In Nandurbar District<br />
About 50 villages of Nandurbar district are completely isolated due to Backwaters of Sardar<br />
Sarovar. These villages have mountain on one side and back water on other side.<br />
Government of Maharashtra is providing <strong>health</strong> services to theses villages by floating<br />
dispensaries. These dispensaries visit all the villages on fixed days and provide services. Only<br />
the post of Medical Officer and Driver are approved by Government. These dispensaries are<br />
providing good services, however, in case of emergency, particularly the delivery case or<br />
critically sick child, they have to discontinue the service and take the patient back to Health<br />
Facility for treatment. This leads to major disruption of services to remaining villages and<br />
irregularity in service provision.<br />
Page | 97
Distance between floating dispensary and bank of river changes every time and patients<br />
need to travel in water to reach dispensary. This becomes very difficult for the patients<br />
particularly the pregnant women. In addition there is no place for patients to wait till the<br />
Floating dispensary approaches the villages. Therefore, one clinic room is proposed at each<br />
stop of the dispensary.<br />
Considering the above condition, it is proposed to provide additional essential staff and<br />
space to Floating Dispensary and three Floating Ambulances to this areas so that these<br />
ambulances can be called to shift pregnant women, critically ill neonates and other sick<br />
persons. The ambulance will be called through wireless contact system.<br />
Budget required for this activity is as mentioned in table below:<br />
Table – Budget requirement for Floating dispensaries and Ambulances<br />
Sir Activity Unit cost<br />
No.of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
A Floating dispensary<br />
1 Pharmacist (one per dispensary) 1.2 2 2.4<br />
2 ANM 1.44 2 2.88<br />
3 Laboratory Technician 1.2 2 2.4<br />
4 Construction of clinic (Fibre - 400 sq. feet) 12 16 192<br />
5 Maintenance of clinic by local ASHA 0.36 16 5.76<br />
6 Solar light system and water supply 3 16 48<br />
4 Assistant 0.96 2 1.92<br />
5 Medicine 0.5 2 1<br />
6 Additional POL 0.5 2 1<br />
Total Floating dispensary 257.36<br />
B Floating Ambulance<br />
1 Procurement of Floating Ambulance 20 3 60<br />
2 One Driver 0.48 3 1.44<br />
3 One ANM in ambulance 0.72 3 2.16<br />
4 One Assistant 0.36 3 1.08<br />
5 Total Floating Ambulance 64.68<br />
Grand Total 322.04<br />
Considering the time required for procurement, salary of staff for Floating ambulance is<br />
requested for six months only.<br />
Subsection - B.18.6.4 : Specialised Services By Speciality Vans In Gadchiroli District<br />
Gadchiroli district is completely LEA area and length of the district is about 350 KM. Except<br />
for DH Gadchiroli and SDH Aheri, there is no availability of dentist, pathology unit or the<br />
Ophthalmological unit. Considering this, six mobile units have been supplied under IAP to<br />
Gadchiroli districts. These include 2 Dental Units, 2 Pathology Units and 2 Ophthalmologist<br />
Page | 98
units. However, these units are not functional due to non-availability of funds for manpower<br />
and operational expenses. As no such services are available in periphery, these units are<br />
extremely essential for the district. Considering this, it is proposed to support these units<br />
from Mission Flexi Pool. Budget required for these units is as follows:<br />
Table – Budget required for operationalization of Mobile Units<br />
Sir Particulars<br />
Unit<br />
rate<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
A Mobile Dental Unit (2)<br />
1 Salary of Dentist (Rs. 20000/PM) 2.4 2 4.8<br />
2 Salary of Dental Technician (Rs. 12000/PM) 1.44 2 2.88<br />
3 Salary of Attendant (Rs. 6000/PM) 0.72 2 1.44<br />
4 Salary of driver (Rs. 8000/PM) 0.96 2 1.92<br />
5 Medicines and consumables (Rs. 1.2 L/year) 1.2 2 2.4<br />
6 POL 1.2 2 2.4<br />
7 Overheads 1 2 2<br />
Total 17.84<br />
B Mobile Ophthalmic Unit (2)<br />
1 Salary of Ophthalmic Officer (Rs. 14000/PM) 1.68 2 3.36<br />
3 Salary of Attendant (Rs. 6000/PM) 0.72 2 1.44<br />
4 Salary of driver (Rs. 8000/PM) 0.96 2 1.92<br />
5 Medicines and consumables 0.6 2 1.2<br />
6 POL 1.2 2 2.4<br />
7 Overheads 1 2 2<br />
Total 12.32<br />
A Mobile Pathology Unit (2)<br />
1 Salary of Doctor (Rs. 25000/PM) 3 2 6<br />
2 Salary of Laboratory Technician (Rs. 12000/PM) 1.44 2 2.88<br />
3 Salary of Attendant (Rs. 6000/PM) 0.72 2 1.44<br />
4 Salary of driver (Rs. 8000/PM) 0.96 2 1.92<br />
5 Lab consumables 6 2 12<br />
6 POL 1.2 2 2.4<br />
7 Overheads 1 2 2<br />
Total 28.64<br />
Grand Total 58.8<br />
Page | 99
SUBSECTION - B.18.7 : STRATEGIC INTERVENTIONS TO IMPROVE HEALTH CARE<br />
MANAGEMENT<br />
Considering the volume of activities being carried out by Public Health Department, number<br />
of persons involved and amount data generated in system, it has been decided to<br />
computerize all the activities in the state step by step. Ultimate aim of the computerization<br />
is to get real time data for all important indicators and enable the higher level managers to<br />
act upon without any time lag. It is also important to monitor the grievences of public in<br />
getting the services. Considering this, following programs are submitted for approval.<br />
The programs mentioned below were submitted under M & E Seciton. However as per<br />
discussion during 6-8 June <strong>2012</strong>, these activities are re-located to Section B.18 as follows:<br />
B.18.7.1 : Establishment And Functioning Of Grievance Cells<br />
Under Community Based Monitoring System, Grievance Cell is to be established at all<br />
District Headquarters, Circle and State Headquarters. After that GoI published guidelines to<br />
establish Grievance cell for JSY and recently for JSSK. Considering the importance of<br />
Grievance cell, following action was taken:<br />
1. One Grievance Cell at SHS. This cell established in 2009-10. There is one Grievance<br />
Redressal Officer and one DEO approved and functioning on this post. One Joint<br />
Director level officer is in charge of the cell.<br />
2. One Grievance cell at each of the Circle. One Grievance Redressal Officer is<br />
appointed in each circle. There is Grievance redressal committee at circle level.<br />
Members of committee are:<br />
a. Deputy Director i/c circle or his representative<br />
b. One NGO representative, preferably the CBM NGO of the city<br />
c. One retired judge or senior journalist of the city<br />
3. One Grievance Redressal Cell is established at each District HQ. No contractual staff<br />
is appointed here. Administrative Officer of FW Program is incharge of cell and DPM<br />
assists the AO for this activity.<br />
Work done by GR Cell<br />
Work done by GR Cell is mentioned below:<br />
• During the year 2011-12, Grievance cell received total 291 complaints. All these<br />
complaints were processed. Out of these, action completed in <strong>13</strong>1 complaints and<br />
action in process in 160 complaints.<br />
• Lot of complaints are received regarding grievances against regular staff. Such<br />
complaints are tracked till enquiry is made and enquiry report is sent to DHS for<br />
further action. Enquiry has been started against <strong>13</strong> officers due to constant follow up<br />
of the Grievance Cell.<br />
• Currently, grievance Cell is also entrusted responsibility of tracking the news appear<br />
in local newspapers.<br />
Page | 100
• Telephone charges are doubled due to increase in follow up of the complaints to<br />
district and state HQ. This is good indication.<br />
Following are the details of grievances registered in the year April 2011 to march 12<br />
Sr. no Grievance Cell Office<br />
Name<br />
No Of<br />
Complaints<br />
Received<br />
Year 2011-12<br />
No Of<br />
Complaints<br />
Resolved<br />
No of<br />
Complaints<br />
In process<br />
1 State Office, Mumbai. 80 55 25<br />
2 Dy. Director, Health,<br />
Pune Office<br />
11 6 5<br />
3 Dy. Director, Health,<br />
Thane Office<br />
16 4 12<br />
4 Dy. Director, Health,<br />
Kolhapur Office<br />
<strong>13</strong> 9 4<br />
5 Dy. Director, Health,<br />
Aurangabad Office<br />
17 8 9<br />
6 Dy. Director,<br />
Health, Latur Office<br />
50 8 42<br />
7 Dy. Director, Health,<br />
Akola Office<br />
26 6 20<br />
8 Dy. Director, Health,<br />
Nagpur Office<br />
56 31 25<br />
9 Dy. Director, Health,<br />
Nashik Office<br />
22 4 18<br />
Total 291 <strong>13</strong>1 160<br />
Budget requirement<br />
Budget required for grievance cell is for telephone and Grievance Redressal Officer. Budget<br />
will be required to one state cell and one cell each for 8 circle offices in state. Total budget<br />
required is as follows:<br />
Table - : Budget requirement for grievance cell<br />
Sir Activity Unit cost<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
1 Telephone charges 0.48 9 4.32<br />
2 Salary of GR Officer 2.4 9 21.6<br />
3 Salary of DEO to GR Officer at state 1.26 2 2.52<br />
3 TA/DA to nonofficial members 1.2 8 9.6<br />
4 Contingency 0.6 8 4.8<br />
Total 42.84<br />
Page | 101
Considering the fact that all the GR offices are in position since 2011-12 and work done by<br />
the GR Cell and also considering guidelines of GoI under JSY and JSSK to establish GR Cell, it<br />
is requested to approve this activity for year <strong>2012</strong>-<strong>13</strong>.<br />
B.8.7.2 : Computerization Of HMIS, E-Governance And E-Health<br />
Presently, following E-Governance activities are being carried out or in execution stage in<br />
the state<br />
• E-office introduced for the first time in Maharashtra at NRHM Mumbai. It has<br />
started functioning well.<br />
• Biometric attendance system in all <strong>health</strong> offices, PHCs and hospitals. Biometric<br />
system is installed in all the Hospitals. Once it is functional, PHCs will be<br />
introduced in the system.<br />
• Development of ASHA software – ASHA software already developed. Information<br />
of about 60000 ASHA in place. Software has helped to pay compensation to<br />
ASHA in time.<br />
• Hospital MIS software being established in State initially for 23 District Hospitals,<br />
4 General Hospitals and 8 Women Hospitals. This software will completely<br />
computerize the hospital functioning and will improve the efficiency of the<br />
system.<br />
• Inventory management - Computerization of Medicine distribution system –<br />
already started and providing good results. Now daily monitoring of all the<br />
important medicines in all <strong>health</strong> facilities of state is possible. This has resulted<br />
into saving of medicines from expiry, calculating correct demand, indications<br />
before the medicine is out of stock.<br />
• Computerization of Medical Equipment inventory – This software is also in<br />
progress and is being prepared with the help of agency appointed by Department<br />
of Information Technology, Govt. of Maharashtra.<br />
• Fund transfer through E-banking to district level – already started in all the<br />
districts, circle offices and training centers.<br />
• Payment of cheques through e-banking – Cheques to venders and other<br />
personnel are now being paid through e-banking.<br />
• Tally ERP-9 Introduced at state, district and block level.<br />
• GIS mapping with the support from UNICEF – GIS maps are being used for<br />
decision making and presentation in the state.<br />
• Use of MCTS software and HMIS software as per GoI guidelines.<br />
• E-transfer – All the request transfers are now online. Officers interested in<br />
request transfer will have to submit their request online to the Government.<br />
These requests will be considered based on need and transfers will be made.<br />
B.18.7.3: E- Office and Software For Hospitals<br />
Considering the implementation of all the above mentioned activities in the state following<br />
actions are proposed for year <strong>2012</strong>-<strong>13</strong> :<br />
Page | 102
1. Creation of awareness among <strong>health</strong> officials for E-Governance: All the officers of<br />
Health Department need to know the strengths of E-Governance and advances of<br />
technology available for <strong>health</strong> related monitoring. If they understand the concepts<br />
and benefits of E-Governance, then they will start monitoring from their own.<br />
Considering this, now there is one session of senior IT expert regarding technologies<br />
available for <strong>health</strong>. As these sessions are included in regular meetings, no additional<br />
cost is required for this activity.<br />
2. Expansion of E-Office to other State level Offices: E-Office is started in SHS office<br />
and senior officers related to NRHM such as Director of Health Services, Additional<br />
Chief Secretary (PH&FW), etc. The software is from NIC and installation, training,<br />
handholding for one year, maintenance, etc. is being carried out by NIC. One<br />
department of Directorate (Joint Director (Hospitals)) is also included in the scheme.<br />
Now it is proposed to expand this scheme to all the state level offices in Mumbai,<br />
Pune and Nagpur. These offices will require Computers, Scanners, cabling, etc. for<br />
these offices. This is very important for Maharashtra as State level offices in the state<br />
are situated in three different cities and at 8 different places.<br />
3. Establishment and Expansion of Hospital Software : Maharashtra has 455 hospitals<br />
and bed strength of these hospitals ranges from 30 beds to 550 beds. It is proposed<br />
to completely computerize these hospitals in phased manner. Initially all District<br />
Hospitals, all women hospitals and hospitals above 200 beds (General Hospitals) are<br />
being computerized and later on 100 bedded hospitals will be included for<br />
computerization. The software for computerization is prepared by Tata Consultancy<br />
Services and will be procured from Maha-online a Government of Maharashtra<br />
company. Budget required for this will be for software, computers, servers and LAN<br />
and also for additional manpower for initial period till the system settles down.<br />
4. Biometric Attendance System : Biometric Attendance System is introduced in the<br />
state. Initially, all the offices from State to District level are covered and then the<br />
Hospitals are covered. Now, it is proposed to cover all the Primary Health Centers in<br />
the state. This activity is separately mentioned in next chapter.<br />
Budget requirement<br />
As mentioned above, budget is required for procurement of software, hardware and<br />
manpower. Budget required for each of the software system is as follows:<br />
Table – Budget requirement for E-Governance<br />
Sir Particulars Unit rate<br />
No. of<br />
units<br />
Rs. In Lakhs<br />
Budget<br />
required<br />
A Expansion of E-Office in State Offices<br />
1 Payment to NIC for software 20 1 20<br />
2 Procurement of Computers 0.4 214 85.6<br />
3 Procurement of Scanners 0.8 36 28.8<br />
4 Lan system 2 8 16<br />
5 Internet connectivity 1.2 6 7.2<br />
Page | 103
Sir Particulars Unit rate<br />
No. of<br />
units<br />
Budget<br />
required<br />
6 Computer specialist (one for one building) 2.64 6 15.84<br />
7 Overheads 2 6 12<br />
Total 185.44<br />
B<br />
Establishment<br />
Software<br />
and Expansion of Hospital<br />
1 Payment to 'Maha Online for Software 300 1 300<br />
2 Procurement of Computers 0.4 1240 496<br />
4 Lan system 5 23 115<br />
5 Internet connectivity 1.2 23 27.6<br />
6 Manpower 2.64 6 15.84<br />
7 DEO (4/hospital) (92) 1.2 92 110.4<br />
8 Pharmacy Officer (2/Hospital) (46) 1.2 92 110.4<br />
9 Overheads 1 23 23<br />
C<br />
Total 1198.24<br />
Other E-projects that will come up during <strong>2012</strong>-<br />
<strong>13</strong><br />
10 5 50<br />
Grand Total 1433.68<br />
B.18.7.4 : Strengthening Of Supervision And Monitoring System<br />
The state has established the Health Management Information system for easy monitoring<br />
and data retrieval. This helps in Monitoring and supportive supervision of <strong>health</strong><br />
institutions. Such an attempt to automate the records of <strong>health</strong> institutions would help, in<br />
the long run, to reduce the workload of maintaining physical records and in compilation and<br />
collation of data generated. This would also facilitate timely reporting of data as well as<br />
analysis and interpretation of various data generated. In the future, such an initiative can<br />
pave way for attempting emerging trends in medicine like telemedicine.<br />
Support is required to establish and maintain the E-Governance system which is submitted<br />
in this chapter.<br />
Plan of action<br />
It is also proposed to support the program offices directly involved in the NRHM activities.<br />
Six old and three new important Disease Control Programs get funds as per PIP. However<br />
some program offices such as Nursing, Hospitals, Primary <strong>health</strong> institutions actually<br />
implement important activities of program but are not directly provided funds. Therefore it<br />
is proposed to provide funds to these institutions along with the peripheral <strong>health</strong><br />
institutions.<br />
As discussed during 6-8 meeting, requirement of DEO and districts is deductd and revised<br />
budget is proposd as follows:<br />
Page | 104
Budget requirement<br />
Budget is required for establishment of Computer Laboratory, internet facility, salary of<br />
support staff required for supervision provided to the program officers and related facilities<br />
to all the concerned Program Officers at state level.<br />
Budget required for this purpose is as follows:<br />
Table – : Budget requirement for strengthening MIS and supervision<br />
Rs. In Lakhs<br />
Sir Particulars Unit cost<br />
No. of<br />
units<br />
Budget<br />
required<br />
Replacement of old computers and<br />
1 maintenance of existing computers in all<br />
the State level offices<br />
12 8 96<br />
2<br />
Procurement of Heavy Duty Printers (2 per<br />
office<br />
0.3 8 2.4<br />
3 LAN System 2 8 16<br />
4 Civil Works 5 8 40<br />
5 Support to program offices 6 8 48<br />
6 Support to MIS section of Directorate 18 1 18<br />
Total 220.4<br />
B.20 : RESEARCH, STUDIES AND ANALYSIS<br />
Two operational research topics of operational research importance are submitted for<br />
approval. National Rural Health Mission, Directorate of Health Services and Senior Faculty of<br />
Medical Colleges are involved in these research projects. Detailed description of the projects<br />
is as follows :<br />
The research studies submitted in this chapter are proposed by the teams in which retired<br />
Vice Chancellor of Maharashtra University of Health Sciences, retired Professors and Deans<br />
and also Directors of Research Institutes are included. Remarks on these researches were<br />
shown to the team. The team has opined that, these studies are Maharashtra specific and<br />
they will definitely benefit for identifying high risk infants and their management.<br />
Considering this, it is proposed to sanction these studies.<br />
SUBSECTION - B.21.1 : PACKAGE OF NEONATAL CARE BY ASHA (PNC BY ASHA)<br />
Activity not approved by GoI. Decision accepted.<br />
SUBSECTION - B.21.2 : MULTICENTRIC BIRTH COHORT TO STUDY THE ANTHROPOMETRIC<br />
MEASUREMENTS OF CHILDREN IN MAHARASHTRA AND THEIR SOCIOEDMOGRAPHIC<br />
CORRELATES<br />
Remarks of ROP : Not approved. A similar study is being undertaken by AIIMS with support<br />
from IAP and WHO. Also any recommendations regarding MUAC cut-offs for diagnosis of<br />
Page | 105
SAM will uniform at National Level. Till then the values provided by WHO are to be used in<br />
the National Program. Therefore, the results from the National Level Study may be awaited.<br />
Explanation of authors to the remarks is as follows:<br />
Multicenter birth cohort from Maharashtra will be undertaken with a view to get<br />
assessment of infants & children from Maharashtra, a state with high rates of stunning &<br />
wasting specially in Advasi (Tribal ) region which may not be reflected in other studies.<br />
The study also envisages to cover infants below 6 months wherein current data for<br />
MUAC is not available & not covered by other studies (Like AIIMS & Others). Proposal from<br />
Maharashtra will also study biochemical hormonal & immunological aspects of SAM which<br />
will cover cytokines interleukins.<br />
Besides all this it is important to have many studies all over India, specially of this<br />
nature as one multicentre study from AIIMS may not be able to address each and every<br />
research question. Malnutrition is a priority for the county and 'National Shame'. Any<br />
amount of work is an absolute necessity & need of the hour.<br />
In addition the Hon. High court of Mumbai has asked opinion from experts on the<br />
role of wt. for age vis a vis wt. for height in detection of SAM, MAM, SUW & MUW for<br />
children of Maharashtra as the PIL is filed by NGO activists from Melghat.<br />
In order to answer all these questions academically, operationally, administratively as<br />
also legally, it is crucial to undertake study in Maharashtra as outlined in our proposal.<br />
Aims and Objectives :<br />
Primary -<br />
1)To obtain anthropometric data from infants and children from Maharashtra.<br />
2) To evaluate the utility and diagnostic efficacy of wt for age, wt for ht and MUAC in infants<br />
and children to detect SAM<br />
Secondary -<br />
3) To assess renal, immunological, biochemical and hepatic functions in babies detected to<br />
have malnutrition and correlate anthropometrically.<br />
Methods :<br />
This is a multicentric study that will be conducted in Government Medical College hospitals<br />
and private nursing homes, primary <strong>health</strong> centers, <strong>rural</strong>, sub-district hospitals in various<br />
cities and towns of Maharashtra so as to cover families from varied socio-economic<br />
backgrounds. We shall recruit 10000 women from different wealth quintiles. We will form a<br />
birth cohort recruiting babies after due informed consent of the mothers taken in last<br />
trimester of pregnancy. Along with this longitudinal study a cross sectional study will be<br />
undertaken to study anthropometry of infants of various months as they attend the<br />
Page | 106
immunization clinics of the hospitals. Longitudinal study would be on 1000 infants and 9000<br />
infants from birth to 3 years of age will be studied cross sectionally.<br />
Duration of study :<br />
Data collection - 6 months for cross sectional study. 2 years for longitudinal study. Data<br />
analysis- 3 months, paper writing- 6 months, dissemination- 6 months<br />
Post funding Timeline<br />
Activity 3mths 6 9 12 18 24 36<br />
Meeting of all investigators and CRF development<br />
workshop<br />
+ + +<br />
Recruitment of ROs and ANMs +<br />
Training of Ros and ANMs +<br />
Procurement of equipment +<br />
Piloting of CRF +<br />
Data collection- enrollment, follow-up + +<br />
Data analysis + +<br />
Paper writing +<br />
Dissemination of data +<br />
Sample size- per center and total. For each center, 1000 women from different wealth<br />
quintiles.<br />
Financial Implications –<br />
Non- recurring -<br />
Weighing balance, tapes (MUAC) caliper identical at all centers. Rs.15,000/- per center.<br />
Rs.1,50,000/- at 10 centers.<br />
Recurring –<br />
Travel Rs. 20,000/- per center every year.<br />
Rs. 2,00,000/- for 10 centers for 1 year.<br />
Stationery Rs.1,00,000/- for all the centers<br />
Staff- Research Assistant- (MBBS or MD) nurse or ancillary helper Rs. 20,000/- per<br />
month<br />
Rs.24,00,000/- per year.<br />
Cost for investigations (Chemicals, Lab kits) Rs.10,00,000/-<br />
Contingency Rs.50,000/-<br />
Total Expenditure -<br />
Rs.39,00,000/-<br />
Considering above explanation, it is submitted to approve this study.<br />
Page | 107
Activity approved<br />
B.21 : ESTABLISHMENT AND FUNCTIONING OF SHSRC<br />
SECTION – B.22 : SUPPORT SERVICES<br />
SUBSECTION : B.22.1 : SUPPORT STRENGTHENING NPCB<br />
ACTIVITY : B.22.1.1 : OPERATIONALIZATION OF SUPERSPECIALITY HOSPITAL FOR CHILD<br />
EYE CARE<br />
Activity Approved<br />
ACTIVITY : B.22.1.2 : PROVISION OF HIRED VEHICLES TO OPHTHALMIC SURGEONS FOR<br />
CATARACT OPERATIONS<br />
Activity Approved<br />
ACTIVITY : B.22.1.3 : PROCUREMENT OF OPHTHALMIC EQUIPMENT FOR CATARACT<br />
OPERATIONS<br />
Activity Approved<br />
SUBSECTION : B.22.3 : SUPPORT STRENGTHENING NVBDCP<br />
Approval with changes accepted.<br />
SUBSECTION : B.22.4 : SUPPORT STRENGTHENING RNTCP<br />
Approval with changes accepted.<br />
SUBSECTION : B.23.6 : OTHER NDCP SUPPORT PROGRAMS<br />
ACTIVITY : B.22.6.1 : RENOVATION OF OCCUPATIONAL THERAPY AND KITCHEN<br />
DEPARTMENT IN 4 REGIONAL MENTAL HOSPITALS – 2 nd PHASE<br />
Approved<br />
ACTIVITY : B.22.6.2 : LEPTOSPIROSIS PREVENTION AND CONTROL PROGRAM<br />
Approved<br />
ACTIVITY : B.22.6.3 : PIP FOR STATE BUREAU OF HEALTH INTELLIGENCE AND VITAL<br />
STATISTICS<br />
As per discussion with Hon. AS & MD, proposal is resubmitted.<br />
To strengthen all activities under this bureau, strong monitoring and evaluation is essential.<br />
Considering this aspect PIP for the year <strong>2012</strong>-<strong>13</strong> has been prepared. In this plan emphasis<br />
Page | 108
has been given on training, monitoring and evaluation, publication of various annual reports<br />
and printing of Birth and Death forms, conduction of statistical evaluation studies and<br />
building construction/renovation. Detailed plan of action is furnished below.<br />
1 Printing<br />
1.1 State Level<br />
1.1.1 For printing of annual reports: Civil Registration System , Survey<br />
of Causes of Death and Medical Certification of Causes of Death,<br />
expected expenditure Rs 1 ,00,000 has been proposed.<br />
1.1.2 Survey of causes of Death (Rural) Scheme is being implemented<br />
in one selected village of every primary <strong>health</strong> center. For the<br />
training of MO,ANM,MPW working under this scheme, printing<br />
of training modules and guidelines of the scheme Rs 2,00,000/- is<br />
proposed.<br />
1.1.3 Printing of Registration of Birth and Death Act 1969 booklet is<br />
proposed. Expenditure of Rs 25,000 is expected.<br />
1.2 District Level<br />
1.2.1 Printing of Birth and Death formats, form No 1 Birth reporting<br />
form, form no 2 Death reporting form, form no 3 Still birth<br />
reporting form, monthly summary report of Birth, Death and Still<br />
birth form no 11, 12 and <strong>13</strong> Rs. 32,41,200/- expenditure is<br />
needed.<br />
1.2.2 According to the directives from Government of India,<br />
Standardized birth and death certificates are to be issued to all<br />
<strong>rural</strong> units. For this printing of form no 5 (birth certificate) and<br />
form no 6 (death certificate) RS. 7, 18,880/- is proposed.<br />
1.2.3 Printing of Form no 4 and 4a under Medical Certification of<br />
Causes of Death to be provided to districts is essential for which<br />
Rs. 3,16,680/- is proposed.<br />
1.2.4 SCD scheme is implemented in all the Primary Health Centers.<br />
One village from each Primary Health Centre is selected under<br />
this scheme. Out of 1818 PHCs in the State 18<strong>13</strong> are working<br />
under this scheme. The information on Births, Deaths, Still Births<br />
and Causes of Deaths is collected every month by this office. It is<br />
the responsibility of this office to provide prescribed formats of<br />
reporting to the PHCs. For printing of these forms funds required<br />
budget is Rs. 11, 02,500/-.<br />
Page | 109
2 Monitoring and Evaluation<br />
3 IEC<br />
2.1.1 The data entry of Block level is expected to be done in newly<br />
developed software by NIC Pune. For this purpose new Server for<br />
HIVS Bureau is required. Rs. 5, 00,000/- is the expected<br />
expenditure.<br />
2.1.2 a) Under Survey of causes of Death scheme®, for ascertaining<br />
cause of death, two physician per district will be authorized and<br />
they will be expected to ascertain every cause of death under<br />
this scheme in their district. An honorarium of Rs. 25/- per<br />
physician per death is planned. For this RS. 11, 50,000/-<br />
expenditure is expected.<br />
b) Under SCD scheme Health worker (M/F) are required to visit<br />
fortnightly to the selected village for collecting sign and<br />
symptoms of deceased before death from their relative. Hon. Of<br />
Rs 25/- per death to <strong>health</strong> worker is proposed. For 2300 deaths<br />
under SCD scheme Rs. 5, 75,000 are proposed.<br />
2.1.3 a) Appointment of one programmer is need for NIC developed<br />
software for taking output of various combinations of variables<br />
under civil registration system. Estimated expenditure of Rs 1,<br />
80,000 /- is needed for contractual appointment of one<br />
Computer (software) programmer in the financial year <strong>2012</strong>-<strong>13</strong><br />
for a period of nine months.<br />
2.1.4 Deleted<br />
b) Data entry of Birth and death registration of urban units is<br />
done at State level at HIVS bureau. On an average data entry of<br />
10 lakh urban births and 3.5 lakh urban deaths are expected per<br />
year. As existing staff is not able to complete the data entry in<br />
stipulated additional manpower is required. Hence, appointment<br />
of 10 data entry operators is proposed. For this financial<br />
assistance of Rs. 8, 64,000/- is required for a period of<br />
nine months.<br />
2.1.5 For statistical analysis of Medical Certification of Causes of<br />
Death, software needs to be developed. Rs. 1, 00,000/- is<br />
expected for this purpose.<br />
2.1.6 Deleted<br />
Page | 110
4 Training<br />
3.1.1 IEC plays an important role in giving information to various<br />
provisions under this act to public at large. Coverage of Death<br />
registration appears to be low due to non-registration of deaths<br />
under 6 years of age. Focus of IEC on registration of deaths under<br />
6 years of age is the need of hour. Rs. 6, 60,000/- expenditure is<br />
required for this publicity.<br />
4.1.1 Under civil registration events like Births, Deaths and Still Births<br />
that occur are filled in prescribed forms. On the basis of this<br />
forms various statistical tables are generated which are used for<br />
future planning purpose. NIC, Pune has developed software for<br />
data entry of these forms. Training at block level is proposed for<br />
which an amount of Rs. 3, 76,000/- is required.<br />
4.1.2 To ascertain the causes of death under SCD scheme, training of<br />
three selected / authorized physicians per district is proposed.<br />
For these 4 batches, State level TOT will be conducted. 100<br />
participants will be trained. This will require budget of Rs. 1,<br />
40,000/-.<br />
Total budget required for HIVS is Rs. 102.5 Lakhs<br />
ACTIVITY : B.22.6.4 : IDSP ADDITIONAL BUDGET FROM NRHM MISSION FLEXIPOOL<br />
Approval in ROP accepted<br />
SECTION – B.24 : SPECIAL SCHEMES FOR TRIBAL AND LEFTIST EXTREMISM AFFECTED<br />
AREAS<br />
Maharashtra has 15 tribal districts out of which 5 are sensitive and six are leftist<br />
extremism affected districts. Considering the <strong>health</strong> problems of these areas and nonavailability<br />
of trained staff to provide the <strong>health</strong> services, specific schemes are proposed for<br />
these areas. Schemes in Part –A are related to all the tribal areas of the State. However<br />
more focus is given to districts with remote tribal areas. Part – B of this Section is related to<br />
special schemes and activities proposed for high focus districts namely: Nandurbar, Gondia<br />
and Gadchiroli.<br />
Following schemes are proposed for tribal and leftist extremism areas.<br />
SUB-SECTION – B.24.2 :MAHER SCHEME<br />
Page | 111
Approved<br />
SUB-SECTION – B.24.4 : VOLUNTEER TO TRIBAL AND LEFTIST EXTREMISM AFFECTED PHCS<br />
Approved.<br />
SUB-SECTION – B.24.5. : MOBILITY SUPPORT<br />
Comprehensive plan for mobility support submitted elsewhere<br />
SUB-SECTION – B.24.6 : SOLAR BACK-UP SYSTEM FOR TRIBAL AREAS<br />
Shifted to B.4<br />
SUBSECTION - B.24.8 : ORGANIZATION OF SPECIALIST MEDICAL & DENTAL CAMPS<br />
THROUGH MEDICAL COLLEGES IN TRIBAL HOSPITALS<br />
Approved<br />
SUBSECTION - B.24.9 : PILOT PROJECT TO REDUCE IMR IN MELGHAT REGION (DIST.<br />
AMARAWATI) OF MAHARASHTRA<br />
Activity not approved. Accepted.<br />
SUBSECTION - B.24.10 : COORDINATION CELL FOR TRIBES IN SELECTED LEA & TRIBAL<br />
DISTRICTS HOSPITALS<br />
Approved<br />
SUBSECTION - B.24.11 : INTEGRATION OF PALLIATIVE CARE IN JAWHAR TRIBAL BLOCK DIST<br />
THANE<br />
Remarks of ROP : Approved.<br />
NPCC has approved this activity. However two components of this activity, incentive to<br />
ASHA and post of Medical Officers are not approved. Sub<strong>mission</strong> for reconsideration of<br />
these activities is as follows:<br />
1. Incentives for ASHA workers & other Health Care Provider<br />
Budget proposed was Rs. 2.0 Lakh and not approved. This is important activity and<br />
needs to be continued for effective implementation of program. Important points in this<br />
regard are as follows:<br />
• 232 ASHAs form Jawhar block are trained for providing palliative care to the patient<br />
by experts from Tata Memorial Center, Mumbai in 2011-12.<br />
Page | 112
• ASHA detected and provided palliative care to 164 patients during 2011-12 (ASHA<br />
identified patients were confirmed expert doctor).<br />
• ASHA were provided medicine kits and they were given weekly follow up visits to the<br />
patients.<br />
• ASHA were provided Rs. 50/- on identification and referring each patient to PHC and<br />
Rs. 50/ - more on confirmation by expert doctor.<br />
• ASHA are paid Rs. 25/- for weekly follow up visit to patient.<br />
• Majority of patients registered for palliative care project are bed-ridden and are need<br />
in domiciliary care which on day to day basis ASHA can provide.<br />
• ASHA gets performance based incentives; hence the incentive to ASHA needs to be<br />
approved.<br />
For effective implementation of the project and continuation of the project as in<br />
2011-12, there is a need of additional budget Rs. 2.00 Lakhs for incentives to ASHA .<br />
2. Salary of Contractual Medical Social Worker (Counsellor) & Medical Officer (Budget<br />
required – Rs. 3.5 Lakhs)<br />
Medical Social worker was appointed in June 11 and Medical Officer in November 11.<br />
Salary of MO is Rs. 16000/PM and salary of Medical Social Worker is Rs. 15000/PM.<br />
As these were new appointments, salary was not requested for whole year. However, as<br />
both of them are continued from 1 st April <strong>2012</strong>, requirement of salary for one year even<br />
if it is not increased will be as follows:<br />
Table – Salary of Medical Officer and Medical Social Worker for year <strong>2012</strong>-<strong>13</strong> (at old<br />
rates)<br />
Rs. In Lakhs<br />
Sr Post Monthly salary Budget required for<br />
salary of <strong>2012</strong>-<strong>13</strong><br />
1 Medical Officer 0.16 1.92<br />
2 Medical Social Worker 0.15 1.8<br />
Total 3.72<br />
Table above indicate that budget required for this approved activity is Rs. 3.72 Lakh.<br />
Considering the explanation, GoI is requested to approve Rs. 2.0 lakh for ASHA and Rs.<br />
3.72 lakh for salary of MO and MSW. Accordingly total budget required for this activity<br />
will be now Rs. <strong>13</strong>.72 Lakh.<br />
SUBSECTION – B.24.12 : ESTABLISHMENT OF NUTRITIONAL REHABILITATION CENTERS IN<br />
TRIBAL AND LEA BLOCKS.<br />
Page | 1<strong>13</strong>
Activity not approved. Accepted.<br />
SUBSECTION – B.24.<strong>13</strong> : ESTABLISHMENT OF MEDICINE WAREHOUSE AT SELECTED PLACES<br />
IN TRIBAL AREAS.<br />
Activity not approved. Accepted.<br />
SUB-SECTION –B.24.14: TELEMEDICINE IN TRIBAL AREAS<br />
Not approved. Accepted.<br />
Page | 114