Bifid Condyle: Review of the Literature of the Last 10 Years and ...
Bifid Condyle: Review of the Literature of the Last 10 Years and ...
Bifid Condyle: Review of the Literature of the Last 10 Years and ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
0886-9634/2802-<br />
000$05.00/0, THE<br />
JOURNAL OF<br />
CRANIOMANDIBULAR<br />
PRACTICE,<br />
Copyright © 20<strong>10</strong><br />
by CHROMA, Inc.<br />
Manuscript received<br />
September 23, 2009;<br />
revised<br />
manuscript received<br />
December 3, 2009;<br />
accepted<br />
December 4, 2009<br />
Address for correspondence:<br />
Dr. Raúl Ayuso-Montero<br />
Faculty <strong>of</strong> Dentistry<br />
Dept. <strong>of</strong> Prosthodontics<br />
University <strong>of</strong> Barcelona<br />
Campus de Bellvitge<br />
C/Feixa Llarga s/n<br />
L’Hospitalet de Llobregat<br />
Barcelona E-08907<br />
Spain<br />
E-mail: raulayuso@ub.edu<br />
■ CASE REPORTS<br />
<strong>Bifid</strong> <strong>Condyle</strong>: <strong>Review</strong> <strong>of</strong> <strong>the</strong> <strong>Literature</strong> <strong>of</strong> <strong>the</strong> <strong>Last</strong> <strong>10</strong><br />
<strong>Years</strong> <strong>and</strong> Report <strong>of</strong> Two Cases<br />
José López-López, M.D., Ph.D.; Raúl Ayuso-Montero, D.D.S., Ph.D.;<br />
Enric Jané Salas, M.D., Ph.D.; Xavier Roselló-Llabrés, M.D., Ph.D.<br />
<strong>Bifid</strong> m<strong>and</strong>ibular condyle is a rare anomaly; <strong>the</strong>re are several <strong>the</strong>ories about its etiology, <strong>and</strong> it has been<br />
studied in both prehistoric <strong>and</strong> historic skulls, as well as in living human beings. It is a frequent, although<br />
unexpected, finding in asymptomatic individuals during radiological treatment. Presented here is a<br />
review <strong>of</strong> <strong>the</strong> literature over <strong>the</strong> past <strong>10</strong> years <strong>and</strong> two new cases <strong>of</strong> unilateral bifid condyle.<br />
Computerized tomography is usually considered <strong>the</strong> test <strong>of</strong> choice for establishing <strong>the</strong> differential diagnosis,<br />
although in certain cases, its use seems questionable. The distinction between bifid condyle <strong>and</strong><br />
condylar notch or cleft has been described in <strong>the</strong> literature, it is proposed a criteria for defining bifid<br />
condyle depending on <strong>the</strong> level <strong>of</strong> <strong>the</strong> two heads. It is suggested that fur<strong>the</strong>r testing such as MRI or CT<br />
be carried out only in cases where <strong>the</strong> <strong>the</strong>rapeutic approach involves an active treatment. It is proposed<br />
that bifid condyle is described as that which presents two condylar heads emerging from <strong>the</strong> neck <strong>of</strong> <strong>the</strong><br />
condyle or fur<strong>the</strong>r down.<br />
Dr. José Lopéz-Lopéz has a M.D. degree<br />
from Autonoma <strong>of</strong> Barcelona University,<br />
Spain <strong>and</strong> a Ph.D. from <strong>the</strong> University <strong>of</strong><br />
Barcelona. He is a full pr<strong>of</strong>essor <strong>of</strong> oral<br />
medicine in <strong>the</strong> Department <strong>of</strong> Dentistry<br />
at <strong>the</strong> University <strong>of</strong> Barcelona. Dr. Lopéz-<br />
Lopéz also has received master’s degrees<br />
in implantology from <strong>the</strong> University <strong>of</strong><br />
Sevilla <strong>and</strong> oral pathology from <strong>the</strong><br />
University <strong>of</strong> Barcelona.<br />
1<br />
The term bifid condyle has been described as a condition<br />
<strong>of</strong> unknown etiology <strong>and</strong> uncertain pathogenesis.<br />
1,2 Duplication <strong>of</strong> <strong>the</strong> m<strong>and</strong>ibular condyle<br />
is rare <strong>and</strong> has been studied both in prehistoric <strong>and</strong> historic<br />
skulls, 2,3 as well as in living human beings. 4-<strong>10</strong> It is a<br />
rare <strong>and</strong> unexpected radiologic finding in asymptomatic<br />
individuals. 4,5,8-<strong>10</strong> O<strong>the</strong>r cases occur with functional ankylosis<br />
<strong>of</strong> one or both temporom<strong>and</strong>ibular joints (TMJ). 11,12<br />
Different authors describe bifid condyle as a result <strong>of</strong><br />
trauma (application <strong>of</strong> forceps during birth, 11 condylar<br />
fracture by accident, 1,6,13-15 surgical condylectomy). This<br />
<strong>the</strong>ory is based on <strong>the</strong> fact that after a condylar neck fracture,<br />
an antero-medial displacement <strong>of</strong> <strong>the</strong> condyle takes<br />
place due to <strong>the</strong> action <strong>of</strong> <strong>the</strong> external pterygoid muscle,<br />
such that it produces a metaplasia <strong>of</strong> <strong>the</strong> local fibroblasts<br />
in <strong>the</strong> condylar neck, which in turn develops a new<br />
condylar head in <strong>the</strong> normal anatomic location, while <strong>the</strong><br />
displaced condyle begins a resorption process. Thus, for a<br />
time, two or more condyles 14 or a double condyle on one<br />
side <strong>and</strong> a triple condyle on <strong>the</strong> o<strong>the</strong>r side may be present.<br />
15 In <strong>the</strong>se cases, one <strong>of</strong> <strong>the</strong> condyles (anterior) does<br />
not function <strong>and</strong> one <strong>of</strong> <strong>the</strong>m (posterior) does.
BIFID CONDYLE LOPEZ-LOPEZ ET AL.<br />
O<strong>the</strong>r authors support <strong>the</strong> <strong>the</strong>ory that bifid condyle is<br />
an embryological malformation. When <strong>the</strong> fetus is about<br />
20 weeks old, a septum <strong>of</strong> vascular fibers appears in <strong>the</strong><br />
cartilage <strong>of</strong> <strong>the</strong> condyle, extending all <strong>the</strong> way to <strong>the</strong> interior<br />
<strong>of</strong> <strong>the</strong> bone. This septum disappears at about <strong>the</strong> nineteenth<br />
week <strong>of</strong> life, such that if one suffers an injury or<br />
<strong>the</strong>re continues to be a shortage <strong>of</strong> blood supply, it may<br />
affect <strong>the</strong> proper ossification <strong>of</strong> <strong>the</strong> condyle <strong>and</strong> end up<br />
producing a bifid condyle. 7,9<br />
Surgery is usually indicated only in cases <strong>of</strong> condylar<br />
ankylosis 13 or when <strong>the</strong>re is significant pain when chewing,<br />
16 which is usually secondary to trauma. Displaced<br />
articular disks, causing pain <strong>and</strong>/or dysfunction may also<br />
be an indication for surgery. As for cases, which are<br />
asymptomatic or <strong>the</strong>re is mild temporom<strong>and</strong>ibular dysfunction,<br />
<strong>the</strong> treatment is usually conservative. Computerized<br />
tomography is most <strong>of</strong>ten considered <strong>the</strong> test <strong>of</strong><br />
choice for establishing <strong>the</strong> differential diagnosis. 17<br />
Some authors have documented cases with additional<br />
tests such as Panoramic Radiograph (PR), 4,18 Computerized<br />
Tomography (CT), 6,8,<strong>10</strong>-11,13-15 Magnetic Resonance<br />
Imaging (MRI), 1,5,9 <strong>and</strong> as aforementioned, <strong>the</strong>y are <strong>of</strong>ten<br />
cases in which <strong>the</strong> patient is asymptomatic <strong>and</strong> <strong>the</strong><br />
condyle is functioning normally when <strong>the</strong> diagnosis is<br />
made unexpectedly. In addition, <strong>the</strong> <strong>the</strong>rapeutic approach<br />
does not vary depending on <strong>the</strong> results <strong>of</strong> <strong>the</strong> additional<br />
tests. In this sense, it seems reasonable to question <strong>the</strong><br />
need for fur<strong>the</strong>r tests that are invasive <strong>and</strong> do not alter <strong>the</strong><br />
treatment.<br />
Dennison 2 suggests that <strong>the</strong> term bifid condyle should<br />
only be reserved for cases in which <strong>the</strong>y appear both in<br />
<strong>the</strong> anterior <strong>and</strong> posterior part <strong>of</strong> <strong>the</strong> sagittal plane, suggesting<br />
that <strong>the</strong> rest <strong>of</strong> <strong>the</strong> cases should be classified as a<br />
cleft, notch, or gap, thus considering <strong>the</strong>m to be false<br />
bifid condyles. This study presents two new cases <strong>of</strong> unilateral<br />
bifid condyle.<br />
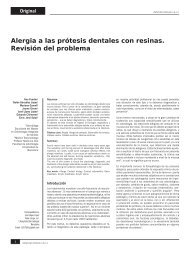
Clinical Case No. 1<br />
Case number one is a female patient aged 70 years,<br />
who requested oral rehabilitation, <strong>and</strong> had not been clinically<br />
diagnosed with temporom<strong>and</strong>ibular dysfunction<br />
(TMD). She had normal opening (Figure 1) without<br />
signs or symptoms in <strong>the</strong> joints or muscles. During <strong>the</strong><br />
radiological testing (PR) for treatment planning, <strong>the</strong><br />
image showed a double contour <strong>of</strong> <strong>the</strong> condyle (Figure<br />
2), which can be seen in <strong>the</strong> left temporom<strong>and</strong>ibular joint<br />
(TMJ). In <strong>the</strong> medical history, <strong>the</strong> patient reported childhood<br />
trauma on that side <strong>of</strong> <strong>the</strong> face, which resulted in<br />
not being able to open <strong>the</strong> mouth for several days. The<br />
<strong>the</strong>rapeutic approach was <strong>the</strong> prosthodontic rehabilitation<br />
<strong>of</strong> <strong>the</strong> patient without active <strong>the</strong>rapeutic treatment <strong>of</strong><br />
<strong>the</strong> TMJ.<br />
Figure 1<br />
Clinical case No. 1: Normal mouth opening.<br />
Clinical Case No. 2<br />
Case number two is a female patient aged 53 years who<br />
was referred by a general dentist for TMJ evaluation. The<br />
patient presented discomfort in <strong>the</strong> jaw when waking up<br />
in <strong>the</strong> morning. The clinical evaluation revealed a displacement<br />
<strong>of</strong> seven mm in <strong>the</strong> opening on <strong>the</strong> right side <strong>of</strong><br />
Figure 2<br />
Clinical case No. 1: Detail <strong>of</strong> <strong>the</strong> double contour <strong>of</strong> <strong>the</strong> left TMJ<br />
condyle. The emergence <strong>of</strong> <strong>the</strong> second head can be observed beneath<br />
<strong>the</strong> neck <strong>of</strong> <strong>the</strong> larger condyle.<br />
2 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE APRIL 20<strong>10</strong>, VOL. 28, NO. 2
LOPEZ-LOPEZ ET AL. BIFID CONDYLE<br />
Figure 3<br />
Clinical case No. 2: Displacement seven mm to <strong>the</strong> right at maximum<br />
opening.<br />
<strong>the</strong> mouth (Figure 3), normal lateralities, stiff end-feel,<br />
<strong>and</strong> positive muscle palpation on <strong>the</strong> right <strong>and</strong> left external<br />
pterygoid, insertion <strong>of</strong> <strong>the</strong> right <strong>and</strong> left temporal, <strong>and</strong><br />
left masseter muscles. The PR revealed <strong>the</strong> left mediolateral<br />
double contour <strong>of</strong> <strong>the</strong> condyle (Figure 4). The <strong>the</strong>rapeutic<br />
approach was conservative, making a splint that<br />
would provide decompression <strong>of</strong> <strong>the</strong> joints <strong>and</strong> relaxation<br />
<strong>of</strong> <strong>the</strong> muscles. The patient was seen for a checkup after<br />
Figure 4<br />
Clinical case No. 2: The panoramic radiograph revealed <strong>the</strong> left mediolateral<br />
double contour <strong>of</strong> <strong>the</strong> condyle.<br />
six months, <strong>and</strong> progress was observed to be favorable.<br />
Discussion<br />
In <strong>the</strong> last ten years, we have found 30 cases <strong>of</strong> bifid<br />
condyle referenced in <strong>the</strong> literature (Table 1). It is an<br />
unexpected finding in routine checkups such as <strong>the</strong> PR,<br />
which is <strong>the</strong> most common way it is diagnosed. That is,<br />
most patients who are diagnosed are asymptomatic <strong>and</strong><br />
have normal joint function. 4,5,8-<strong>10</strong> In <strong>the</strong>se types <strong>of</strong> patients,<br />
<strong>the</strong> case is <strong>of</strong>ten documented with supporting tests such<br />
as a CT, MRI, or both, 1,5-6, 8-<strong>10</strong>,12-15 although <strong>the</strong> usefulness<br />
<strong>of</strong> conducting such tests is questionable, since <strong>the</strong>y<br />
involve a financial <strong>and</strong> time commitment on <strong>the</strong> part <strong>of</strong><br />
<strong>the</strong> patient whose prognosis is not going to change.<br />
(Moreover, in <strong>the</strong> case <strong>of</strong> <strong>the</strong> CT, <strong>the</strong> patient receives<br />
radiation.) However, <strong>the</strong> diagnostic orientation <strong>and</strong><br />
<strong>the</strong>rapeutic treatment in patients who show symptoms<br />
or who have abnormal function may justify performing<br />
such tests.<br />
However, <strong>the</strong> designation <strong>of</strong> bifid condyle has also<br />
been discussed, <strong>and</strong> it has been proposed to reserve <strong>the</strong><br />
name exclusively for antero-posterior cases while considering<br />
<strong>the</strong> rest to be false bifid condyles. 2 In this sense, it<br />
would be advisable to analyze each case in order to determine<br />
if it corresponds to a gap or if it is an actual bifid<br />
condyle, given that it does not seem reasonable to set <strong>the</strong><br />
criteria according to which direction <strong>the</strong> condylar heads<br />
are facing. It could be <strong>the</strong> case that <strong>the</strong> central split <strong>of</strong> <strong>the</strong><br />
condyle was so deep that it exceeded <strong>the</strong> entire condyle,<br />
actually presenting two condylar heads in <strong>the</strong> lateromedial<br />
direction, 6-7,13 with subsequent adjustment <strong>of</strong> <strong>the</strong><br />
remaining joint structures (menisci, muscular insertions,<br />
ligaments <strong>and</strong> glenoid cavity).<br />
For this reason, <strong>and</strong> in an effort to simplify <strong>the</strong> terminology,<br />
it is proposed that <strong>the</strong> criteria for defining bifid<br />
condyle be determined according to whe<strong>the</strong>r or not <strong>the</strong><br />
condylar heads emerge from <strong>the</strong> neck <strong>of</strong> <strong>the</strong> condyle or<br />
fur<strong>the</strong>r down, regardless <strong>of</strong> <strong>the</strong> spatial orientation, given<br />
that functionally speaking <strong>the</strong>y should be considered in<br />
<strong>the</strong> same manner.<br />
Conclusions<br />
It is suggested that fur<strong>the</strong>r tests, such as MRI or CT, be<br />
carried out only in cases where <strong>the</strong> <strong>the</strong>rapeutic approach<br />
involves an active treatment.<br />
In order to simplify <strong>the</strong> terminology used, it is proposed<br />
that bifid condyle is described as that which presents<br />
two condylar heads emerging from <strong>the</strong> neck <strong>of</strong> <strong>the</strong><br />
condyle or fur<strong>the</strong>r down, regardless <strong>of</strong> <strong>the</strong> direction in<br />
which <strong>the</strong>y are facing.<br />
APRIL 20<strong>10</strong>, VOL. 28, NO. 2 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE 3
BIFID CONDYLE LOPEZ-LOPEZ ET AL.<br />
Table 1<br />
Thirty (30) <strong>Bifid</strong> <strong>Condyle</strong>s Documented in <strong>the</strong> <strong>Literature</strong> Over <strong>the</strong> Past <strong>10</strong> <strong>Years</strong> in Living Humans<br />
No. <strong>of</strong> patients/ Gender/ No. <strong>of</strong> Additional<br />
author med. record Age condyles Orientation Impact Clinical tests<br />
1/Acikgoz Female 54 2 Mediolateral Bilateral Asymptomatic PR, CT<br />
1/Alpaslan Male 40 2 Mediolateral Bilateral Asymptomatic PR, CT, MRI<br />
discovery <strong>of</strong><br />
anterior disk<br />
displacement<br />
w/o reduction<br />
1/Antoniades Male 15 2 right Medial, central Bilateral Opening limited PR, CT<br />
T 3 left <strong>and</strong> lateral 24 mm, no flares<br />
1/Artvinli Female 25 3 Medial, central Left Asymptomatic PR, CT<br />
T <strong>and</strong> lateral<br />
1/Corchero Female 42 2 Anteroposterior Left Reciprocal click, PR, CT, MRI<br />
lateral displacement<br />
to <strong>the</strong> left<br />
protrusion <strong>10</strong> mm<br />
1/Daniels Male 32 2 Mediolateral Right Displacement to PR, CT<br />
T <strong>the</strong> right, limited<br />
opening, protrusion<br />
9 mm<br />
1/De Sales Male 8 2 Mediolateral Right Displacement to PR, CT<br />
T <strong>the</strong> right<br />
1/Espinosa Male 29 2 Mediolateral Bilateral Asymptomatic PR, CT, MRI<br />
1/Hersek Female 36 2 Anteroposterior Left Facial asymmetry,<br />
T limit lat. right <strong>and</strong><br />
protrusion, click left<br />
9/Menezes Female 28 2 Left Asymptomatic PR (all)<br />
Male 30 Left CT (two)<br />
Female 74 Bilateral Transcranial (1)<br />
Female 20 Left<br />
Male 43 Bilateral<br />
Female 53 Right<br />
Female 72 Left<br />
Female 52 Right<br />
Female 29 Right<br />
1/Moraes Female 20 2 Mediolateral Left Asymptomatic PR, MRI,<br />
Rx TMJ<br />
<strong>10</strong>/Rehman Male T 9 2 Anteroposterior Bilateral Ankylosis CT<br />
Female T 6 Anteroposterior Bilateral Ankylosis<br />
Male T 26 Mediolateral Bilateral Ankylosis<br />
Female T 8 Mediolateral Bilateral Ankylosis<br />
Male T 16 Mediolateral Right Ankylosis<br />
Female T 38 Mediolateral Right Ankylosis<br />
Female T 5 Mediolateral Left Ankylosis<br />
Male T 44 Mediolateral Right Ankylosis<br />
Female T 7 Mediolateral Right Ankylosis<br />
Male I 20 Mediolateral Left Ankylosis<br />
1/Sales Female 8 2 Mediolateral Left Ankylosis CT<br />
2/Shiriki Female 45 2 Mediolateal Right Headache, clicks CT, MRI<br />
Female M 17 2 Mediolateral Left Asymptomatic<br />
4/Stefanou Female 55 2 Mediolateral Bilateral Asymptomatic PR, Rx TMJ<br />
Male 47 2 Mediolateral Bilateral Asymptomatic PR, Rx TMJ<br />
Female 39 2 Mediolateral Bilateral Asymptomatic PR, Rx TMJ<br />
Female 69 2 Mediolateral Bilateral Asymptomatic Rx TMJ<br />
1/Tunçbilek Male T 8 2 Mediolateral Left Asymptomatic PR, CT<br />
T: trauma; I: infection; M: microtia, PR: panoramic radiograph; CT: computerized tomography; MRI: magnetic resonance<br />
imaging; Rx TMJ: lateral radiograph <strong>of</strong> TMJ<br />
4 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE APRIL 20<strong>10</strong>, VOL. 28, NO. 2
LOPEZ-LOPEZ ET AL. BIFID CONDYLE<br />
References<br />
1. Hersek N, Özbeck M, Tasar F, et al.: <strong>Bifid</strong> m<strong>and</strong>ibular condyle: a case report.<br />
Dent Traumatol 2004; 20:184-186.<br />
2. Dennison J, Mahoney P, Herbison P, Dias G: The false <strong>and</strong> <strong>the</strong> true bifid<br />
condyles. HOMO, J Comp Human Biol 2008; 59:149-159.<br />
3. Jordana X, García C, Palacios M, Chimenos E, Malgosa A: <strong>Bifid</strong> m<strong>and</strong>ibular<br />
condyle: archaeological case report <strong>of</strong> a rare anomaly. Dentomaxill<strong>of</strong>ac<br />
Radiol 2004; 33:278–281.<br />
4. Stefanou EP, Fanourakis IG, Vlastos K, Katerelou J: Bilateral bifid m<strong>and</strong>ibular<br />
condyles. Report <strong>of</strong> four cases. Dentomaxill<strong>of</strong>ac Radiol 1998; 27:186-<br />
188.<br />
5. Alpaslan S, Özbek M, Hersek N, et al.: Bilateral bifid m<strong>and</strong>ibular condyle.<br />
Dentomaxill<strong>of</strong>ac Radiol 2004; 33:274-277.<br />
6. De Sales MA, Amaral JI, Fern<strong>and</strong>es R, Almeida R: <strong>Bifid</strong> m<strong>and</strong>ibular<br />
condyle: case report <strong>and</strong> etiological considerations. Can Dent Assoc 2004;<br />
70:158-162.<br />
7. Shriki J, Lev R, Wong B, Sundine MJ, Hasso A. <strong>Bifid</strong> m<strong>and</strong>ibular condyle:<br />
CT <strong>and</strong> MR imaging appearance in two patients: case report <strong>and</strong> review <strong>of</strong><br />
<strong>the</strong> literature. Am J Neuro Radiol 2005; 26:1865-1868.<br />
8. Açikgöz A: Bilateral bifid m<strong>and</strong>ibular condyle: a case report. J Oral Rehabil<br />
2006; 33:784-787.<br />
9. Espinosa-Femenia M, Satorres-Nieto M, Berini-Aytés L, Gay-Escoda C:<br />
Bilateral bifid m<strong>and</strong>ibular condyle. Report <strong>of</strong> a case <strong>and</strong> review <strong>of</strong> <strong>the</strong> literature.<br />
J Craniom<strong>and</strong>ib Pract 2006; 24:137-140.<br />
<strong>10</strong>. Sales MA, Oliveira JX, Cavalcanti MG: Computed tomography imaging<br />
findings <strong>of</strong> simultaneous bifid m<strong>and</strong>ibular condyle <strong>and</strong> temporom<strong>and</strong>ibular<br />
joint ankylosis: case report. Braz Dent J 2007; 18:74-77.<br />
11. Rehman TA, Gibikote S, Ilango N, Thaj J, Sarawagi R, Gupta A: <strong>Bifid</strong><br />
m<strong>and</strong>ibular condyle with associated temporom<strong>and</strong>ibular joint ankylosis: a<br />
computed tomography study <strong>of</strong> <strong>the</strong> patterns <strong>and</strong> morphological variations.<br />
Dentomaxill<strong>of</strong>ac Radiol 2009; 38:239-244.<br />
12. Moraes F, Vasconcelos J, Manzi F, Bóscolo F, Almeida S: <strong>Bifid</strong> m<strong>and</strong>ibular<br />
condyle: a case report. J Oral Sci 2006; 48:35-37.<br />
13. Daniels J, Ali I: Post-traumatic bifid condyle associated with temporom<strong>and</strong>ibular<br />
joint ankylosis: Report <strong>of</strong> a case <strong>and</strong> review <strong>of</strong> <strong>the</strong> literature.<br />
Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005; 99:682-688.<br />
14. Artvinli L, Kansu Ö. Trifid m<strong>and</strong>ibular condyle: a case report. Oral Surg Oral<br />
Med Oral Pathol Oral Radiol Endod 2003; 95:251-254.<br />
15. Antoniades K, Hadjipetrou L, Antoniades V, Paraskevopoulos K: Bilateral<br />
bifid m<strong>and</strong>ibular condyle. Oral Surg Oral Med Oral Pathol Oral Radiol<br />
Endod 2004; 97:535-538.<br />
16. Tunçbilek G, Çavdar G, Mavili E. <strong>Bifid</strong> m<strong>and</strong>ibular condyle: a rare disorder.<br />
J Crani<strong>of</strong>ac Surg 2006; 17:1207-1209.<br />
17. Corchero G, Gonzalez T, García MF, Sánchez S, Saiz R: Cóndilo bífido: a<br />
propósito de un caso. Med Oral Patol Oral Cir Bucal 2005; <strong>10</strong>:277-279.<br />
18. Menezes, Moraes FM, Vasconcelos J, Kurita LM, Almeida SM, Haiter-Neto<br />
F: The prevalence <strong>of</strong> bifid m<strong>and</strong>ibular condyle detected in a Brazilian population.<br />
Dentomaxill<strong>of</strong>ac Radiol 2008; 37:220-223.<br />
Dr. Raúl Ayuso Montero received a D.D.S. <strong>and</strong> Ph.D. degrees from <strong>the</strong><br />
University <strong>of</strong> Barcelona, Spain. He also has master’s degrees in prosthodontics<br />
from <strong>the</strong> same university <strong>and</strong> implantology from <strong>the</strong> University <strong>of</strong><br />
Sevilla. Dr. Montero is a pr<strong>of</strong>essor <strong>of</strong> prosthodontic medicine in <strong>the</strong><br />
Department <strong>of</strong> Dentistry at <strong>the</strong> University <strong>of</strong> Barcelona.<br />
Dr. Enric Jané Salas received an M.D. degree from Autonoma <strong>of</strong><br />
Barcelona, University <strong>of</strong> Barcelona, Spain <strong>and</strong> a Ph.D. from <strong>the</strong><br />
University <strong>of</strong> Barcelona. He also has a master’s degree in endodontics<br />
from <strong>the</strong> same university. Dr. Salas is a pr<strong>of</strong>essor <strong>of</strong> oral medicine in <strong>the</strong><br />
Department <strong>of</strong> Dentistry at <strong>the</strong> University <strong>of</strong> Barcelona.<br />
Dr. Xavier Roselló-Llabrés received an M.D. degree from Autonoma <strong>of</strong><br />
Barcelona, University <strong>of</strong> Barcelona, Spain <strong>and</strong> a Ph.D. from <strong>the</strong><br />
University <strong>of</strong> Barcelona. He is a pr<strong>of</strong>essor <strong>of</strong> oral medicine in <strong>the</strong><br />
Department <strong>of</strong> Dentistry at <strong>the</strong> University <strong>of</strong> Barcelona.<br />
APRIL 20<strong>10</strong>, VOL. 28, NO. 2 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE 5