Case 22-2004: A 30-Year-Old Woman with a Pericardial Effusion
Case 22-2004: A 30-Year-Old Woman with a Pericardial Effusion
Case 22-2004: A 30-Year-Old Woman with a Pericardial Effusion

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
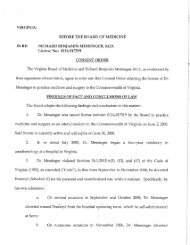
Table 2. Causes of Pericarditis.<br />
Cause<br />
284<br />
The causes of pericarditis vary among populations.<br />
In a general hospitalized population, unselected<br />
cases of pericarditis are predominantly idiopathic<br />
or due to cancer (Table 2), 7 and the diagnostic<br />
yield of pericardiocentesis is low in the absence of<br />
tamponade or signs of infection.<br />
The new england journal of medicine<br />
9-11<br />
In contrast,<br />
among patients admitted to a university tertiary-care<br />
center <strong>with</strong> new, large, symptomatic pericardial effusions,<br />
infectious causes predominate, followed by<br />
a malignant condition and radiation-induced pericarditis.<br />
8<br />
noninfectious causes of pericarditis<br />
Among noninfectious causes of pericarditis, tumors<br />
are most common, <strong>with</strong> lung cancer, breast cancer,<br />
and Hodgkin’s disease heading the long list of possibilities.<br />
Given this patient’s mediastinal lymphadenopathy,<br />
it is important to consider cancer, especially<br />
lymphoma. Factors that argue against this<br />
diagnosis are the absence of a known primary tumor,<br />
the negative results of the cytologic evaluation<br />
of the pericardial fluid, and the negative results of<br />
examination of the bronchoscopic washings and<br />
the transbronchial needle–biopsy specimen. A pericardial<br />
biopsy performed at the time of the pericardiocentesis<br />
would have been useful for ruling out<br />
cancer and certain other diagnoses.<br />
Several noninfectious, inflammatory causes of<br />
pericarditis — radiation therapy, drugs, myocardial<br />
infarction, and metabolic factors — are not supported<br />
by the clinical history. Remaining are the collagen<br />
vascular diseases and sarcoidosis. Almost all of the<br />
Echocardiogram<br />
Series* Large New <strong>Effusion</strong>s†<br />
percent of patients<br />
Infectious — 27<br />
Acute idiopathic 20 —<br />
Iatrogenic 16 14 (radiation therapy)<br />
Malignant 13 23<br />
Chronic idiopathic 9 7<br />
Associated <strong>with</strong> preceding acute<br />
myocardial infarction<br />
8 —<br />
Associated <strong>with</strong> uremia or dialysis 6 12<br />
Associated <strong>with</strong> cardiovascular<br />
disease<br />
5 12<br />
* The data are from Sagrista-Sauleda et al. 7 and reflect findings in 3<strong>22</strong> patients.<br />
† The data are from Corey et al. 8 and reflect findings in 75 patients.<br />
n engl j med 351;3<br />
collagen vascular diseases have been associated <strong>with</strong><br />
pericarditis, but systemic lupus erythematosus and<br />
rheumatoid arthritis are the most common causes.<br />
The prevalence of collagen vascular diseases is increased<br />
among young women, such as this patient.<br />
Although pericardial disease is said to be the most<br />
common cause of symptomatic cardiac involvement<br />
in lupus, most pericardial effusions in patients <strong>with</strong><br />
lupus are small and asymptomatic and are associated<br />
<strong>with</strong> a polyserositis and a pericardial friction<br />
rub on examination. In one study, pericardial effusion<br />
was seen in 19 percent of patients and tamponade<br />
in 2.5 percent, and it was the initial presentation<br />
in 1 percent.<br />
12<br />
www.nejm.org july 15,<br />
<strong>2004</strong><br />
Mediastinal lymphadenopathy can<br />
occur in lupus, but nodular lung infiltrates are not<br />
consistent <strong>with</strong> a diagnosis of lupus. The low titer<br />
of antinuclear antibodies and the negative test for<br />
double-stranded DNA also make such a diagnosis<br />
unlikely. In one study of complications of rheumatoid<br />
arthritis, only 1.25 percent of patients <strong>with</strong> the<br />
disease had pericarditis<br />
13<br />
and 0.5 percent had tam-<br />
ponade. Furthermore, pericarditis occurs late in the<br />
course of rheumatoid arthritis. This patient had no<br />
joint symptoms, and a test for rheumatoid factor<br />
was negative. Still’s disease in adults has been associated<br />
<strong>with</strong> pericarditis, and tests for both antinuclear<br />
antibodies and rheumatoid factor are usually<br />
negative, but this patient did not have the high<br />
fever, polyarthralgias, rash, leukocytosis, abnormal<br />
aminotransferase levels, and elevated serum ferritin<br />
levels that are characteristic of that disease.<br />
Sarcoidosis can cause mediastinal lymphadenopathy<br />
and commonly affects the heart, causing<br />
arrhythmias, conduction abnormalities, heart failure,<br />
and pericardial disease. <strong>Pericardial</strong> involvement<br />
is rare,<br />
15<br />
but tamponade has been reported.<br />
14<br />
16<br />
The<br />
level of angiotensin-converting enzyme was normal<br />
in the patient under discussion.<br />
infectious causes of pericarditis<br />
This process of elimination leads me to the infectious<br />
causes of pericarditis. Most bacterial infections<br />
of the pericardium are fulminant, result in<br />
small effusions, and are rapidly fatal. They are usually<br />
caused by common bacteria such as staphylococcus,<br />
streptococcus, Escherichia coli, salmonella,<br />
and Neisseria meningitidis, and most will be evident<br />
on Gram’s staining and will grow in culture. This<br />
patient started taking levofloxacin just before the<br />
pericardiocentesis was performed, and this drug<br />
could have interfered <strong>with</strong> growth in culture, although<br />
on staining, purulent fluid and organisms<br />
The New England Journal of Medicine<br />
Downloaded from nejm.org by LOKESH VUYYURU on February <strong>22</strong>, 2012. For personal use only. No other uses <strong>with</strong>out permission.<br />
Copyright © <strong>2004</strong> Massachusetts Medical Society. All rights reserved.