

Integrating IMCI & ETAT Guidelines Presentation - INMED
Integrating IMCI & ETAT Guidelines Presentation - INMED
Integrating IMCI & ETAT Guidelines Presentation - INMED

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
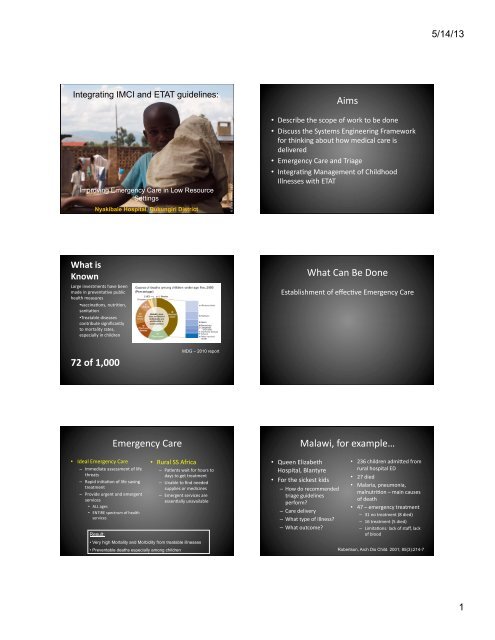
<strong>Integrating</strong> <strong>IMCI</strong> and <strong>ETAT</strong> guidelines:<br />
Improving Emergency Care in Low Resource<br />
GECC<br />
Settings<br />
Bisanzo,<br />
Nyakibale Hospital, Rukungiri District Sheila ©<br />
What is<br />
Known<br />
Large investments have been<br />
made in preventa@ve public<br />
health measures<br />
• vaccina@ons, nutri@on,<br />
sanita@on<br />
• Treatable diseases<br />
contribute significantly<br />
to mortality rates,<br />
especially in children<br />
72 of 1,000<br />
• Ideal Emergency Care<br />
– Immediate assessment of life<br />
threats<br />
– Rapid ini@a@on of life saving<br />
treatment<br />
– Provide urgent and emergent<br />
services<br />
• ALL ages<br />
• ENTIRE spectrum of health<br />
services<br />
Result:<br />
Emergency Care<br />
MDG – 2010 report<br />
• Rural SS Africa<br />
– Pa@ents wait for hours to<br />
days to get treatment<br />
– Unable to find needed<br />
supplies or medicines<br />
– Emergent services are<br />
essen@ally unavailable<br />
• Very high Mortality and Morbidity from treatable illnesses<br />
• Preventable deaths especially among children<br />
Aims<br />
• Describe the scope of work to be done<br />
• Discuss the Systems Engineering Framework<br />
for thinking about how medical care is<br />
delivered<br />
• Emergency Care and Triage<br />
• Integra@ng Management of Childhood<br />
Illnesses with <strong>ETAT</strong><br />
What Can Be Done<br />
Establishment of effec@ve Emergency Care<br />
Malawi, for example…<br />
• Queen Elizabeth<br />
Hospital, Blantyre<br />
• For the sickest kids<br />
– How do recommended<br />
triage guidelines<br />
perform?<br />
– Care delivery<br />
– What type of illness?<br />
– What outcome?<br />
• 236 children admiUed from<br />
rural hospital ED<br />
• 27 died<br />
• Malaria, pneumonia,<br />
malnutri@on – main causes<br />
of death<br />
• 47 – emergency treatment<br />
– 31 no treatment (8 died)<br />
– 16 treatment (5 died)<br />
– Limita@ons: lack of staff, lack<br />
of blood<br />
Robertson, Arch Dis Child. 2001; 85(3):214-7<br />
5/14/13<br />
1
A Model of Healthcare<br />
Carayon, P., Alvarado, C., Brennan, P., Gurses, A., Hundt, A., Karsh, B., and<br />
Smith, M., (2003). Work system and patient safety. Proceedings of Human<br />
Factors in Organizational Design and Management-VII 583-588.<br />
Nyakibale Hospital<br />
Resources -‐ People<br />
© Paul Bauer, MDA<br />
• Doctor: Popula@on Ra@o in Rukungiri<br />
– 1:18,500<br />
• Mid-‐Level Provider (equivalent to PA):<br />
Popula@on Ra@o in Rukungiri<br />
– 1:13,500<br />
• Nurse: Popula@on Ra@o in Rukungiri<br />
– 1:895<br />
Nyakibale Hospital<br />
Environment -‐ Emergency<br />
Department<br />
ED Tasks<br />
Holding area from outpa@ent<br />
department prior to<br />
admission<br />
No Triage system<br />
Other Elements<br />
© Sheila Bisanzo, GECC<br />
ED Tools and Technology<br />
Broken Imaging<br />
Laboratory oriented toward<br />
Outpa@ent care<br />
Supplies – what supplies?<br />
5/14/13<br />
2
<strong>ETAT</strong> designed for…<br />
• High admission mortality rates<br />
• Delays in care<br />
• Lack of triage system<br />
• Integra@on with trea@ng childhood illnesses<br />
What does teaching <strong>ETAT</strong> look like?<br />
• 7 Modules<br />
• 3.5 days<br />
• Instructor and Course<br />
book<br />
– Recommended Timeline<br />
– Resources<br />
– Equipment lists<br />
– Tests<br />
• Material from Integrated<br />
Management of<br />
Childhood Illnessses<br />
• 7 modules<br />
– Triage and “ABCD”<br />
– Airway and Breathing<br />
– Circula@on<br />
– Coma and Convulsion<br />
– Dehydra@on<br />
– Case Management<br />
Scenarios<br />
– Implemen@ng <strong>ETAT</strong><br />
Is Implemen@ng <strong>ETAT</strong> effec@ve?<br />
• Adapted <strong>ETAT</strong> at Red<br />
Cross War Memorial<br />
– “Two armed descrip@ve<br />
study” – <strong>ETAT</strong> alone<br />
– Triage data,<br />
retrospec@ve, Oct 2007<br />
to July 2009<br />
– 1309 records<br />
– 3 categories<br />
• Emergency, Urgent, Non-‐<br />
Urgent<br />
Oct 2007 AdmiAed<br />
3.8% (34) 52.9% (18)<br />
37.5% (338) 32.5% (110)<br />
58.8% (530) < 10% (52)<br />
Oct July 2009 AdmiAed<br />
2.9% (12) 91.7% (11)<br />
45.9% (187) 36.9% (69)<br />
51.1% (208) 10% (21)<br />
Buys et al., S Afr Med J. 2012 Dec 31;103(3):161-5<br />
What does teaching <strong>ETAT</strong> look like?<br />
• Module based educa@on – flexible @meframe<br />
• Cross-‐discipline training<br />
<strong>ETAT</strong> course Emergency Triage only<br />
ED staff Watchmen<br />
Pediatricians and surgeons Gate Keepers<br />
On call physicians Administra@ve Staff<br />
Health professions teachers Driver<br />
• Meant to impact en@re hospital!<br />
Is teaching <strong>ETAT</strong> effec@ve?<br />
• Pediatric Resuscita@on<br />
for nurses working in<br />
Ghana<br />
• 1 day of <strong>ETAT</strong> training<br />
• Self-‐Efficacy, Ghanaian<br />
hospital nurses<br />
• Before and aoer design,<br />
focusing on self-‐efficacy<br />
– Survey<br />
• Increase for<br />
– Resuscita@on in general<br />
– Bag-‐Mask Ven@la@on<br />
– Knowledge of Paediatric<br />
Resuscita@on<br />
• Recommenda@ons:<br />
– More Teaching with a<br />
focus on nurses<br />
Brennan et al, Int Nurs Rev. 2013 Mar;60(1):136-43.<br />
What does <strong>ETAT</strong> cost?<br />
• District Hospital Implementa@on of <strong>ETAT</strong> in Kenya<br />
• Cost analysis with outcomes data<br />
• 4 district hospitals -‐ full <strong>ETAT</strong> training vs 4 hospitals -‐ par@al training<br />
• 14 process measures to follow quality<br />
Category IntervenGon control<br />
Cost/admission (2009 $) 50.74 31.1<br />
• Improvement in quality (key indicators – actuarial math…): US$0.79 per<br />
% increase in care<br />
• Es@mated cost to na@onal health care system?<br />
– 3.6 million, $39.8 -‐ $398/disability adjusted life year (DALY)<br />
Barasa, PLoS Med. 2012;9(6):e1001238<br />
5/14/13<br />
4
Does <strong>ETAT</strong> improve performance?<br />
• KenyaUa Na@onal<br />
Hospital, Nairobi<br />
• Before-‐aoer study<br />
• 2005 vs. 2009<br />
• <strong>ETAT</strong> and <strong>IMCI</strong><br />
• Guideline adherence:<br />
– Pneumonia, dehydra@on,<br />
severe malnutri@on<br />
– Assessment, classifica@on,<br />
treatment, and follow-‐up<br />
care<br />
Irimu et al., PLoS One. 2012; 7(7): e39964.<br />
Integrated Management of<br />
Childhood Illnesses<br />
• Aims:<br />
– Improving case<br />
management skills of<br />
health-‐care staff<br />
– Improving overall health<br />
systems<br />
– Improving family and<br />
community health<br />
prac@ces.<br />
• Mul@ple condi@ons<br />
working together to<br />
increase risk for children<br />
• Macro to Micro<br />
approach<br />
– Health policy<br />
– Hospital organiza@on<br />
– Ward personel<br />
– Front line clinic workers<br />
• Evaluated in many<br />
countries<br />
Integra@ng <strong>ETAT</strong> and <strong>IMCI</strong><br />
http://www.who.int/maternal_child_adolescent/documents/9241546700/en/<br />
Does <strong>ETAT</strong> improve performance?<br />
Treatment 2005 2009 Significance<br />
Dose and Frequency<br />
of Penicillin<br />
Fluid Resuscita@on<br />
<strong>ETAT</strong>+ guidelines<br />
Feeds for severe<br />
malnutri@on<br />
137/265 (51.7%;<br />
45.5–57.9)<br />
100/265 (37.7%;<br />
31.9–43.9)<br />
25/274 (9.1%; 6.0–<br />
13.2)<br />
258/287 (89.9%;<br />
85.8–93.1)<br />
177/286 (61.8%;<br />
60.0–67.5)<br />
135/197 (68.5%;<br />
61.5–74.9)<br />
+38.2%<br />
+24.2%<br />
+59.5%<br />
Outcome 2005 2009 Rela@ve Significance<br />
Mortality with<br />
pneumonia<br />
Mortality from<br />
shock<br />
Mortality with<br />
malnutri@on<br />
40/265 (15.1%) 19/293 (6.5%) -‐57%<br />
53/297 (17.9%) 26/294 (8.8%) -‐51%<br />
82/284 (29.9%) 44/197 (22.3%) -‐25%<br />
Irimu et al., PLoS One. 2012; 7(7): e39964.<br />
<strong>IMCI</strong> course by district density<br />
Case #1<br />
• A 5 week old male presents with a fever. Mother reports<br />
uncomplicated delivery in the village. Child was well un@l this<br />
morning when mother noted he would not feed. No cough<br />
• PE: 34.8 170 52 92% on room air<br />
Gen: Difficult to arouse<br />
HEENT: normal scalp, fontanelle, no rhinorrhea, MMM, not pale<br />
Neck: supple, no masses<br />
Chest: clear to asculta@on<br />
Heart: tachy, no murmur<br />
Abd: soo, non-‐tender. Umbilicus appears normal other then reducible<br />
umbilical hernia<br />
Ext: no edema<br />
Skin: no rash, cool to touch<br />
Neuro: sleeping, poor muscle tone<br />
5/14/13<br />
5
Case #1<br />
• What immediate treatment and work-‐up does<br />
this child need?<br />
• Does the child need an LP? Why or why not?<br />
• Would you give an@bio@cs to this child once<br />
you place the cannula?<br />
• Would give an@bio@cs if the child has a<br />
posi@ve BS?<br />
Emergency Signs<br />
• Airway<br />
– Obstructed Breathing<br />
• Breathing<br />
– Severe respiratory distress<br />
– Central cyanosis<br />
• Circula@on<br />
These children<br />
need to be treated<br />
immediately to<br />
avert death<br />
– Signs of shock (cold hands; capillary refill longer than<br />
3 seconds, weak, fast pulse, signs of severe<br />
dehydra@on in a child with diarrhea)<br />
• Disability<br />
– Coma, Convulsions<br />
Emergency Signs<br />
Airway and Breathing<br />
• Necessitate immediate treatment, call for<br />
help, blood draw (glucose, malaria smear,<br />
hemoglobin)<br />
Assess Treat<br />
Airway and Breathing Manage airway<br />
Obstruc@on<br />
ANY SIGN POSITIVE<br />
Neck injury?<br />
Cyanosis Choking?<br />
Severe respiratory distress Oxygen<br />
Warm child<br />
Stages in the management of the sick<br />
child admiUed to hospital: summary of<br />
key elements<br />
• Check for emergency<br />
signs, assess ABC’s<br />
• If emergency signs<br />
found,<br />
– Call for help<br />
– Start treatment<br />
– Stay calm<br />
– Work as a team<br />
Ini@al Evalua@on<br />
Developed from WHO Pocket book<br />
of Hospital Care for Children<br />
• Emergency<br />
inves@ga@ons:<br />
– Blood glucose<br />
– Blood smear<br />
– Hemoglobin<br />
– Type and cross-‐match?<br />
• Shock, anemia, bleeding<br />
Emergency Signs -‐ Circula@on<br />
Assess Treat<br />
CirculaGon ANY SIGN POSITIVE<br />
Support circulaGon<br />
Cold hands with Stop bleeding<br />
Delayed capillary refill Give Oxygen<br />
Weak and fast pulse Warm child<br />
Not malnourished<br />
Place IV,<br />
intraosseus, or<br />
external jugular<br />
line<br />
Malnourished<br />
Give IV glucose<br />
Place IV and give<br />
fluids<br />
5/14/13<br />
6
Emergency Signs: Neurologic Disability<br />
Assess Treat<br />
Coma/convulsing Manage airway (mind<br />
neck injury)<br />
Coma or<br />
IF COMA OR<br />
CONVULSING<br />
Check RBS – IV glucose<br />
if low<br />
Convulsing (now) Posi@on unconscious<br />
child to avoid<br />
aspira@on<br />
Priority signs<br />
Convulsion = diazepam<br />
rectally<br />
• Need prompt assessment<br />
• No wai@ng in queue – move to the front<br />
• Get surgical help as needed<br />
Priority Signs<br />
Assess<br />
Severe DehydraGon in<br />
presence of diarrhoea<br />
Emergency Signs<br />
Severe Dehydra@on<br />
DIARRHEOA plus<br />
Treat<br />
Not malnourished<br />
Lethargy<br />
TWO SIGNS<br />
POSITIVE<br />
Start IV and rapid<br />
IV fluids<br />
Sunken eyes Check for severe Severely malnourished<br />
Very slow skin pinch malnutriCon Do NOT start IV<br />
Proceed to full<br />
assessment and<br />
treatment<br />
Priority Signs – give pa@ents urgent<br />
aUen@on<br />
• Tiny Baby: sick child<br />
under 2 months<br />
• Temperature: > 39 C<br />
• Trauma or other urgent<br />
surgical condi@on<br />
• Pallor (severe)<br />
• Poisoning<br />
• Pain (severe)<br />
• Respiratory distress<br />
• Restless or lethargic<br />
• Referral (urgent)<br />
• Malnutri@on with<br />
severe was@ng<br />
• Oedema of both feet<br />
• Burns (major)<br />
3TPR MOB<br />
The Young Child with a Fever<br />
5/14/13<br />
7
Fever work-‐up<br />
• What are the causes of fever in young<br />
children?<br />
– Meningi@s – bacterial, viral, fungal<br />
– Pneumonia – bacterial, viral<br />
– Malaria<br />
– Sepsis (bacteremia) – blood infec@on<br />
– Urinary Tract infec@on -‐ bacterial<br />
– Viral infec@ons<br />
The Ill Neonate (< 2 months)<br />
• ABC’s<br />
• History<br />
– Focus on birth history<br />
– Ask mother if history of genital herpes?<br />
– Full term? Prolonged labor/rupture of membranes?<br />
Forceps delivery? Maternal fever during delivery<br />
• Exam –<br />
– Examine scalp for abrasions/sings of infec@on<br />
– Fontanelle exam<br />
– Umbilicus<br />
– Gums – for evidence of false teeth extrac@on<br />
– Rash – herpes, petechiae, pustules<br />
Neonate with Fever: Treatment<br />
• Fluid bolus with NS or LR (preferred if diarrhea)<br />
– 20 mL/kg, repeat aoer re-‐evalua@on<br />
– Severe Anemia (Hb< 5 g/dL) given 10-‐20 mL/kg whole<br />
blood<br />
– If not responding, call doctor<br />
• An@bio@cs – regardless of results of tes@ng<br />
– Ampicillin 50 mg/kg; Gentamicin 7.5 mg/kg<br />
• Give Acyclovir is mother has genital herpes<br />
• An@malarials if BS is posi@ve or suspect par@ally<br />
treated malaria<br />
Why are young children different?<br />
• Physiology<br />
– Immune system of newborn not func@onal un@l 2-‐4<br />
months of age<br />
– Unable to communicate symptoms<br />
– Exam is unreliable (lacks sensi@vity) to localize<br />
symptoms<br />
– Observa@ons other than heart rate remain normal<br />
un@l child is close to death<br />
– Some@mes poor PO in take is only sign of illness<br />
• Immuniza@ons<br />
– Have not completed full course<br />
Neonate with Fever: Work-‐up<br />
• Place IV, BS, RBS, Hgb,<br />
– LP for CSF workup is MANDATORY regardless of results<br />
of other tes@ng<br />
– Consider CXR if sat < 94, grun@ng, focal abnormal<br />
breath sounds, tachypnea, or chest indrawing.<br />
– Consider Urine analysis if no source for fever, and LP<br />
nega@ve<br />
– Consider Rapid An@body Test in mother if HIV<br />
unknown<br />
• Re-‐assess observa@ons frequently (15-‐20<br />
minutes)<br />
Case #1<br />
• What treatment and work-‐up does this child<br />
need?<br />
• Does the child need an LP? Why or why not?<br />
• Would you give an@bio@cs to this child once<br />
you place the cannula?<br />
• Would give an@bio@cs if the child has a<br />
posi@ve BS?<br />
5/14/13<br />
8
Case #1<br />
• What work-‐up does this child need?<br />
IV, Bolus, LP, BS, RBS, Chest x-‐ray<br />
• Does the child need an LP? Why or why not?<br />
YES – immune system is s@ll weak, PE is unreliable<br />
• Would you give an@bio@cs to this child once you<br />
place the cannula?<br />
YES – give Ampicillin and Gentamicin<br />
• Would give an@bio@cs if the child has a posi@ve<br />
BS?<br />
YES<br />
Case #2<br />
• What work-‐up does this child need?<br />
• Does the child need an LP? Why or why not?<br />
• Would you give an@bio@cs to this child once<br />
you place the cannula?<br />
• Would give an@bio@cs if the child has a<br />
posi@ve BS?<br />
Child < 1 year with Fever: Work-‐up<br />
• Place IV, BS, RBS, Hgb,<br />
– LP for CSF workup is MANDATORY if no immuniza@ons<br />
– LP for CSF is MANDATORY if child is ill-‐appearing<br />
– Consider CXR if sat < 94, grun@ng, focal abnormal<br />
breath sounds, tachypnea, or chest indrawing.<br />
– Consider Urine analysis if no source for fever, and LP<br />
nega@ve<br />
• Re-‐assess observa@ons frequently (15-‐20<br />
minutes)<br />
Case #2<br />
• A 6 month old female presents to the ED with a fever. Mother<br />
reports child well un@l this morning. She developed fever and<br />
vomi@ng, that was not bloody. She has no diarrhea or cough. She<br />
is up to date on her immuniza@ons<br />
• PE 38.4 136 80/50 38 95%<br />
Gen: Awake, looks at you when you approach mother<br />
HEENT: MMM, NC, fontanelle flat, + rhinorrhea, OP is clear<br />
Neck: supple<br />
Chest: clear bilaterally<br />
Heart: tachycardic, no murmur<br />
Abd: soo, non-‐tender<br />
Ext: no edema<br />
Skin: no rash, hair appears normal<br />
Neuro: awake, interac@ve, smiles when you play with her.<br />
Child less then 1 year with fever<br />
• ABC’s<br />
• History:<br />
– Immuniza@ons<br />
– Signs and Symptoms are more reliable the older<br />
the child<br />
– Malnutri@on (can suppress immune response to<br />
bacterial infec@on<br />
Child < 1 year with Fever: Treatment<br />
• If tachycardia, fluid bolus with NS or LR (preferred if<br />
diarrhea)<br />
– 20 mL/kg, repeat aoer re-‐evalua@on<br />
– Severe Anemia (Hb< 5 g/dL) given 10-‐20 mL/kg whole<br />
blood<br />
– If not responding, call doctor<br />
• An@bio@cs only if bacterial focus found<br />
– Ceoriaxone 50-‐100 mg/kg daily (Meningi@s?)<br />
– Mandatory if child is toxic looking or severely<br />
malnourished<br />
• An@malarials if BS is posi@ve or suspect par@ally<br />
treated malaria<br />
5/14/13<br />
9
Case #2<br />
• What work-‐up does this child need?<br />
• Does the child need an LP? Why or why not?<br />
• Would you give an@bio@cs to this child once<br />
you place the cannula?<br />
• Would give an@bio@cs if the child has a<br />
posi@ve BS?<br />
Case #3<br />
• An 8 month old female presents with difficulty in breathing.<br />
Mother noted cough and “flu” symptoms for 1 day. She has<br />
also been having trouble breathing that seems to be ge|ng<br />
worse. Has had trouble breast feeding this aoernoon<br />
PE 38.7 122 80/40 36 90%<br />
Gen: crying, irritable child<br />
HEENT: NC/AT, MMM<br />
Neck without mass<br />
Chest with crackles in the base, subcostal recessions<br />
Hyperdynamic precordium, no murmur, cool hands and feet<br />
Absomen distended, nontender, spleen @p palpable<br />
Feet with oedema, and scaly rash over extremi@es<br />
Hair is red and patchy<br />
Assessment of the severely<br />
malnourished child<br />
• History:<br />
– Mother with ISS, Child living with grandmother<br />
– Cessa@on of breast feeding before 1 yr<br />
– No meat or beans in diet<br />
• Exam:<br />
– Observa@ons, may be hypothermic (elevated heart<br />
rate if dehydrated)<br />
– AUen@on to height, weight<br />
– AUen@on to skin, hair, extremi@es (oedema and rash)<br />
Case #2<br />
• What work-‐up does this child need?<br />
BS, other tests only if BS nega@ve or suspicion for other<br />
pathology arises<br />
• Does the child need an LP? Why or why not?<br />
No, well appearing and fully immunized<br />
• Would you give an@bio@cs to this child once you place<br />
the cannula?<br />
No, child is well appearing<br />
• Would give an@bio@cs if the child has a posi@ve BS?<br />
No, child is well appearing<br />
Approach to the Severely<br />
Malnourished Child<br />
• Diagnosis<br />
– Weight for length < 70% or < -‐3SD (see WHO<br />
pocket book on Hospital Care for Children,<br />
appendix 5, p 359)<br />
– Oedema of both feet (Kwashiorkor – edema from<br />
low albumin)<br />
– Visible was@ng (Merasmus – muscle atrophy from<br />
low protein intake)<br />
– Red or light brown hair, derma@@s<br />
– Developmental delay or developmental regression<br />
Malnourished Child – Work Up<br />
• RCT, RBS, Hgb, BS<br />
• Indica@ons for LP:<br />
– Persistent vomi|ng<br />
– Convulsions<br />
– Temperature instability (T > 38 or T < 35)<br />
– Cranial nerve abnormali@es (disconjugate gaze,<br />
facial palsy)<br />
– New confusions or lethargy<br />
• CXR if signs or symptoms of pneumonia<br />
5/14/13<br />
10
Malnourished Child -‐ Treatment<br />
• Careful fluid administra@on if dehydrated<br />
(10-‐20 ml/kg with observa@ons)<br />
– Concern for conges@ve cardiac failure due to<br />
chronic malnutri@on<br />
– NS or LR are both acceptable<br />
• An@bio@cs for any child mee@ng criteria for<br />
severe malnutri@on<br />
• An@malarials if BS posi@ve or suspicion for<br />
par@ally treated malaria<br />
Case #3<br />
• What work-‐up does this child need?<br />
• Does the child need an LP? Why or why not?<br />
• Would you give an@bio@cs to this child once<br />
you place the cannula?<br />
• Would give an@bio@cs if the child has a<br />
posi@ve BS?<br />
Summary of <strong>ETAT</strong><br />
• Triage – Check for Emergency signs! <br />
determines pa@ent flow (Airway, Breathing,<br />
Circula@on, Coma, Convulsion, Dehydra@on)<br />
• Emergency<br />
• Priority<br />
• Queue<br />
• Pay aUen@on to Priority Signs: 3PTR MOB<br />
• HIV status important in ill appearing children<br />
• Malnourished children < 1 yr may not show sings<br />
of infec@on when sep@c, treatment is similar to<br />
newborns<br />
Malnourished Child Admission<br />
Orders<br />
• All severely Malnourished children should get:<br />
– ORS to con@nue rehydra@on if dehydrated<br />
– 50-‐100 cc addi@onal ORS for every loose stool<br />
– Ceoriaxone 50 mg/kg<br />
– HEM (high energy milk)<br />
• 11 mL/kg every 2 hours<br />
– Vitamins<br />
• A dose varies with age<br />
• Folic Acid 5 mg on day one then 1 mg/day<br />
50,000 IU if < 6 mnth<br />
100,000 IU for 6-‐12 mnths<br />
200,000 IU if > 12 mnths<br />
• Magnesium 50 mg/Kg IV up to 1 gram total dose (to be<br />
given slowly over 2 hours)<br />
• Zinc: 2 mg/kg/day orally<br />
Case #3<br />
• What work-‐up does this child need?<br />
– RBS, BS, Hgb, LP, CXR, RCT<br />
• Does the child need an LP? Why or why not?<br />
– Yes. Two risk factors for meningi@s: Mother with ISS, and<br />
severe malnutri@on<br />
• Would you give an@bio@cs to this child once you place<br />
the cannula?<br />
– Yes, this pa@ent can hide an infec@on that is hard to no@ce<br />
on clinical exam because of severe malnutri@on<br />
• Would give an@bio@cs if the child has a posi@ve BS?<br />
– Yes, the child has severe malnutri@on.<br />
How to make this possible<br />
• AUen@on to Environment<br />
• People<br />
• Tasks<br />
• Tools and Technology<br />
• Follow the process measures Outcomes<br />
5/14/13<br />
11
Environment<br />
Partnership with GECC and<br />
MDA:<br />
Medicine Cabinet<br />
Surgical Lamps<br />
Privacy Curtains<br />
Triage desk<br />
Chart System<br />
Library<br />
Equipment steriliza@on © Sheila Bisanzo, GECC<br />
Comprehensive Emergency Care Training<br />
• Pediatric Emergencies and Malnutri@on Care<br />
• Commonly used procedures<br />
– Suturing<br />
– Lumbar Puncture<br />
– Seda@ons<br />
– I and D<br />
• Symptom based approach to major complaints<br />
• Trauma care<br />
• Consulta@ons to physicians<br />
– Major surgery (laparotomy)<br />
– Cri@cally ill and not responding to treatment<br />
Tools and<br />
Technology<br />
Do you have what you<br />
need to do your job?<br />
Supplies<br />
Diagnos@cs<br />
Therapeu@cs<br />
© Sheila Bisanzo, GECC<br />
People – the Emergency<br />
Nurse PracGGoners<br />
Intensive training<br />
Highly skilled<br />
Excellent outcomes<br />
Unmatched in Sub-‐Saharan<br />
Africa<br />
Ongoing mentorship to<br />
become leaders<br />
Mentorship to enable<br />
propaga@on of the model<br />
Tasks<br />
Effec@ve:<br />
Triage<br />
Assessment<br />
Treatment<br />
Disposi@on<br />
© Sheila Bisanzo, GECC<br />
© Sheila Bisanzo, GECC<br />
Effec@ve Integrated Emergency<br />
Care<br />
• Reduce morbidity and mortality from acute<br />
illness and injury<br />
• Triage of pa@ents<br />
– Pa@ents for rou@ne follow up or minor illness are seen in<br />
OPD<br />
– Sickest pa@ents sent to Emergency Department<br />
– Can be done by a Nursing Assistant<br />
• Maximizes efficiency of care<br />
– Cri@cally ill pa@ents not wai@ng in line<br />
– Sick pa@ents are resuscitated before going to the ward.<br />
5/14/13<br />
12
Is it Quality Care?<br />
• Beginning November 13 th , 2009<br />
– GECC volunteers help monitor care<br />
– 72 hour follow up on all pa@ents seen in the ED<br />
– Telephone calls to ED mentor with targeted ques@ons<br />
• As of February, 2010<br />
– 1828 pa@ents seen<br />
– 432 are children under 5<br />
– ~90% seen primarily by Ugandan trainees<br />
Comparison to other Data<br />
• Nyakibale ED: 2.12%<br />
• Mortality Rates in AdmiUed Children<br />
– 4.5% (Soweto, South Africa)<br />
– 5.7% (Mafikeng, South Africa)<br />
– 9.9% (Siaya, Kenya)<br />
– 13.7% (Bissau, Guinea)<br />
– 17.4% (Lwiro, South Kivo, DRC)<br />
Sustainable Emergency Care<br />
• Operate the ED 24 hours a day<br />
• Eventually expand the training program ?<br />
– Establish Emergency Care at other District<br />
Hospitals<br />
– Scaleable to other countries?<br />
• What do we need?<br />
– Enthusias@c physicians with desire to mentor!<br />
– Volunteers with adult educa@on skills<br />
Results<br />
• Pa@ents under 5 years (432)<br />
– 330 admiUed<br />
– 199 had malaria (174 admiUed)<br />
– 105 had malnutri@on (104 admiUed)<br />
• Mortality in pa@ents under 5:<br />
– AdmiUed: 7 pa@ents (2.12%) *<br />
– AdmiUed with malaria: 1 (0.57%)**<br />
– AdmiUed with malnutri@on: 3 (2.88%)<br />
Where do we go from here? © Sheila Bisanzo, GECC<br />
© Sheila Bisanzo, GECC<br />
5/14/13<br />
13
© Paul Bauer, MDA<br />
Global Emergency Care<br />
Collabora@ve<br />
hUp://www.globalemergencycare.org/<br />
Partners<br />
Mission Doctors<br />
Associa@on<br />
hUp://missiondoctors.org/<br />
5/14/13<br />
14